Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
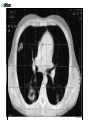
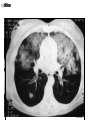
Vasculitis and connective tissue disease – just a taster!! The common and the rare!! Polymyalgia rheumatica (PMR) • Common clinical syndrome of middleaged & elderly (2-3 / GP) • characterized by pain & stiffness neck, shoulder & pelvic girdles • • dramatic response to small doses of steroids Giant cell arteritis • vasculitis underlying polymyalgia rheumatica and temporal arteritis • Other terms cranial arteritis & granulomatous arteritis • • Early recognition & treatment can prevent blindness & other complications resulting from occlusion or rupture of involved arteries Polymyalgia rheumatica • musculoskeletal symptoms usually bilateral & symmetric • Stiffness predominant feature; particularly EMS may prevent patient getting out of bed • • Muscular pain often diffuse; pain at night common • Corticosteroid treatment usually required for at least 2 years. Sometimes 4-5 years • Systemic features include low-grade fever, fatigue, weight loss & an increased erythrocyte sedimentation rate • Prednisolone 20 – 30mg / day ( tapering over 2 years or so) Giant cell arteritis • wide range of symptoms, clinical findings related to involved arteries • Frequently fatigue, headaches, jaw claudication, loss of vision, scalp tenderness, AND polymyalgia rheumatica • Risk is loss of vision – this is a medical emergency! • Prednisolone 40 – 60 mg / day ( tapering over 2 years or so) Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Figure 157.2 Granulomatous vasculitis. (a) Brain biopsy findings of granulomatous vasculitis side by side with a polyarteritis-type necrotizing arteritis (open arrow). (b) Close-up view of (a) showing foreign body (short arrow) & foreign body (long arrow) giant cells in granulomatous vasculitis. Hematoxylin & eosin, × 64 & 400 respectively. (With permission from Calabrese et al. 4) Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier 'vasculitis' • heterogeneous group of disorders characterized inflammatory alteration of blood vessel wall • primary event (primary vasculitis) - e.g. in ANCAassociated vasculitides • or secondary to other diseases (secondary vasculitis), e.g. in RA or SLE • underlying events mediated by immunologic mechanisms • supported by response to various potent immunosuppressives • Aggressive treatment to prevent permanent organ damage Few clues to aetiology of primary vasculitides • Hep B virus implicated as causative agent in polyarteritis nodosa (PAN) & Hep C in essential mixed cryoglobulinemia (EMC) • • circumstantial evidence for causative role of infection in Wegener's granulomatosis: seasonal variation in incidence of proteinase 3 autoantibodies (PR3-ANCA) suggests that an infectious agent prevalent in spring or autumn might trigger WG • genetic predisposition suggested by studies showing link between small vessel vasculitis & HLA-DQw7, between WG & DR1, & between HLA-Bw52 & giant cell arteritis • • • • • • • • • • • To name a few…….. Giant cell arteritis Takayasu arteritis Polyarteritis nodosa Kawasaki disease Wegeners Granulomatosis Churg-Strauss Syndrome Microscopic polyangiitis Henoch-Schonlein purpura Essential cryoglobulinaemic vasculitis Behcets disease Cutaneous leukocytoclastic vasculitis Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Figure 155.6 Leukocytoclastic vasculitis with ulceration in a patient with rheumatoid arthritis. Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Figure 146.4 Polyarteritis involving the gallbladder artery, showing pleomorphic inflammatory cell infiltration & fibrinoid necrosis. (With permission from Conn 10.) Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Figure 146.6 Vasculitis pathogenesis Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Connective tissue disease • group of conditions which affect many organs or tissues • widespread inflammation • Have some symptoms in common • All patients have features of general inflammation : fever, weight loss, tiredness & anaemia • Most patients also have inflammation of joints • Vasculitis of small blood vessels also common • Raynaud’s phenomenon • Involvement of the kidney may result in hypertension • If inflammation settles all symptoms improve • However, if process continues scarring occurs in affected tissues - will be damaged permanently • As well as symptoms common to whole group, each CTD has own particular symptoms • All can be distinguished clinically & serologically • All these CTD are rare • All more common in women • All treated with immunosuppressant drugs • SCLERODERMA; excessive fibrosis of tissues; skin is hard, & loses its ability to stretch. The fingertips are thickened & skin around the mouth tightens • POLYMYOSITIS; inflammation mainly in muscles; pain & weakness are main symptoms. Lung fibrosis • SLE; skin, joints, fatigue, mouth ulcers, alopecia, glomerulonephritis, lung fibrosis, CNS involvement • Sjogrens; sicca symptoms, joints, fatigue, lymphoma risk • • Also may have symptoms from different disorders; MIXED CONNECTIVE TISSUE DISEASE Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier Downloaded from: Rheumatology (on 19 November 2006 12:03 AM) © 2005 Elsevier Figure 122.6 Mouth ulcers in a patient with SLE. Downloaded from: Rheumatology (on 18 November 2006 12:39 PM) © 2005 Elsevier