Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
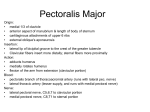
n Case Report Atypical Pectoralis Major Muscle Wasting in a Recreational Weight Lifter Nata Parnes, MD; Maryellen I. Blevins, PA-C, MPAS; Paul Carey, MD; Darren J. Friedman, MD abstract Pectoralis major injuries are relatively uncommon and can pose a diagnostic challenge. Deformity and weakness of this muscle in weight lifters is typically due to traumatic tendon rupture and often requires surgical repair. However, there are other less common etiologies that can mimic the clinical presentation of pectoralis major wasting and weakness that require different treatment approaches. This article describes a case of a 48-year-old recreational weight lifter who presented with severe pectoralis major wasting and weakness secondary to isolated mononeuropathy of the lateral pectoral nerve possibly due to Parsonage Turner syndrome. The patient was treated nonoperatively and achieved full recovery 18 months after onset. Parsonage Turner syndrome should be included in the differential diagnosis of patients with atraumatic weakness and wasting of the pectoralis major muscle and dysfunction. [Orthopedics. 2016; 39(4):e756-e759.] T he pectoralis major is the largest and most powerful muscle of the chest. It is composed of 3 distinct segments: clavicular, sternal, and sternoabdominal. It has an important role in forward flexion, adduction, and internal rotation of the shoulder. The most widely described pectoralis major injury in weight lifters is tendon rupture from the humeral insertion secondary to eccentric contraction. Pectoralis major injury can cause pain, weakness, deformity, and muscle wasting. This injury usually requires surgical repair to restore strength and fatigue resistance.1 However, other e756 less common pathologies can cause similar clinical presentations. These conditions require different modalities of treatment and should be recognized. This article describes a unique case in a recreational weight lifter who presented with pectoralis major wasting secondary to isolated involvement of the lateral pectoral nerve likely due to Parsonage Turner syndrome. Case Report A 48-year-old male recreational weight lifter presented with sudden onset of pain in his right shoulder after routine workout activities. There was no history of trauma, malignancy, changes in workout routine, prior shoulder or neck surgeries, cervical spine disease, or viral disease. The patient reported that the pain began after his daily weight lifting routine and subsided after 3 weeks. A few weeks after resolution of the pain, severe shoulder weakness developed. The patient presented to the authors’ clinic 3 months after the initial onset of symptoms. Physical examination of the right shoulder girdle revealed wasting of the pectoralis major muscle with associated weakness in horizontal adduction and internal rotation of the shoulder (Figure 1). Horizontal adduction pectoralis major muscle strength was rated as 3+ out of 5 The authors are from the Department of Orthopaedic Surgery (NP, MIB), Carthage Area Hospital, Carthage; the Department of Orthopaedic Surgery (PC), Fort Drum; and the Department of Orthopaedic Surgery (DJF), New York Presbyterian Lower Manhattan Hospital, New York, New York. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Darren J. Friedman, MD, Department of Orthopaedic Surgery, New York Presbyterian Lower Manhattan Hospital, 170 William St, New York, NY 10038 ([email protected]). Received: July 9, 2015; Accepted: August 7, 2015. doi: 10.3928/01477447-20160526-09 Copyright © SLACK Incorporated n Case Report (5=normal). Active range of motion of the right shoulder was full and symmetric with the contralateral extremity. All of the other muscles of the right shoulder girdle and right upper extremity were found to be of normal strength (5 out of 5) without any visualized atrophy. Sensory and vascular examination of the right upper extremity were normal. Magnetic resonance imaging (MRI) of the cervical spine, brachial plexus, shoulder, and chest was performed 3 months after the onset of symptoms. Magnetic resonance imaging of the chest revealed intramuscular edema and muscular atrophy of the pectoralis major without fatty infiltration (Figure 2). Electromyography (EMG) of the right upper extremity performed 3 months after the onset of symptoms revealed fibrillations and positive sharp waves with reduced recruitment of the upper two-thirds of the pectoralis major consistent with mononeuropathy of the lateral pectoral nerve likely secondary to Parsonage Turner syndrome. No other neurologic abnormalities were identified. Nerve conduction study of the right upper extremity performed at the same time was normal. Based on the history, examination, and diagnostic studies, the diagnosis of likely Parsonage Turner syndrome was made. Treatment included reassurance, physical therapy including active and passive range of motion exercises, eventual strengthening exercises of the pectoralis major muscle, and analgesics as necessary. Nine months after the onset of symptoms, the patient reported significant subjective improvement. Physical examination revealed decreased muscle atrophy with improved pectoralis muscle strength (4 out of 5). Follow-up EMG of the right upper extremity 6 months after the initial EMG demonstrated interval improvement. Eighteen months after the onset of symptoms, the patient reported full recovery with no residual pain or weakness. He had returned to his baseline activity with full function, including bench JULY/AUGUST 2016 | Volume 39 • Number 4 Figure 1: Photograph showing wasting of the pectoralis major muscle at presentation. press and weight lifting. Visual analog pain scale was 0 out of 10, and his right subjective shoulder value was 100% of normal. Physical examination revealed normal muscle bulk of the pectoralis major muscle that was symmetric with the contralateral side (Figure 3). Pectoralis major muscle strength was symmetric and 5 out of 5 bilaterally. Discussion The pectoralis major muscle is a large fan-shaped muscle composed of 3 heads: clavicular, sternal, and sternoabdominal. It is innervated by both the lateral pectoral nerve, which branches off the lateral cord of the brachial plexus and receives innervation from the C5-C6 nerve roots, and the medial pectoral nerve, which branches off the medial cord of the brachial plexus and receives innervation from the C7-C8 and T1 nerve roots.2 The lateral pectoral nerve runs along the medial aspect of the pectoralis minor muscle and then along the A Figure 2: T2-weighted axial magnetic resonance image showing intramuscular edema and muscular atrophy without fatty infiltration of the pectoralis major muscle. undersurface of the pectoralis major muscle along with the pectoral branch of the thoracoacromial artery, supplying roughly the upper two-thirds of the pectoralis major muscle. The medial pectoral nerve pierces the pectoralis minor muscle and then runs along its lower border to supply the lower one-third of the pectoralis major muscle. The lateral pectoral nerve is larger in size compared to the medial pectoral nerve, innervating a greater percentage of the pectoralis major muscle.3 The pectoralis major is an important contributor to the shoulder’s internal rotation, adduction, and forward flexion. The most commonly reported pectoralis major injury in weight lifters is tendon rupture from the humeral insertion, which usually is an acute well-defined injury characterized by immediate pain, diminished ante- B Figure 3: Coronal (A) and sagittal (B) photographs 18 months after presentation showing no residual wasting of the pectoralis major muscle. e757 n Case Report rior axillary fold, weak horizontal adduction, and cosmetic deformity that includes bulging at the origin of the muscle on the medial aspect of the chest accompanied by typical defect at the lateral aspect of the anterior chest wall. In cases of complete or high-grade partial tears, surgical anatomic repair generally is advised to restore function, improve cosmesis, and increase overall patient satisfaction compared to nonsurgical treatment.1 The current case lacked the history and characteristic findings of acute tendon tear, leading the authors to investigate less common etiologies for pectoralis major wasting such as cervical radiculopathy,4 tumor of the spinal cord or brachial plexus,5 peripheral nerve injury,4,6 or amyotrophic lateral sclerosis. The history of sudden onset of intense pain with no inciting trauma that improved spontaneously and was followed by weakness and muscle atrophy suggested Parsonage Turner syndrome. In addition, MRI studies of the C-spine, brachial plexus, shoulder, and chest ruled out structural abnormality. Diagnosis was confirmed on EMG, which established isolated mononeuropathy of the lateral pectoral nerve likely due to Parsonage Turner syndrome. Parsonage Turner syndrome is a rare syndrome of unknown etiology with an incidence of less than 2 in 100,000.7 It affects men more than women, with occurrence reports ranging from 2:1 to 12:1. In one-third of cases, it occurs bilaterally. The etiology of Parsonage Turner syndrome is still unclear7 with factors proposed to be: recent immunization,8 recent surgery in remote area of the body,9 trauma,10 infection,11 and autoimmune disease.12 The typical presentation of Parsonage Turner syndrome is acute severe pain in the neck, shoulder, and arm that resolves spontaneously in a few weeks, followed by weakness and atrophy affecting muscles around the shoulder region. Parsonage Turner syndrome most commonly presents as a global plexopathy, with iso- e758 lated involvement of a nerve branch being less common.7 However, several cases of single phrenic nerve involvement,13 anterior interosseous nerve involvement,12 and involvement of the anterior branch of the axillary nerve14 have been described. To the best of the authors’ knowledge, this is the first published report of isolated involvement of the lateral pectoral nerve. The results of basic laboratory investigations (complete blood test, erythrocyte sedimentation rate, and antiviral antibodies), as in this case, typically are normal in Parsonage Turner syndrome. MRI findings of an affected muscle or muscles in Parsonage Turner syndrome is nonspecific and defined as features of denervation involving muscles of the shoulder girdle and upper extremity, including intramuscular edema, muscular atrophy with or without fatty infiltration, or a combination of these findings.5 In the current case, there was evidence on the MRI of pectoralis major intramuscular edema and muscular atrophy without fatty infiltration. Electrodiagnostic studies can aid in confirming the diagnosis of Parsonage Turner syndrome, with changes often found 3 weeks or more after the onset of symptoms.7 In this case, EMG of the pectoralis major muscle demonstrated fibrillations and positive sharp waves with reduced recruitment of the upper two-thirds consistent with lateral pectoral nerve involvement. Normal motor unit potentials were recorded at all other muscles of the right upper extremity. Most Parsonage Turner syndrome patients have normal nerve conduction studies.15 Overall, Parsonage Turner syndrome is a self-limiting condition, with the mainstay of treatment being supportive. In their review of 99 patients, Tsairis et al16 found no significant benefit for patients who had a course of corticosteroids. They also found that physical therapy did not appear to improve time to functional recovery. Provision of adequate analgesia during the initial phase of this condition is recommended with no substantial sup- portive evidence for the use of other modalities such as massage, ultrasound, or electrical stimulation therapy. Prognosis is favorable with an estimated 75% of all patients making a complete recovery within 2 years and approximately 90% demonstrating complete recovery in 3 years.16 Conclusion Mononeuropathy and Parsonage Turner syndrome must be included in the differential diagnosis of patients with weakness, wasting of the pectoralis major muscle, and shoulder girdle pain, along with neuropathic muscular changes on MRI. Atraumatic history must raise suspicion, with EMG of the affected extremity confirming diagnosis. Conservative treatment of pectoral nerve palsy secondary to Parsonage Turner syndrome has a favorable outcome but can take 2 to 3 years for full recovery. References 1. Butt U, Mehta S, Funk L, Monga P. Pectoralis major ruptures: a review of current management. J Shoulder Elbow Surg. 2015; 24(4):655-662. 2. Provencher MT, Handfield K, Boniquit NT, Reiff SN, Sekiya JK, Romeo AA. Injuries to the pectoralis major muscle: diagnosis and management. Am J Sports Med. 2010; 38(8):1693-1705. 3. Prakash KG, Saniya K. Anatomical study of pectoral nerves and its implications in surgery. J Clin Diagn Res. 2014; 8(7):AC01AC05. 4. Aktas I, Palamar D, Akgun K. Lateral pectoral nerve injury mimicking cervical radiculopathy. Clin J Sport Med. 2015; 25(4):e64-e66. 5. Gupta A, Winalski CS, Sundaram M. Neuralgic amyotrophy (Parsonage Turner syndrome). Orthopedics. 2014; 37(2):75, 130133. 6. Gardetto A, Thaler C, Kiechl S, Maurer H, Piza-Katzer H. Isolated compression of the pectoral nerve resulting in atrophy of the major pectoral muscle. Muscle Nerve. 2003; 28(6):760-763. 7. Tjoumakaris FP, Anakwenze OA, Kancherla V, Pulos N. Neuralgic amyotrophy (Parsonage-Turner syndrome). J Am Acad Orthop Surg. 2012; 20(7):443-449. 8. Taras JS, Donohue KW. Radial nerve motor palsy following seasonal influenza vaccination: a case report. J Surg Orthop Adv. 2014; Copyright © SLACK Incorporated n Case Report 23(1):42-44. 9. Verhasselt S, Schelfaut S, Bataillie F, Moke L. Postsurgical Parsonage-Turner syndrome: a challenging diagnosis. Acta Orthop Belg. 2013; 79(1):20-24. 10. Zhao JC, Xian CJ, Yu JA. Parsonage-Turner syndrome in second-degree contact burns. J Burn Care Res. 2014; 35(4):e276-e280. 11. Deroux A, Brion JP, Hyerle L, et al. Association between hepatitis E and neurological disorders: two case studies and literature re- JULY/AUGUST 2016 | Volume 39 • Number 4 view. J Clin Virol. 2014; 60(1):60-62. 12. Hussey AJ, O’Brien CP, Regan PJ. Parsonage-Turner syndrome: case report and literature review. Hand (N Y). 2007; 2(4):218-221. 13. Weng M, Fidel C. Isolated unilateral brachial neuritis of the phrenic nerve (ParsonageTurner syndrome) in a marathon runner with exertional dyspnea. Sports Health. 2010; 2(4):307-310. 14. Landau ME, Faillace WJ, Nesti LJ, Grimes JB. Neuralgic amyotrophy manifested by se- vere axillary mononeuropathy limited only to the anterior branch. Muscle Nerve. 2015; 52(1):143-145. 15. Dumitru D. Brachial plexopathies and proximal mononeuropathies. In: Dumitru D, Amato AA, Zwarts MJ, eds. Electrodiagnostic Medicine. 2nd ed. Philadelphia, PA: Hanley & Belfus; 2001:623-624. 16. Tsairis P, Dyck PJ, Mulder DW. Natural history of brachial plexus neuropathy: report of 99 patients. Arch Neurol. 1972; 27(2):109117. e759