Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
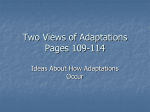
2226 Point/Counterpoint Folate and Cancer Prevention—Where to Next? Counterpoint Cornelia M. Ulrich Cancer Prevention Program, Fred Hutchinson Cancer Research Center, Seattle, Washington It is an interesting task to write a ‘‘counterpoint’’ to Dr. Kim’s article on folate and cancer prevention (1). We both agree that there are positive and negative aspects to the B-vitamin folate in cancer prevention and the terms ‘‘Janus-head’’ and ‘‘double-edged sword’’ have been used. In the broader sense, the folate story reminds us that as cancer epidemiologists we need to be mindful of cancer biology and the potentially different roles of an exposure during the carcinogenic process. In addition, we may need to consider nonlinear relationships and the potential for an optimum exposure beyond which one may not do additional good, but possibly harm. In the following, I will focus on some key aspects of folate in carcinogenesis and cancer epidemiology. Because of the high intakes of synthetic folate (=folic acid) in much of the population (as part of nutritional supplements, functional foods, and food fortification), we need to devise a research agenda that will fill fundamental gaps in our knowledge. The following will briefly summarize what is known today about folate and cancer prevention and suggest some next steps to arrive at responsible public health recommendations. Biological Mechanisms—Does Folate Status Mediate Carcinogenesis via Epigenetic Effects? Folate biochemistry is generally very well understood: all major enzymes are described and both cytosolic and mitochondrial folate metabolism is well defined (2, 3). The connection of folate to carcinogenesis is probably attributed to a large degree to its role in nucleotide synthesis; experimental studies unequivocally link folate deficiency to decreased synthesis of both thymidylate and purines, with subsequent DNA damage and inadequate repair (4). Recent studies suggest that enzymes of folate-mediated one-carbon metabolism that are critical for nucleotide synthesis exist not only in the cytosol but also directly in the nucleus (5). This is an active area of research. However, folate is also critical for the provision of methyl groups, including for DNA methylation, which is Cancer Epidemiol Biomarkers Prev 2008;17(9):2226 – 30 Received 12/31/07; accepted 4/8/08. Grant support: NIH grants CA 105437 (C.M. Ulrich), CA 59045 (J.D. Potter), and CA 105145 (C.M. Ulrich). Requests for reprints: Cornelia M. Ulrich, Cancer Prevention Program, Fred Hutchinson Cancer Research Center, Seattle, WA 98109. Phone: 206-667-7617; Fax: 206-667-7850. E-mail: [email protected] Copyright D 2008 American Association for Cancer Research. doi:10.1158/1055-9965.EPI-07-2952 an important epigenetic mode of gene silencing. The connection between DNA methylation and cancer risk is complicated: DNA methylation can occur at known gene promoters as well as in repetitive genomic sequences; currently, the processes that initiate and regulate DNA methylation at these different sites are poorly understood, although BRAF mutations may play a role (6). During carcinogenesis, both global hypomethylation at repetitive sequences and promoter-specific hypermethylation with associated gene silencing are observed. The capacity of folate status to affect global genomic methylation is fairly well supported by both human and experimental data (7-11). However, data are sparse and conflicting on whether folate status affects promoter methylation of specific genes or the CpG island methylator phenotype, which characterizes tumors with widespread hypermethylation of gene promoters (12-18). Thus, more epidemiologic and experimental studies evaluating the effects of folate deficiency and folate excess on epigenetic biomarkers are looked for, ideally involving epigenetic assays in target tissues (e.g., the gastrointestinal tract). It is important to note that lymphocytes, which have been used as easily accessible source of DNA, have a short life span and do not necessarily reflect methylation patterns of the tissue of interest (e.g., the colon or breast). Where Are Gaps in the Cancer Epidemiology of Folate and One-Carbon Nutrients? The role of folate in nucleotide synthesis suggests that an adequate intake is most critical for tissues with regularly replicating cells or tissues that are undergoing periods of growth. Indeed, antifolate drugs (discussed in more detail below) can have severe toxicities affecting the gastrointestinal tract (which is constantly self-renewing) as well as the hematopoietic system, both of which are sites of active cellular replication. The epidemiologic evidence on folate and cancer is consistent with this biological mechanism of an adequate supply of folate being vital for nucleotide synthesis and reduction of mutations in replicating tissues. The body of epidemiologic literature can perhaps be summarized as reflecting consistent inverse associations between higher folate intakes and colorectal cancer (19), a possible role of low folate increasing the risk of breast cancer, most likely in conjunction with high alcohol intakes (20), and some evidence for inverse associations with other gastrointestinal cancers, cervical cancer and pancreatic cancer. There are several key questions that still need to be addressed with regard to the epidemiology of folate and Cancer Epidemiol Biomarkers Prev 2008;17(9). September 2008 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention cancer. First, are the dose-response relationships linear, or do we observe a flattening out with higher intakes and, perhaps, even increases in risk with excessive intakes (20)? Second, what are the associations between dietary and supplemental folate intakes and hematopoietic cancers? These have been strongly associated with genetic polymorphisms (21-23), yet studies on diet have been sparse. Third, to what extent do epidemiologic associations differ, depending on the source of folate (i.e., the natural form from foods, versus the synthetic form, folic acid, from supplements or fortified foods)? Folic acid has greater bioavailability and thus epidemiologic studies of diet should use the composite ‘‘dietary folate equivalents’’ to account for both dietary folate and synthetic folic acid from fortified foods or supplements (24) to obtain a more accurate exposure measure. In addition, other nutrients that are important in onecarbon metabolism, particularly, vitamin B6 or methionine, may be linked to cancer risk (25, 26) and this area deserves further investigation. What Is the Importance of Genetic Variability in Folate Metabolism? There are common genetic polymorphisms that affect both folate homeostasis and the risks of several types of cancer (27-30). The ‘‘poster child polymorphism’’ in this regard is the MTHFR C677T variant, which shows a fairly consistent, and biochemically supported, pattern of gene-diet interaction in relation to cancer risk. In addition, the thymidylate synthase promoter variant that clearly reduces thymidylate synthase gene expression has also been associated with cancer risk. These polymorphisms may also affect mutation patterns and tumor characteristics (31, 32). The fact that these polymorphisms are associated with cancer risk, particularly of the gastrointestinal and hematopoietic systems, strongly implicates folate status as causally related to disease. However, most studies to date have focused only on selected candidate polymorphisms. Because of the well-supported significance of folate and folaterelated polymorphisms to health outcomes, we should undertake a comprehensive assessment of genetic variability (with sufficient power and appropriate biomarkers) in relation to multiple cancer types. Subsequently, we will face the challenge of devising appropriate statistical analysis tools for pathway-based analyses; folate metabolism is a promising starting point for such analyses: the biochemical relationships are well defined and several nonlinear interactions have been described. Our group’s efforts have focused on integrating mathematical modeling of the biochemistry of folate metabolism in the statistical data analysis (33, 34); however, many other important approaches to pathway-based analyses are getting developed and are critical to support molecular epidemiologic studies of candidate pathways. Is Folate A Cancer Chemopreventive Agent? The results of the Aspirin/Folate Polyp Prevention Trial have added yet another complexity to the picture of folate and cancer (35). This first randomized, controlled trial of folic acid for chemoprevention of colorectal polyps included about 1,000 participants with a history of colorectal adenomas who were randomly assigned to 1 mg/d folic acid F aspirin. Follow-up colonoscopies took place f3 years after the initial endoscopy and supplementation continued until a second surveillance exam. Folic acid clearly did not prevent the recurrence of colorectal adenomas at 3 years (rate ratio, 1.04) and at the second follow-up (rate ratio, 1.13; 0.93-1.37). In fact, at the second follow-up, the intervention group experienced a 67% increased risk of advanced lesions (rate ratio, 1.67; 1.00-2.80), along with a more than 2-fold increased risk of having at least three adenomas (rate ratio, 2.32; 1.23-4.35). How should one interpret the unexpected results of this study? The most likely explanation for the increased risk of advanced and multiple adenomas in the intervention group is that early precursor lesions were present in the mucosa of these patients and not detected during endoscopy and that folic acid promoted growth of these lesions (36). This is consistent with the notion that patients with adenoma are at increased risk of a second adenoma. Thus, the trial was designed to investigate the secondary prevention on colorectal adenoma, rather than the primary prevention. Based on the epidemiologic picture overall, higher folate status seems protective against colon cancer (19), although apparently not in individuals with precursor lesions. So what should be our next steps after this trial? Do we need to give up on folate as a cancer-preventive agent entirely? Should we attribute the discrepancy between the epidemiologic and trial data simply to faulty epidemiologic data, perhaps pointing to confounding by other substances in fruits and vegetables, or health behaviors associated with fruits and vegetables? The strong experimental evidence and the associations with genetic polymorphisms in genes of this pathway argue against this interpretation. Rather, the trial results should be interpreted in light of our knowledge today, about the different effects of folate during the process of carcinogenesis (Fig. 1). The trial results also point toward several critical avenues of research. We know that many cancers respond to chemotherapy with agents that target folate metabolism, such as 5-fluorouracil and methotrexate (37). These drugs result in reduced nucleotide synthesis with subsequent DNA damage and apoptosis (37). Further, tumors are known to up-regulate folate receptors and enzymes in nucleotide synthesis (38-44), consistent with a greater need for folate to support DNA synthesis and tumor growth. The experimental evidence from studies in rats and mice [as reviewed by Kim (1, 45)] implicates folate as supporting the growth of early neoplastic lesions. Thus, the interpretation that folate supplementation in the Aspirin/Folate Polyp Prevention Trial increased the growth of undetected precursor lesions in individuals at high risk of recurring adenomas is well supported. The trial raises yet several important questions: First, what are the net effects of folate supplementation on colon cancer rates in the population? Is there a ‘‘biological switch’’ after which supplementation may be harmful? Data by Mason et al. (46) suggest a potential increase with the initiation of folate fortification in both the United States and Canada. In addition to this ecologic study, our group has used an established model of colon cancer development (47) to mimic the dual role of folate in carcinogenesis (48). Findings from this modeling suggest that the Cancer Epidemiol Biomarkers Prev 2008;17(9). September 2008 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research. 2227 2228 Folate in Cancer Prevention Figure 1. Possible dual roles of folate in the prevention and promotion of carcinogenesis, as suggested by prior investigations (59, 60). Although higher folate status prevents an accumulation of mutations and genomic instability, it may also foster the growth of early preneoplastic lesions. effects of folate on colon carcinogenesis are indeed age and dose dependent, with predominantly harm if the amount of folate given were to increase cellular replication rates by 20%. However, this modeling also illustrated the shortcomings in the current literature on quantitative estimates of the response of tissues or cancer precursors to folate or folic acid supplementation. To better estimate risks to the population, it will be essential that such data are obtained experimentally. Can Folate Promote the Growth of Cancer Precursors in Humans? An interrelated question is what the effects of folate supplementation may be on existing colorectal polyps? In the Aspirin/Folate Polyp Prevention Trial, the study design with repeated colonoscopies ensured that no colons contained polyps. Yet, in the general U.S. population, only about a third of adults over age 50 have had an endoscopic examination in the previous 5 years (49). It has been estimated that f30% of individuals over age 60 carry a prevalent colorectal polyp (50). Use of folic acid – containing supplements is particularly common in this age group (51). Studying the effects of folic acid supplementation on unresected colorectal polyps is unethical in humans; thus, we need to rely on animal experiments, perhaps incorporating new technologies, such as mouse endoscopy (52). Incorporating results from such studies may then be used to inform mathematical modeling of the opposing effects of folic acid on cancer in humans. Is There a Safe Dose of Folic Acid? Most recently, results from the ukCAP trial, which parallels the Aspirin/Folate Polyp Prevention Trial, have become available (53). Here, 853 European individuals with a prior history of adenoma were randomized to 500 Ag folic acid or aspirin (in a similar 2 2 factorial design). Follow-up colonoscopies were targeted at 3 years, yet sometimes completed earlier. The trial showed relative risks of 1.07 (0.85-1.34) for the occurrence of any adenoma in the folic acid intervention arm and 0.98 (0.68-1.40) for advanced adenoma and, again, no evidence for cardiovascular protection. Does this suggest that a dose of 500 Ag does not have tumor-promoting effects? This conclusion would be premature because the relative risks from the ukCAP trial are consistent with those of the Aspirin/Folate Polyp Prevention Trial at its first 3-year follow-up (e.g., 1.07 versus 1.04 for any adenoma), and in the Aspirin/Folate Polyp Prevention Trial, the elevated risks did not emerge until the second follow-up after 6 to 8 years, which is largely consistent with the time frame for development of a larger colorectal polyp. The ukCAP trial took place in countries that have not (yet) introduced folic acid fortification, which reduced participants’ background folic acid intakes by about 150 to 200 Ag/d. Finally, polyp multiplicity was not assessed, which was increased most prominently in the Aspirin/Folate Polyp Prevention Trial. Hopefully, the intervention period of the ukCAP trial can be extended or participants followed further to provide insight into the long-term effects of the 500 Ag folic acid intervention in a nonfortified population. What Are the Effects of Folate Supplements on Cancer Prognosis? Another research priority ought to be studying the effects of folate supplementation among cancer patients. Cancer patients generally consume more supplements than healthy individuals, frequently without knowledge of the treating physicians (54). A significant proportion of Cancer Epidemiol Biomarkers Prev 2008;17(9). September 2008 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention cancer patients will exceed the recommended upper intake level of synthetic folic acid of 1,000 mg/d (55). Such intakes can be easily achieved by use of multivitamins (f400 Ag folic acid), health drinks or bars (up to 400 Ag folic acid), breakfast cereals (up to 400 Ag folic acid per serving), and folic acid fortification (in average 100-200 Ag/d). Considering the potential of folate to support or enhance the growth of tumors, we urgently should initiate studies of the effects of folate supplement use on cancer progression and recurrence. Studying the role of folate status in cancer prognosis is particularly relevant, given that methotrexate and 5-fluorouracil are commonly used chemotherapeutic drugs that target enzymes in folate metabolism. Initial research suggests that their efficacy and toxicity can be related to genetic polymorphisms in folate metabolism (56, 57). However, the role of folate supplementation during chemotherapy and radiation therapy has been insufficiently explored (58). Considering the multiple components of folate status in cancer patients, including folate-related characteristics of the tumor, the patient, chemotherapy, and supplement use, an integrated and interdisciplinary approach to prognostic studies of folate and cancer will be most successful. Finally, the Aspirin/Folate Polyp Prevention Trial has reported an increased risk of cancers other than colorectal cancer in the intervention group, largely attributable to prostate cancer cases (35). Although the number of cases was small, the potential public health effect of an increase in the progression of prostate cancers with folic acid is significant and requires rigorous followup studies. Summary and Recommendations In summary, the recently completed Aspirin/Folate Polyp Prevention Trial has added an important chapter to the story of folate and cancer: the results raise concerns about the use of folic acid in older individuals who may harbor cancer precursors, as well as cancer patients. The exposure of the public to synthetic folic acid is high, particularly among consumers of supplements and fortified health foods. Thus, it is critical that we continue research on the effects of folate on carcinogenesis in the context of our knowledge of cancer biology. A dual role of folate in carcinogenesis is the most likely explanation for the somewhat contradictory research findings from epidemiology and the cancer prevention trial. Yet, we still need better quantitative experimental data on the growth-promoting effects of folate in carcinogenesis of the colon and other tissues to clarify the potential of adverse effects of folate at varied doses. A research agenda on folate and cancer should aim to fill gaps in understanding the biological mechanisms (especially effects of folate status on epigenetics) and cancer etiology (dose response, genetic variability, and noncolon cancers). Yet, particularly important from a public health perspective are studies on the effects of high or excessive folate intakes in patients with cancer precursors or cancer, and the effects of these high intakes on their prognosis. In the absence of these important data to inform our decision making, what should be the current public health recommendations? First, as a safeguard, clinicians should inquire about the use of supplements among cancer patients and caution them against high intakes of folic acid from supplements, particularly when their nutritional intake in general is adequate or good. Second, countries that are currently considering mandatory fortification with folic acid (such as Australia and several European countries) may be best advised to defer decisions until more is known about the potential cancer-promoting effects of added folic acid. Disclosure of Potential Conflicts of Interest No potential conflicts of interest were disclosed. Acknowledgments I thank Dr. John D. Potter and my other colleagues working on folate and carcinogenesis for their valuable insights. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. Kim Y-I. Folic acid supplementation and cancer risk: Point Cancer Epidemiol Biomarkers Prev 2008;17:2220 – 25. Wagner C. Biochemical role of folate in cellular metabolism. Folate in health and disease. New York: Marcel Dekker; 1995. Nijhout HF, Reed MC, Lam SL, Shane B, Gregory JF III, Ulrich CM. In silico experimentation with a model of hepatic mitochondrial folate metabolism. Theor Biol Med Model 2006;3:40. Choi SW, Mason JB. Folate status: effects on pathways of colorectal carcinogenesis. J Nutr 2002;132:2413 – 8S. Woeller CF, Anderson DD, Szebenyi DM, Stover PJ. Evidence for small ubiquitin-like modifier-dependent nuclear import of the thymidylate biosynthesis pathway. J Biol Chem 2007;282:17623 – 31. Laird PW. Cancer epigenetics. Hum Mol Genet 2005;14 Spec No 1: R65 – 76. Rampersaud GC, Kauwell GP, Hutson AD, Cerda JJ, Bailey LB. Genomic DNA methylation decreases in response to moderate folate depletion in elderly women. Am J Clin Nutr 2000;72:998 – 1003. Kim YI. Folate and DNA methylation: a mechanistic link between folate deficiency and colorectal cancer? Cancer Epidemiol Biomarkers Prev 2004;13:511 – 9. Davis S, Stacpoole PW, Bailey LB, Gregory JF III. C677T MTHFR genotype & homocysteine remethylation; effects of folate depletion. Exp Biol 2002. Shelnutt KP, Kauwell GP, Gregory JF III, et al. Methylenetetrahydrofolate reductase 677C!T polymorphism affects DNA methylation in response to controlled folate intake in young women. J Nutr Biochem 2004;15:554 – 60. Pufulete M, Al-Ghnaniem R, Khushal A, et al. Effect of folic acid supplementation on genomic DNA methylation in patients with colorectal adenoma. Gut 2005;54:648 – 53. van den Donk M, van Engeland M, Pellis L, et al. Dietary folate intake in combination with MTHFR C677T genotype and promoter methylation of tumor suppressor and DNA repair genes in sporadic colorectal adenomas. Cancer Epidemiol Biomarkers Prev 2007;16: 327 – 33. Waterland RA, Jirtle RL. Transposable elements: targets for early nutritional effects on epigenetic gene regulation. Mol Cell Biol 2003; 23:5293 – 300. Dolinoy DC, Huang D, Jirtle RL. Maternal nutrient supplementation counteracts bisphenol A-induced DNA hypomethylation in early development. Proc Natl Acad Sci U S A 2007;104:13056 – 61. Paz MF, Avila S, Fraga MF, et al. Germ-line variants in methylgroup metabolism genes and susceptibility to DNA methylation in normal tissues and human primary tumors. Cancer Res 2002;62: 4519 – 24. Oyama K, Kawakami K, Maeda K, Ishiguro K, Watanabe G. The association between methylenetetrahydrofolate reductase polymorphism and promoter methylation in proximal colon cancer. Anticancer Res 2004;24:649 – 54. Curtin K, Slattery ML, Ulrich CM, et al. Genetic polymorphisms in one-carbon metabolism: associations with CpG island methylator phenotype (CIMP) in colon cancer and the modifying effects of diet. Carcinogenesis 2007;28:1672 – 9. van Engeland M, Weijenberg MP, Roemen GM, et al. Effects of dietary folate and alcohol intake on promoter methylation in Cancer Epidemiol Biomarkers Prev 2008;17(9). September 2008 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research. 2229 2230 Folate in Cancer Prevention 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. sporadic colorectal cancer: the Netherlands cohort study on diet and cancer. Cancer Res 2003;63:3133 – 7. Sanjoaquin MA, Allen N, Couto E, Roddam AW, Key TJ. Folate intake and colorectal cancer risk: a meta-analytical approach. Int J Cancer 2005;113:825 – 8. Ulrich CM. Folate and cancer prevention: a closer look at a complex picture. Am J Clin Nutr 2007;86:271 – 3. Skibola CF, Forrest MS, Coppede F, et al. Polymorphisms and haplotypes in folate-metabolizing genes and risk of non-Hodgkin lymphoma. Blood 2004;104:2155 – 62. Skibola CF, Smith MT, Hubbard A, et al. Polymorphisms in the thymidylate synthase and serine hydroxymethyltransferase genes and risk of adult acute lymphocytic leukemia. Blood 2002;99: 3786 – 91. Skibola CF, Smith MT, Kane E, et al. Polymorphisms in the methylenetetrahydrofolate reductase gene are associated with susceptibility to acute leukemia in adults. Proc Natl Acad Sci U S A 1999;96:12810 – 5. Institute of Medicine. Dietary reference intakes: thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. Washington (DC): National Academy Press; 1998. Larsson SC, Giovannucci E, Wolk A. Methionine and vitamin B6 intake and risk of pancreatic cancer: a prospective study of Swedish women and men [see comment]. Gastroenterology 2007;132:113 – 8. Zhang SM, Moore SC, Lin J, et al. Folate, vitamin B6, multivitamin supplements, and colorectal cancer risk in women. Am J Epidemiol 2006;163:108 – 15. Ulrich CM. Nutrigenetics in cancer research—folate metabolism and colorectal cancer. J Nutr 2005;135:2698 – 702. Little J, Sharp L, Duthie S, Narayanan S. Colon cancer and genetic variation in folate metabolism: the clinical bottom line. J Nutr 2003; 133:3758 – 66S. Ulrich C. Genetic variability in folate-mediated one-carbon metabolism and cancer risk. In: Choi SW, Friso S, editors. Nutrient-gene interactions in cancer. Boca Raton (FL): Taylor & Francis Group; 2006. p. 75 – 91. Ulrich CM, Curtin K, Potter JD, Bigler J, Caan B, Slattery ML. Polymorphisms in the reduced folate carrier, thymidylate synthase, or methionine synthase and risk of colon cancer. Cancer Epidemiol Biomarkers Prev 2005;14:2509 – 16. Ulrich CM, Curtin K, Samowitz W, et al. MTHFR variants reduce the risk of G:C!A:T transition mutations within the p53 tumor suppressor gene in colon tumors. J Nutr 2005;135:2462 – 7. Curtin K, Ulrich CM, Samowitz WS, et al. Thymidylate synthase polymorphisms and colon cancer: associations with tumor stage, tumor characteristics and survival. Int J Cancer 2007;120:2226 – 32. Reed MC, Nijhout HF, Neuhouser ML, et al. A mathematical model gives insights into nutritional and genetic aspects of folate-mediated one-carbon metabolism. J Nutr 2006;136:2653 – 61. Ulrich CM, Nijhout HF, Reed MC. Mathematical modeling: epidemiology meets systems biology. Cancer Epidemiol Biomarkers Prev 2006;15:827 – 9. Cole BF, Baron JA, Sandler RS, et al. Folic acid for the prevention of colorectal adenomas: a randomized clinical trial. JAMA 2007;297: 2351 – 9. Ulrich CM, Potter JD. Folate and cancer—timing is everything. JAMA 2007;297:2408 – 9. Kamen B. Folate and antifolate pharmacology. Semin Oncol 1997;24: S18 – 30-S18 – 39. Gates SB, Mendelsohn LG, Shackelford KA, et al. Characterization of folate receptor from normal and neoplastic murine tissue: influence of dietary folate on folate receptor expression. Clin Cancer Res 1996; 2:1135 – 41. Weitman SD, Lark RH, Coney LR, et al. Distribution of the folate 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. receptor GP38 in normal and malignant cell lines and tissues. Cancer Res 1992;52:3396 – 401. Ross JF, Chaudhuri PK, Ratnam M. Differential regulation of folate receptor isoforms in normal and malignant tissues in vivo and in established cell lines. Physiologic and clinical implications. Cancer 1994;73:2432 – 43. Dainty LA, Risinger JI, Morrison C, et al. Overexpression of folate binding protein and mesothelin are associated with uterine serous carcinoma. Gynecol Oncol 2007;105:563 – 70. Matherly LH, Hou Z, Deng Y. Human reduced folate carrier: translation of basic biology to cancer etiology and therapy. Cancer Metastasis Rev 2007;26:111 – 28. Kelemen LE. The role of folate receptor a in cancer development, progression and treatment: cause, consequence or innocent bystander? Int J Cancer 2006;119:243 – 50. Yang R, Kolb EA, Qin J, et al. The folate receptor a is frequently overexpressed in osteosarcoma samples and plays a role in the uptake of the physiologic substrate 5-methyltetrahydrofolate. Clin Cancer Res 2007;13:2557 – 67. Kim YI. Folate, colorectal carcinogenesis, and DNA methylation: lessons from animal studies. Environ Mol Mutagen 2004;44:10 – 25. Mason JB, Dickstein A, Jacques PF, et al. A temporal association between folic acid fortification and an increase in colorectal cancer rates may be illuminating important biological principles: a hypothesis. Cancer Epidemiol Biomarkers Prev 2007;16:1325 – 9. Luebeck EG, Moolgavkar SH. Multistage carcinogenesis and the incidence of colorectal cancer. Proc Natl Acad Sci U S A 2002;99: 15095 – 100. Luebeck EG, Moolgavkar SH, Liu AY, Boynton A, Ulrich CM. Does folic-acid supplementation prevent or promote colorectal cancer? Results from model-based predictions. Cancer Epidemiol Biomarkers Prev 2008;17:1360 – 7. American Cancer Society. Colorectal cancer facts and figures special edition 2005. Atlanta: American Cancer Society; 2005. Cannon-Albright LA, Bishop DT, Samowitz W, DiSario JA, Lee R, Burt RW. Colonic polyps in an unselected population: prevalence, characteristics, and associations. Am J Gastroenterol 1994;89:827 – 31. Ulrich CM, Potter JD. Folate supplementation: too much of a good thing? Cancer Epidemiol Biomarkers Prev 2006;15:189 – 93. Huang EH, Carter JJ, Whelan RL, et al. Colonoscopy in mice. Surg Endosc 2002;16:22 – 4. Logan RF, Grainge MJ, Shepherd VC, Armitage NC, Muir KR. Aspirin and folic acid for the prevention of recurrent colorectal adenomas. Gastroenterology 2008;134:29 – 38. Velicer CM, Ulrich CM. Vitamin and mineral supplement use among US adults after cancer diagnosis: a systematic review. J Clin Oncol 2008;26:665 – 73. Institute of Medicine. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. Washington (DC): National Academy Press; 1998. Ulrich CM, Robien K, McLeod HL. Cancer pharmacogenetics: polymorphisms, pathways and beyond. Nat Rev Cancer 2003;3: 912 – 20. Robien K, Boynton A, Ulrich CM. Pharmacogenetics of folate-related drug targets in cancer treatment. Pharmacogenomics 2005;6:673 – 89. Robien K. Folate during antifolate chemotherapy: what we know. . . and do not know. Nutr Clin Pract 2005;20:411 – 22. Melnyk S, Pogribna M, Miller BJ, Basnakian AG, Pogribny IP, James SJ. Uracil misincorporation, DNA strand breaks, and gene amplification are associated with tumorigenic cell transformation in folate deficient/repleted Chinese hamster ovary cells. Cancer Lett 1999;146: 35 – 44. Kim YI. Role of folate in colon cancer development and progression. J Nutr 2003;133:3731 – 9S. Cancer Epidemiol Biomarkers Prev 2008;17(9). September 2008 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research. Folate and Cancer Prevention−−Where to Next? Counterpoint Cornelia M. Ulrich Cancer Epidemiol Biomarkers Prev 2008;17:2226-2230. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cebp.aacrjournals.org/content/17/9/2226 This article cites 51 articles, 29 of which you can access for free at: http://cebp.aacrjournals.org/content/17/9/2226.full.html#ref-list-1 This article has been cited by 11 HighWire-hosted articles. Access the articles at: /content/17/9/2226.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2008 American Association for Cancer Research.