Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
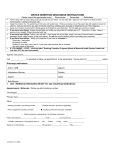
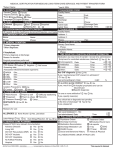
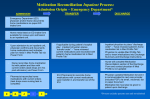
OBSERVATION UNIT DVT PATHWAY OUTLINE Frick Hospital Latrobe Hospital Westmoreland Hospital Exclusion Criteria: (Reason to admit as Inpatient to the hospital) A. New documented Pulmonary Embolus (PE) or clinical suspicion for PE if unable to get definitive test B. Unstable vital signs: Hypotension/Tachycardia C. New hypoxemia on room air or on usual home O2 (SaO2 ≤ 90%) D. Contraindication to Low Molecular Weight Heparin (LMWH) E. New unexplained anemia (Hgb < 10) F. Heme-positive stool with any level of anemia G. Active bleeding / high risk of bleeding H. History of Heparin Induced Thrombocytopenia I. Platelet count less than 75,000 J. Previous episodes of DVT > 2 or recurrent within last 3 months K. Failed outpatient anticoagulant therapy L. High risk for falls or trauma M. Concomitant Unstable or exacerbated co-morbidity requiring admission Observation Interventions: A. Continuous Cardiac Monitoring B. Monitor Vital Signs every 4 hours C. Teach Patient/caregiver how to administer LMWH / Coumadin education D. Arrange home health services E. Further imaging as indicated F. Physician to evaluate patient at admission, discharge and as needed. Disposition Criteria: A. HOME 1) Clinically stable (stable vital signs including O2 Saturation) and able to ambulate 2) No suspicion for PE 3) Anticoagulants initiated 4) Patient/caregiver demonstrate ability to manage care B. 1) 2) 3) ADMIT TO HOSPITAL Patient becomes unstable or develops PE Unable to ambulate due to pain and no support mechanism at home Develops signs of bleeding (This page not a part of the medical record.) EXC 9600-032Ci (Rev.7/11) OBSERVATION UNIT DVT PATHWAY OUTLINE Frick Hospital Latrobe Hospital Westmoreland Hospital PAGE 1 OF 4 Place on Observation Unit for Observation Services due to (Reason): __________________ ____________________________________________________________________________ Directed H&P Dictated: YES NO PCP: ___________________________ ORDERS: Nursing to do the following: • Cardiac Monitor Æ Nurse Notifies Physician of any arrhythmias • Nursing to check vitals with Pulse Oximetry and assess symptoms/pain level every 4 hours • Activity: Up as tolerated unless contraindicated -- Off monitor for testing • Thigh high TED stocking to leg with DVT • Obtain accurate weight in Kg • Allergies: _________________________________________________ _________________________________________________ • Reinforce observation status with patient including anticipated length of stay less than 23 hours Choose all the following that apply: Diet: [ ] Cardiac [ ] Consistent Carbohydrate (CHHO/ADA) [ ] IV Fluids [ ] General [ ] Other _____________ Type _____________ at ___________ml/hour Physician Signature ______________________________ Date _______ Time _______ Verbal Order _____________________________________ Date _______ Time _______ EXC 9600-032Ci (Rev.7/11) OBSERVATION UNIT DVT PATHWAY OUTLINE Frick Hospital Latrobe Hospital Westmoreland Hospital PAGE 2 OF 4 ORDERS (continued): Medications: • Physician to review Admission Medication Reconciliation Form (to see allergies and continue/discontinue/clarify patient home medications and add any additional medications needed for Observation DVT from the list below). • Nursing will scan all orders to the pharmacy along with Admission Medication Reconciliation Form. Lovenox 1mg/kg subcutaneously every 12 hours or every 24 hours (For GFR < 30) Coumadin _______ mg p.o. tonight Tylenol 650 mg p.o. every 6 hours p.r.n. for mild pain/fever Percocet 1 tablet or 2 tablets p.o. every 4 hours p.r.n. for moderate pain Vicodin 1 tablet or 2 tablets p.o. every 4 hours p.r.n. moderate pain (Max. 8 per 24 hours) OTHERS: ________________________________________________________ ______________________________________________________ ______________________________________________________ Labs and studies: CBC, PT/INR, LFT’s if not done in ED Urine pregnancy test for menstruating women if not done in ED Daily PT / INR Initiate Lovenox and Coumadin education and assess patient / caregiver willingness and readiness to administer Lovenox Case manager to assess for coverage of Lovenox and availability in pharmacy Home Health consult for Lovenox administration at home Lytes Bun/ Cr CBC Tomorrow AM or At ________________(Specify date and time needed) Spiral CT of chest with IV contrast to evaluate for PE V/Q scan to evaluate for PE Other ____________________________________________________________ _____________________________________________________________ _____________________________________________________________ Physician Signature ______________________________ Date _______ Time _______ Verbal Order _____________________________________ Date _______ Time _______ EXC 9600-032Ci (Rev.7/11) OBSERVATION UNIT DVT PATHWAY OUTLINE Frick Hospital Latrobe Hospital Westmoreland Hospital PAGE 3 OF 4 PROGRESS NOTES: (date, time and sign each entry) Briefly document any interim patient encounters here. _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ Disposition (If admitted as “Inpatient”, document rationale): _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ DISCHARGE NOTE/ADDENDUM TO H & P DICTATED: YES NO Physician Signature _________________ Date _________ Time ______ EXC 9600-032Ci (Rev.7/11) OBSERVATION UNIT DVT PATHWAY OUTLINE Frick Hospital Latrobe Hospital Westmoreland Hospital PAGE 4 OF 4 PHYSICIAN (Discharge): • Review Discharge Medication Reconciliation Form. • Prescriptions provided for: ________________________________ • Complete Patient Discharge Instructions. • Discharge condition _________________________________ • Discharge to _______________________________________ DISCHARGE ORDERS (Check [√] when done and initial) Nursing Smoking cessation packet given on admission, if patient is a current smoker or quit within the past year. RN ______ DVT Education Folder given on admission. RN ______ Reinforce Lovenox/Coumadin Teaching N/A RN ______ Patient signs Discharge Instructions after review RN_______ Patient given, verbalizes understanding, and signs Medication Reconciliation Home Instructions Form RN_______ Patient verbalizes understanding of recommended follow-up RN_______ Case Management (CM) To be done as close to start of care as possible: Reinforce observation status with patient including anticipated length of stay less than 23 hours Arrange Home Lovenox / Home Health or N/A Assess for discharge needs Assess for transportation needs At Discharge: *CM Contact patient’s Primary Care Physician or covering physician to inform PCP the patient was in Observation Unit for DVT. CM______ *CM Complete the “Physician Notification” form and fax to PCP. CM_______ *Nursing to do after hours RN _______ Physician Signature __________________ Date _________ Time _____ RN Signature ________________________ Date ________ Time _____ CM Signature ________________________ Date ________ Time _____ EXC 9600-032Ci (Rev.7/11)