Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
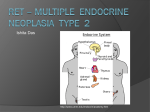
Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Personalized Medicine and Imaging RET Aberrations in Diverse Cancers: Next-Generation Sequencing of 4,871 Patients Clinical Cancer Research Shumei Kato1, Vivek Subbiah2, Erica Marchlik3, Sheryl K. Elkin3, Jennifer L. Carter3, and Razelle Kurzrock1 Abstract Purpose: Aberrations in genetic sequences encoding the tyrosine kinase receptor RET lead to oncogenic signaling that is targetable with anti-RET multikinase inhibitors. Understanding the comprehensive genomic landscape of RET aberrations across multiple cancers may facilitate clinical trial development targeting RET. Experimental Design: We interrogated the molecular portfolio of 4,871 patients with diverse malignancies for the presence of RET aberrations using Clinical Laboratory Improvement Amendments–certified targeted next-generation sequencing of 182 or 236 gene panels. Results: Among diverse cancers, RET aberrations were identified in 88 cases [1.8% (88/4, 871)], with mutations being the most common alteration [38.6% (34/88)], followed by fusions [30.7% (27/88), including a novel SQSTM1-RET] and amplifications [25% (22/88)]. Most patients had coexisting aberrations in addition to RET anomalies [81.8% (72/88)], with the most common being in TP53-associated genes [59.1% (52/88)], cell cycle–associated genes [39.8% (35/88)], the PI3K signaling pathway [30.7% (27/88)], MAPK effectors [22.7% (20/88)], or other tyrosine kinase families [21.6% (19/88)]. RET fusions were mutually exclusive with MAPK signaling pathway alterations. All 72 patients harboring coaberrations had distinct genomic portfolios, and most [98.6% (71/72)] had potentially targetable coaberrations with either an FDAapproved or an investigational agent. Two cases with lung (KIF5B-RET) and medullary thyroid carcinoma (RET M918T) that responded to a vandetanib (multikinase RET inhibitor)containing regimen are shown. Conclusions: RET aberrations were seen in 1.8% of diverse cancers, with most cases harboring actionable, albeit distinct, coexisting alterations. The current report suggests that optimal targeting of patients with RET anomalies will require customized combination strategies. Clin Cancer Res; Introduction RET aberrations can result in gain of function via amplification or mutations and rearrangements that result in ligandindependent kinase activation. These alterations have been reported in different types of malignancies and in hereditary conditions. Mutations in RET have been reported in patients with medullary thyroid carcinoma. They are seen in 43% to 71% of sporadic cases, with the most common mutation being RET M918T (5–8). Of note, germline mutations of RET are a hallmark of multiple endocrine neoplasia (MEN), including type 2A, 2B, and familial medullary thyroid carcinoma, with all three subtypes being associated with a high risk of developing a medullary thyroid carcinoma (70%–100% risk by age 70 years; ref. 9). Clinically, MEN 2A is also associated with pheochromocytoma and parathyroid hyperplasia, whereas MEN 2B is associated with mucosal neuromas, pheochromocytomas, intestinal ganglioneuromas and marfanoid habitus; familial medullary thyroid carcinoma is not associated with other conditions (9). Interestingly, different RET mutations are associated with distinct subtypes of MEN: (i) RET C634R, which leads to ligandindependent receptor dimerization, is most commonly associated with MEN 2A; (ii) RET M918T, which leads to decreased auto-inhibition and increased kinase activity, as well as ATP binding, is associated with MEN 2B; and (iii) various mutations at codons 609, 618, 620, 768, 804, and 891 are reported in both MEN 2A and familial medullary thyroid carcinoma (9, 10). These observations suggest that different RET-activating mutations have dissimilar oncogenic effects. The RET proto-oncogene encodes a transmembrane receptor tyrosine kinase composed of an extracellular cadherin domain, cysteine-rich region, transmembrane domain, and an intracellular kinase domain (1, 2). It functions as the receptor for the growth factors of the glial cell line–derived neurotropic factor family (3). Binding of ligand facilitates RET kinase activation, which leads to activation of multiple downstream effectors, including MAPK and PI3K pathways (3). Physiologically, RET is crucial for neural crest development (1, 2); loss-of-function mutations in RET are associated with aganglionic megacolon in Hirschsprung disease (4). 1 Department of Medicine, Center for Personalized Cancer Therapy and Division of Hematology and Oncology, University of California, San Diego, Moores Cancer Center, San Diego, California. 2Department of Investigational Cancer Therapeutics, The University of Texas MD Anderson Cancer Center, Houston, Texas. 3N-ofOne, Inc., Lexington, Massachusetts. Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Shumei Kato, UC San Diego Moores Cancer Center, 3855 Health Sciences Drive, La Jolla, CA 92093. Phone: 858-822-2372; Fax: 858822-6186; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-16-1679 2016 American Association for Cancer Research. 1–10. 2016 AACR. www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. OF1 Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Kato et al. Translational Relevance To optimize clinical trials targeting RET aberrations, understanding the relevant genomic landscape in diverse cancers is critical. Here, we report the molecular portfolio, including coexisting alterations, of RET-altered cancers in 4,871 patients who were evaluated using clinical grade next-generation sequencing. Among 88 cases with RET aberrations, the most common alterations included mutations [38.6% (34/88)], fusions [30.7% (27/88)], and amplification [25% (22/88)]. In the 72 patients harboring coaberrations along with RET alterations, there were no two patients with identical molecular portfolios. Among 292 coexisting molecular aberrations, 200 were molecularly distinct. The median number of coaberrations per patient was three (range, 0–16). In 71 of the 72 tumors with more than one alteration, at least one coexisting genomic alteration was potentially pharmacologically tractable, suggesting the need for customized combination treatments. On the other hand, fusions in RET have been described in patients with papillary thyroid carcinoma, accounting for approximately 20% to 40% of sporadic cases (2, 11), with a higher frequency of RET fusions observed after radioiodine exposure (60%; ref. 12). Diverse RET fusions have been identified, but more than 90% of fusions involve the coiled–coil domain-containing protein 6 (CCDC6)-RET or nuclear receptor coactivator 4 (NCOA4)-RET (also referred in the literature as RET/PTC1 and RET/PTC3, respectively; ref. 2). Although less frequent, several activating RET fusions have been reported in 1% to 2% of patients with non–small cell lung cancer (NSCLC). These include CCDC6-RET (13, 14), NCOA4RET (14), kinesin family member 5b (KIF5B)-RET (13–18), and tripartite motif-containing 33 (TRIM33)-RET (15). Identification of RET aberrations is therapeutically important as they are targetable with several FDA-approved multikinase inhibitors that have anti-RET activity, including vandetanib (RET/EGFR/VEGFR2 inhibitor, approved for medullary thyroid carcinoma), cabozantinib (RET/MET/VEGFR2 inhibitor, approved for medullary thyroid carcinoma), lenvatinib (RET/FGFR/ VEGFR/KIT/PDGFR inhibitor, approved for differentiated thyroid carcinoma and renal cell carcinoma), ponatinib (RET/ FGFR/VEGFR/KIT/PDGFR/BCR-ABL inhibitor, approved for chronic myeloid leukemia and Philadelphia chromosome–positive acute lymphoblastic leukemia), sunitinib [RET/VEGFR/KIT/ PDGFR/FLT3 inhibitor, approved for renal cell carcinoma and imatinib-resistant gastrointestinal stromal tumor (GIST)], regorafenib (RET/VEGFR/KIT/BRAF/CRAF inhibitor, approved for colorectal cancer and GIST), and sorafenib (RET/VEGFR/KIT/ BRAF/CRAF inhibitor, approved for differentiated thyroid carcinoma, renal cell carcinoma and hepatocellular carcinoma; refs. 19, 20). However, none of these inhibitors are FDA approved on the basis of targeting RET aberrations. Meanwhile, there are a series of reports suggesting that matched therapies against RET aberrations can yield significant responses (8, 15, 21–27). Further clinical trials with a focus on RET-aberrant advanced cancer are being conducted to determine impact on outcome (Supplementary Table S1). OF2 Clin Cancer Res; 2017 To facilitate the clinical trials targeting RET, a comprehensive understanding of RET aberrations among diverse cancer types is essential. Therefore, we examined the genomic landscape of RET alterations using targeted next-generation sequencing (NGS) in 4,871 patients with diverse malignancies, and we also show two illustrative cases of lung and medullary thyroid carcinoma with KIF5B-RET and RET M918T alterations, respectively, who both responded to vandetanib (multikinase RET inhibitor) containing regimen. Materials and Methods Patients We investigated the RET gene status of patients with diverse malignancies that were referred for NGS from October 2011 to November 2013 (N ¼ 4,871; Table 1 and Supplementary Tables S2 and S3; Fig. 1). The submitting physicians provided specification of tumor types. The database was deidentified with only diagnosis available. NGS data were collected and interpreted by N-of-One, Inc. The dataset of 4,871 sequenced tumors was queried for RET and coexisting gene alterations. Clinical impact was demonstrated by selected case studies. This study was performed in accordance with the guidelines of the UCSD and the MD Anderson Internal Review Board. Tissue samples and mutational analysis We collected sequencing information from 4,871 cancers whose formalin-fixed, paraffin-embedded (FFPE) tumor samples were submitted to a Clinical Laboratory Improvement Amendments–certified laboratory for genomic profiling (Foundation Medicine). Samples were required to have a surface area 25 mm2, volume 1 mm3, nucleated cellularity 80%, and tumor content 20% (28). The methods used in this assay have been validated and reported previously (28–30). In short, 50 to 200 ng of genomic DNA was extracted and purified from the submitted FFPE tumor samples. This whole-genome DNA was subjected to shotgun library construction and hybridization-based capture before paired-end sequencing on the Illumina HiSeq2000 platform. Hybridization selection is performed using individually synthesized baits targeting the exons of 182 or 236 cancer-related genes and the introns of 14 or 19 genes frequently rearranged in cancer (Supplementary Table S4). Sequence data were processed using a customized analysis pipeline (28). Sequencing was performed with an average sequencing depth of coverage greater than 250, with >100 at >99% of exons. This method of sequencing allows for detection of copy number alterations, gene rearrangements, and somatic mutations with 99% specificity and >99% sensitivity for base substitutions at 5 mutant allele frequency and >95% sensitivity for copy number alterations. A threshold of 8 copies for gene amplification with 6 copies considered equivocal (except for ERRB2, which is considered equivocally amplified with 5 copies) was used. cBio Cancer Genomics Portal data For comparison purposes, we evaluated the RET aberration status using the cBio Cancer Genomics Portal data (cBioPortal; http://cbioportal.org, accessed May 2016; refs. 31, 32), which provides access to publicly available datasets with genomic information from a diverse array of cancer types (please refer to Supplementary Methods for additional information). Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 RET Aberrations in Cancer Results Analysis of RET aberrations among diverse cancers (N ¼ 4,871) Among the 4,871 diverse cancer patients, the most common diagnosis was breast carcinoma [10.4% (506/4,871)], followed by lung adenocarcinoma [8.5% (412/4,871)], and sarcoma [7.1% (348/4,871); Table 1 and Supplementary Table S2]. Overall, RET aberrations were identified in 88 cases [1.8% (88/4,871)]. Among 88 cases with RET aberrations, 38.6% (34/88) were mutations, 30.7% (27/88) were fusions (defined as RET rearrangement with known fusion partner. e.g., KIF5BRET), 25% (22/88) were amplifications, and 3.4% (3/88) were rearrangements without specific identified fusion partner (e.g., RET rearrangement, exon 11). In addition, RET duplication and loss were each observed in 1 of 88 cases. (Fig. 1). According to cBioPortal, RET aberrations have been reported in 3.0% (181/6,011) of diverse cancers (Supplementary Table S5; Supplementary Fig. S1). In the current report, most RET aberrations were activating alterations [71.6% (63/88)] and one inactivating RET alteration was observed (RET loss). The functional significance of 27.3% (24/88) of RET aberrations, including RET R163Q, M255I, R525Q, V706M, A756V, M1109I, and SQSTM1-RET, fusion was unknown (Supplementary Table S3). Overview of cancer diagnoses and RET aberrations RET aberrations were most commonly seen in patients with medullary thyroid carcinoma [80% (4/5)], followed by anaplastic thyroid carcinoma [16.7% (2/12)], lung carcinosarcoma [16.7% (1/6)], and ureter urothelial carcinoma [16.7% (1/6)]; however, these cancer diagnoses were not reported in cBioPortal, and thus, direct comparisons were not feasible (Table 1 and Supplementary Table S5; Fig. 2 and Supplementary Fig. S1). Although there was only one patient each for hemangiopericytoma and pheochromocytoma, they both harbored RET aberrations (Table 1 and Supplementary Table S3). In some cancer diagnoses, including cholangiocarcinoma (n ¼ 159), neuroendocrine carcinoma (n ¼ 97), renal cell carcinoma (n ¼ 92), and glioblastoma (n ¼ 84), we did not observe RET aberrations (Supplementary Table S2). In contrast, data from cBioPortal showed rare RET alterations in cholangiocarcinoma Table 1. RET aberrations and associated cancer diagnosis (N ¼ 88) Diagnosis Hemangiopericytoma (n ¼ 1) Pheochromocytoma (n ¼ 1) Medullary thyroid carcinoma (n ¼ 5) Paraganglioma (n ¼ 4) Anaplastic thyroid carcinoma (n ¼ 12) Lung carcinosarcoma (n ¼ 6) Ureter urothelial carcinoma (n ¼ 6) Uterine carcinosarcoma (n ¼ 19) Papillary thyroid carcinoma (n ¼ 23) Basal cell carcinoma (n ¼ 8) Merkel cell carcinoma (n ¼ 10) Atypical lung carcinoid (n ¼ 11) Fallopian tube adenocarcinoma (n ¼ 12) Ovarian epithelial carcinoma (n ¼ 54) Salivary gland adenocarcinoma (n ¼ 31) Lung adenocarcinoma (n ¼ 412) Meningioma (n ¼ 18) Duodenal adenocarcinoma (n ¼ 20) Cervical adenocarcinoma (n ¼ 24) Adrenal carcinoma (n ¼ 27) Gastroesophageal junction carcinoma (n ¼ 29) GIST (n ¼ 30) Non–small cell lung carcinoma (n ¼ 125) Cutaneous squamous cell carcinoma (n ¼ 36) Hepatocellular carcinoma (n ¼ 44) Pancreatic ductal adenocarcinoma (n ¼ 160) Prostate adenocarcinoma (n ¼ 64) Melanoma (n ¼ 136) Esophageal adenocarcinoma (n ¼ 69) Endometrial adenocarcinoma (n ¼ 79) Ovarian serous carcinoma (n ¼ 169) Carcinoma unknown primary (n ¼ 270) Bladder urothelial (transitional cell) carcinoma (n ¼ 91) Lung squamous cell carcinoma (n ¼ 93) Colorectal adenocarcinoma (n ¼ 300) HNSCC (n ¼ 108) Sarcoma (n ¼ 348) Gastric adenocarcinoma (n ¼ 134) Breast carcinoma (n ¼ 506) Any aberrations n (%) 1 (100) 1 (100) 4 (80.0) 1 (25.0) 2 (16.7) 1 (16.7) 1 (16.7) 3 (15.8) 3 (13.0) 1 (12.5) 1 (10) 1 (9.1) 1 (8.3) 4 (7.4) 2 (6.5) 23 (5.6) 1 (5.6) 1 (5.0) 1 (4.2) 1 (3.7) 1 (3.4) 1 (3.3) 4 (3.2) 1 (2.8) 1 (2.3) 3 (1.9) 1 (1.6) 2 (1.5) 1 (1.4) 1 (1.3) 2 (1.2) 3 (1.1) 1 (1.1) 1 (1.1) 3 (1.0) 1 (0.9) 3 (0.9) 1 (0.7) 3 (0.6) Fusiona n (%) 0 0 0 0 0 1 (16.7) 0 0 2 (8.7) 0 0 0 0 1 (1.9) 1 (3.2) 16 (3.9) 0 0 0 0 0 0 4 (3.2) 0 0 0 0 0 0 0 0 2 (0.7) 0 0 0 0 0 0 0 Mutation n (%) 1 (100) 1 (100) 4 (80.0) 1 (25.0) 2 (16.7) 0 1 (16.7) 1 (5.3) 1 (4.3) 1 (12.5) 1 (10.0) 1 (9.1) 0 2 (3.7) 0 3 (0.7) 1 (5.6) 0 1 (4.2) 1 (3.7) 0 1 (3.3) 0 0 1 (2.3) 1 (0.6) 0 1 (0.7) 1 (1.4) 1 (1.3) 0 0 0 0 2 (0.7) 0 1 (0.3) 1 (0.7) 1 (0.2) Rearrangementa n (%) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 (0.5) 0 0 0 0 0 0 0 0 0 1 (0.6) 0 0 0 0 0 0 0 0 0 0 0 0 0 Amplification n (%) 0 0 0 0 0 0 0 1 (5.3) 0 0 0 0 1 (8.3) 1 (1.9) 1 (3.2) 2 (0.5) 0 1 (5.0) 0 0 1 (3.4) 0 0 0 0 1 (0.6) 1 (1.6) 1 (0.7) 0 0 2 (1.2) 1 (0.4) 1 (1.1) 1 (1.1) 1 (0.3) 1 (0.9) 2 (0.6) 0 2 (0.4) Duplication n (%) 0 0 0 0 0 0 0 1 (5.3) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 Loss n (%) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 (2.8) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 Abbreviation: HNSCC, head and neck squamous cell carcinoma. The term fusion was used when RET was rearranged with known fusion partner (e.g., KIF5B-RET). On the other hand, the term rearrangement was used when there was no specific identified fusion partner (e.g., RET rearrangement, exon 11). a www.aacrjournals.org Clin Cancer Res; 2017 Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. OF3 Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Kato et al. Duplicaon (1.1%) Loss (1.1%) Rearrangement (3.4%) RET Aberraons (1.8%) Amplificaon (25%) No RET aberraons (98.2%) N = 4,871 [5.7% (2/35)] and glioblastoma [0.7% (2/281); Supplementary Table S5; Supplementary Fig. S1]. Overview of cancer diagnosis and specific RET aberrations As mentioned, the most common type of RET aberrations were mutations [38.6% (34/88)], followed by fusions [30.7% (27/88)] and amplifications [25.0% (22/88); Fig. 1]. This observation was similar to cBioPortal data in relative frequencies, although the actual percentages for cBioPortal mutations, fusions, and amplifications differed a bit from our data [60.2% (109/181), 15.5% (28/181), and 12.7% (23/181), respectively; Supplementary Table S5; Supplementary Fig. S1]. In the current report, RET mutations were most commonly seen in patients with medullary thyroid carcinoma [80% (4/5)], followed by paraganglioma [25% (1/4)], anaplastic thyroid carcinoma [16.7% (2/12)], and ureter urothelial carcinoma [16.7% (1/6); Table 1; Fig. 2]. RET fusions were seen in patients with lung carcinosarcoma [16.7% (1/6)], followed by papillary thyroid carcinoma [8.7% (2/23)] and lung adenocarcinoma [3.9% (16/412)]. RET amplifications were detected in patients with fallopian tube adenocarcinoma [8.3% (1/12)], uterine carcinosarcoma [5.3% (1/19)], and duodenal adenocarcinoma [5.0% (1/20); Table 1; Fig. 2]. Coaberrant oncogenic pathways associated with RET aberrations Among 88 patients with RET aberrations, 72 also harbored coaberrations (Supplementary Table S3). Those include coaberrations with TP53-associated genes [59.1% (52/88)], cell cycle– associated genes [39.8% (35/88)], aberrations in the PI3K signaling pathway [30.7% (27/88)], MAPK effectors [22.7% (20/88)], and other tyrosine kinases families [21.6% (19/88); Fig. 3; Supplementary Table S5]. Coaberrant oncogenic pathways were all readily observed (greater than 20%) among RET mutations, amplifications, and fusions, except the coaberrations with tyrosine kinase families and MAPK signaling pathway were both infrequently associated with RET fusions [7.4% (2/27) and 0% (0/27), respectively; Supplementary Table S5]. Number of cogenetic aberrations associated with RET aberrations and possible cognate targeted therapies As mentioned, among 88 cases with RET aberrations, 72 patients also had cogenetic aberrations along with RET aberrations (Supplementary Table S3). Among these 72 cases, a total of OF4 Clin Cancer Res; 2017 Mutaon (38.6%) Fusion (30.7%) N = 88 Figure 1. Overview of RET aberrations among diverse cancers (N ¼ 4,871). Among diverse cancers (N ¼ 4,871), 88 cases (1.8%) harbored RET aberrations. Among 88 cases with RET aberrations, 38.6% (34/88) were mutations, 30.7% (27/88) were fusions (defined as RET rearrangement with known fusion partner, e.g., KIF5B-RET), 25% (22/88) were amplifications, 3.4% (3/88) were rearrangements (defined as RET rearrangement without specific identified fusion partner, e.g., RET rearrangement, exon 11), 1.1% (1/88) were duplication, and 1.1% (1/88) were loss. 292 coaberrations were identified. Among 292 coaberrations, 80.8% (236/292) were potentially targetable with FDA-approved agents as off-label use, and an additional 8.2% (24/292) were theoretically targetable with therapies that are currently in clinical trials. Altogether, among all coaberrations, 89.0% (260/292) were potentially actionable either with therapies that are approved by the FDA (albeit off label) or with therapies that are in clinical trials (Supplementary Tables S3 and S7). Among 292 coexisting aberrations, 200 were molecularly distinct alterations, occurring either in separate genes or distinct alterations within the same gene. However, there were 16 cases of CDKN2A/B loss, and those were considered as single aberration. Among these molecularly distinct aberrations, 80.0% (160/200) were targetable by an FDA-approved drug, and an additional 7.5% (15/200) were targetable by drugs that are under investigation in clinical trials (Supplementary Tables S3 and S7). Among 88 patients with RET aberrations, the median number of coaberrations per patient was three (range, 0–16; excluding RET alterations). The median number of coaberrations was similar among patients who were tested with the 182-gene panel (n ¼ 16 patients, median of 3 coaberrations, range 0–6) and 236-gene panel (n ¼ 72 patients, median of 3 coaberrations, range 0–16; Supplementary Table S4 for list of genes). The median number of potentially targetable coaberrations per patient was two (range, 0–16; Fig. 4). Among all 88 patients with RET aberrations, 78.4% (69/88) of patients had theoretically actionable coaberrations by an FDA-approved agent, and an additional 2.3% (2/88) patients had coaberrations targetable with investigational agents in clinical trial. Altogether, 80.6% (71/88) patients had actionable coaberrations either with FDA-approved or with investigational agents. However, if we only focus on 72 patients who had coaberrations along with RET aberrations, almost all patients had actionable coaberrations [98.6% (71/72)] either with FDA-approved or with investigational agents (Fig. 4; Supplementary Tables S3 and S7). Distinctness of genomic aberrations among 88 patients with RET aberrations Among 88 patients with RET aberrations, 12 patients had identical genomic portfolios [RET C634R (ID #1 and #2), RET M918T (patient ID #6, #8, #9, #11, and #12), RET-NCOA4 fusion (ID #37 and #38), and RET-CCDC6 fusion (ID #57, #58, and #60); Supplementary Table S3]. However, among 72 patients Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 RET Aberrations in Cancer ≈ All Medullary thyroid carcinoma Anaplastic thyroid carcinoma Lung carcinosarcoma Ureter urothelial carcinoma Uterine carcinosarcoma Papillary thyroid carcinoma Basal cell carcinoma Merkel cell carcinoma Atypical lung carcinoid Fallopian tube adenocarcinoma Ovarian epithelial carcinoma Salivary gland adenocarcinoma Lung adenocarcinoma Duodenal adenocarcinoma 0% 0% Fusion Mutation 5% 5% 10% 10% Rearrangement 15% 15% 20% 20% Amplification ≈ Meningioma 75% 25% Duplication 80% 30% 85% 35% Loss Figure 2. Frequencies and distributions of RET aberrations. RET aberrations were frequently seen in patients with medullary thyroid carcinoma [80% (4/5)], all being mutations. This was followed by anaplastic thyroid carcinoma [16.7% (2/12)], lung carcinosarcoma [16.7% (1/6)], and ureter urothelial carcinoma [16.7% (1/6)]. Included when RET was aberrant in 5% of cases and if at least 5 cancer diagnoses were tested for the aberration. Please see Table 1 for a complete list of cancer diagnoses found to be positive for RET aberrations. The term fusion was used when RET was rearranged with known fusion partner (e.g., KIF5BRET). On the other hand, the term rearrangement was used when there was no specific identified fusion partner (e.g., RET rearrangement, exon 11). harboring coaberrations along with RET aberrations, there were no two patients with identical genomic portfolios (Supplementary Table S3). If we consider the genetic alterations at the level of the gene (and not the specific molecular aberration), then five patients had coaberrations identical to at least one other patient. Those include patient ID #32 and #87 with KRAS and TP53 and ID #39, #41, and #45 with RB1, STK11, and TP53 coaberrations (Supplementary Table S3). Clinical impact of multikinase inhibitors with anti-RET activity in patients with RET aberrations To demonstrate the impact of therapies with anti-RET activity in cancer patients harboring RET aberrations, we report two patients with RET alterations who were treated with multikinase inhibitors that possess anti-RET activity. The first is a 43-year-old woman with adenocarcinoma of the lung and a KIF5B-RET fusion, refractory to multiple lines of therapies including the multikinase RET/ MET/VEGFR2 inhibitor cabozantinib. Treatment with another multikinase inhibitor, vandetanib (RET/EGFR/VEGFR2 inhibitor) in combination with everolimus (an mTOR inhibitor), led www.aacrjournals.org to a major response (Fig. 5A); the second patient was a 35-year-old man with sporadic medullary thyroid carcinoma and a RET M918T mutation as well as ATM L804fs 4 and ATM S978fs 12 alterations. Additional tumor evaluation with an IHC panel also showed strong positivity of phospho-AKT. The patient was initially treated with single-agent vandetanib with prolonged stable disease; however, the addition of everolimus led to significant tumor shrinkage (Fig. 5B). Discussion We report a comprehensive landscape of RET aberrations among 4,871 patients with diverse cancers. RET aberrations were identified in 1.8% (88/4,871) of tumors, with mutations being the most frequent aberration [38.6% (34/88)], followed by fusions [e.g., KIF5B-RET; 30.7% (27/88)], amplifications [25.0% (22/88)], rearrangements without specific identified fusion partner [e.g., RET rearrangement, exon 11; 3.4% (3/88)] and n ¼ 1 each of duplication and loss (Fig. 1). The overall frequency of RET aberrations in this current report is similar to the Clin Cancer Res; 2017 Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. OF5 Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Kato et al. Tyrosine kinases families (21.6%) Cell-cycle–associated genes (39.8%) CDKN2A/B (18.2%) CDKN2A (8.0%) CDKN2C (1.1%) CCND1 (3.4%) CCND2 (3.4%) FGFR1 (3.4%) FGFR2 (2.3%) FGFR3 (3.4%) FGFR4 (1.1%) DDR2 (1.1%) EGFR (2.3%) ERBB2 (2.3%) KDR (2.3%) ALK (1.1%) PDGFRA (2.3%) PDGFRB (1.1%) KIT (2.3%) CDK6 (2.3%) RB1 (6.8%) NF1 (6.8%) Cell-cycle progression TP53 (52.3%) SRC (1.1%) PTEN (5.7%) AKT2 (1.1%) TSC1 (2.3%) TSC2 (2.3%) STK11 (4.5%) ATM (4.5%) MDM2 (5.7%) PIK3CA (10.2%) PIK3R1 (1.1%) KRAS (10.2%) NRAS (3.4%) BRAF (4.5%) TP53-associated genes (59.1%) JAK2 (2.3%) PI3K Signaling (30.7%) MAPK Signaling (22.7%) CCNE1 (6.8%) FLT3 (3.4%) FLT4 (1.1%) MTOR (1.1%) RPTOR (1.1%) NF2 (2.3%) RICTOR (3.4%) Figure 3. Coaberrant oncogenic pathways associated with RET aberrations. Among 88 patients with RET aberrations, some patients also harbored coaberrations that can lead to tumorigenesis. Those coaberrations include TP53-associated genes [e.g., MDM2, ATM, or TP53; 59.1% (52/88)], cell-cycle–associated genes [e.g., CDKN2A/B, CDK6, or RB1; 39.8% (35/88)], PI3K signaling pathway [e.g., PIK3CA, PTEN, AKT, or MTOR; 30.7% (27/88)], MAPK effectors [e.g., KRAS, NF1, or BRAF; 22.7% (20/88)], and other tyrosine kinase families [e.g., FGFR, EGFR, ERBB2, ALK, or KIT; 21.6% (19/88)]. Please see Supplementary Tables S3 and S5 for a complete list of co-occurring aberrations associated with RET aberrations. Cell survival and proliferaon Cell survival and proliferaon frequency reported in the cBioPortal dataset 3.0% (181/6,011; Supplementary Table S5; Supplementary Fig. S1). RET mutations are a hallmark of medullary thyroid cancer (both sporadic and familial cases); they are reported in 43% to 71% of sporadic medullary thyroid carcinomas (5–8). RET M918T is the most common mutation reported in sporadic disease (5, 6, 8), which is consistent with the current report, wherein four of five medullary thyroid cancers 16 ≈ 11 Number of aberrations 10 9 8 Figure 4. Number of all reported coaberrations and possibly actionable coaberrations per patient. Among 88 patients with RET aberrations, there was a median of 3 coaberrations per patient (range, 0–16) and a median of 2 (range, 0–16) possibly actionable coaberrations per patient. Please see Supplementary Table S6 for a complete list of co-occurring aberrations and rationale for possible targeted therapies. 7 6 5 4 3 2 1 0 0 2 4 6 8 10 12 14 16 18 Number of patients All reported coaberrations Possibly actionable coaberrations OF6 Clin Cancer Res; 2017 Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 RET Aberrations in Cancer B Pretreatment Posttreatment Posttreatment 100 mm Pretreatment 100 mm A Figure 5. Case reports of patients with RET aberrations treated with anti-RET multikinase inhibitors. A, Never-smoker lung adenocarcinoma with KIF5B-RET fusion. Posttreatment PET scan was performed at 8 weeks and showed improvement in the right lung hypermetabolic tumor. A 43-year-old female never-smoker was diagnosed with stage IV poorly differentiated adenocarcinoma of the lung with focal signet features. Comprehensive genomic profiling revealed a KIF5B-RET fusion with CDK4 and MDM2 amplification. She was started on treatment with a multikinase RET/MET/VEGFR2 inhibitor, cabozantinib. She responded initially to treatment and derived clinical benefit for 12 months. On progression, she was then enrolled on a trial with carboplatin/paclitaxel plus a heat shock protein 90 inhibitor. She progressed after 7 months and was started on pemetrexed plus bevacizumab. Because of progression, she was enrolled on vandetanib, a multikinase inhibitor of RET/EGFR/VEGFR2 inhibitor, in combination with everolimus (an mTOR inhibitor; ClinicalTrials.gov; NCT01582191). Her performance status and pain improved while on therapy. After two cycles, FDG PET scans showed interval improvement in the right lung hypermetabolic tumor (A) and improvement in metastases to the bones and liver. She had a 76% decrease per RECIST version 1.1. However, she developed new sites of disease after four cycles and was taken off the trial and is now enrolled on another RET inhibitor trial. B, Recurrent medullary thyroid carcinoma sporadic type with RET M918T mutation. Posttreatment CT scan was performed at 8 weeks, which showed improvement of lymphadenopathy. A 45-year-old man without known family history of endocrine malignancy initially underwent thyroidectomy for localized medullary thyroid carcinoma. The patient subsequently developed multiple areas of lymphadenopathy and liver metastasis that was biopsy proven to be recurrent disease. Comprehensive genomic profiling revealed RET M918T as well as ATM L804fs 4 and ATM S978fs 12. The patient was treated with vandetanib for 12 months with overall stable disease with eventual slow increase in size. Meanwhile, the patient had further evaluation of the tumor sample with an IHC panel, including phospho-AKT, which showed positive intensity (3þ) in 100% of cells, suggesting coactivation of the PI3K pathway. He was subsequently enrolled on a trial with vandetanib, a multikinase inhibitor of RET/EGFR/VEGFR inhibitor, in combination with everolimus (an mTOR inhibitor; ClinicalTrials.gov; NCT01582191) with improvement in lymphadenopathy (B). His tumor demonstrated a 25% decrease per RECIST version 1.1 that lasted eight cycles. harbored RET mutations [M918T (n ¼ 3) and C634R (N ¼ 1); Table 1 and Supplementary Table S3; Fig. 2]. Activating RET mutations lead to enhanced downstream signaling with multiple effectors, including those in the MAPK and PI3K pathways, resulting in increased cell proliferation and anchorage-independent cell growth (33–35). Clinically, RET mutations are associated with poor clinical outcomes, including larger tumor size, metastasis, and poorer survival, when compared with RET wild-type cases among patients with medullary thyroid carcinoma (7). www.aacrjournals.org Various FDA-approved multikinase inhibitors that possess anti-RET activity have recently become available: vandetanib, cabozantinib, lenvatinib, ponatinib, sunitinib, regorafenib, and sorafenib (19, 20). Among these agents, one of the earliest studies that demonstrated clinical activity against RET-mutated tumors was a phase I trial with cabozantinib (RET/MET/VEGFR2 inhibitor), which enrolled 37 patients with medullary thyroid carcinoma (8). In that study, 81% (25/31) of analyzed tumors harbored activating RET mutations (including 3 patients with germline RET mutations). Stable disease of at least 6 months or a partial Clin Cancer Res; 2017 Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. OF7 Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Kato et al. response (PR) was observed in 68% (25/37) of patients [PR, 25.9% (17/37)]. Tumor regression was also observed among medullary thyroid carcinomas without identified RET mutations, which could be due to anti-VEGFR2 and anti-MET activities (2 patients had MET amplification) of cabozantinib or because of other unknown aberrations in the RET pathway (8). Cabozantinib was further studied in a double-blind, phase III trial in patients with advanced medullary thyroid carcinoma and demonstrated statistically significant progression-free survival (PFS) when compared with placebo (PFS, 11.2 months versus 4.0 months; HR, 0.28; P < 0.001), with a subgroup analysis demonstrating statistically significant HR only seen among the RET mutation–positive group (22). On the basis of these studies, cabozantinib is currently approved for patients with advanced medullary thyroid carcinoma. In this current report, RET-activating mutations were also found in diverse cancers other than medullary thyroid carcinoma with variable frequencies: anaplastic thyroid [16.7% (2/12)], Merkel cell [10% (1/10)], GIST [3.3% (1/30)], hepatocellular [2.3% (1/44)], endometrial [1.3% (1/79)], colorectal [0.7% (2/300)], and breast [0.2% (1/506)] carcinomas (Table 1 and Supplementary Table S3; Fig. 2). Additional clinical trials targeting diverse cancer types with RET mutations in so-called basket trials may yield insights as to the relevance of histology in the presence of RET mutations (Supplementary Table S1). It is important to also note that medullary thyroid carcinoma patients being targeted with multikinase inhibitors can have frequent initial declines in tumor measurements and markers (calcitonin and carcinoembryonic antigen), followed by short-lived cycling patterns that include an increase in tumor measurements more than 20% above nadir values (which is defined as progressive disease per RECIST version 1.1) with or without increases in tumor markers (36). However, we have previously demonstrated that these fluctuations can be transient, and continued RET inhibition was associated with durable tumor regression (36). RET fusions were the second most common RET aberrations identified [30.7% (27/88); Table 1 and Supplementary Table S3; Fig. 1]. Most fusion partners contain coiled–coil or leucine zipper domains that drive the dimerization or oligomerization of the fusion kinase and lead to ligand-independent RET activation (20). RET fusions have been described in approximately 20% to 40% of papillary thyroid cancers (2, 11), with even higher frequency when associated with radioiodine exposure (60%; ref. 12). More than 10 RET fusion partners have been reported (2). In our study, 8.7% of papillary thyroid carcinomas (2/23) harbored RET fusions (Table 1; Fig. 2). The differences in frequency between previous reports and the current study may be due to small sample size and/or differing detection methods. Recent studies also demonstrated RET fusions in about 1% to 2% of patients with NSCLC, with several of the fusion partners overlapping with those identified in papillary thyroid carcinoma (e.g., CCDC6, KIF5B, NCOA4, and TRIM33; refs. 13–18, 24), which is consistent with findings in this current report (Table 1 and Supplementary Table S3; Fig. 2). Studies analyzing case series have reported that individual patients with NSCLC harboring a CCDC6-RET fusion treated with vandetanib (n ¼ 1; ref. 21) as well as NSCLC bearing TRIM33-RET (n ¼ 1) or KIF5BRET (n ¼ 1) treated with cabozantinib have achieved PRs (15). Herein, we also show a patient with lung adenocarcinoma and a KIF5B-RET fusion, refractory to multiple lines of therapy, who attained a major response (76% regression) with vande- OF8 Clin Cancer Res; 2017 tanib (RET/EGFR/VEGFR2 inhibitor)-based therapy (Fig. 5A). Along with these promising reports (15, 21, 24), there are multiple ongoing phase I and II trials targeting RET fusions in patients with NSCLC and other advanced solid tumors (Supplementary Table S1). Of note, we have identified a patient (papillary thyroid; case #61, Supplementary Table S3) with a sequestosome 1 (SQSTM1)-RET fusion, which, to our knowledge, has not been previously reported (2, 12–18, 20). The functional and clinical relevance of SQSTM1-RET is worth investigating as the SQSTM1 fusion with other partners, such as ALK (37), showed transforming activity in vitro, and there is a case report of a patient with NSCLC and a SQSTM1-NTRK1 fusion demonstrating a durable response to entrectinib (a multikinase inhibitor with targets including TrkA, B, and C; ref. 38). We have also evaluated aberrations that cooccurred with RET. Indeed, 81.8% (72/88) of cases harboring RET aberrations had additional alterations. The most common pathways altered involved TP53-associated genes [59.1% (52/88)], followed by cell cycle–associated genes [39.8% (35/88)], the PI3K signaling pathway [30.7% (27/88)], MAPK effectors [22.7% (20/88)], and other tyrosine kinase families [21.6% (19/88); Fig. 3]. In fact, among 292 coexisting aberrations detected in this report, 80.8% (236/292) were potentially targetable with FDA-approved agents (albeit off label) and an additional 8.2% (24/292) with experimental agents that are under investigation in clinical trials (Supplementary Tables S3 and S7). Moreover, almost all patients [98.6% (71/72)] harboring coaberrations with RET had potentially actionable coaberrations with either FDA-approved or with investigational agents (Supplementary Tables S3 and S7). Although targeting RET aberrations has been reported to be successful, especially when RET was the only identifiable target (15, 21), the current report suggests that therapeutic combination approaches may be necessary to move beyond PRs with limited durability. Several such trials have been suggested or described previously (39–42). Consistent with this notion, we show a patient with sporadic medullary thyroid carcinoma harboring a RET M918T alteration, who had prolonged stable disease on vandetanib (12 months) and had strong positivity for phospho-AKT by IHC. The patient's tumor demonstrated 25% reduction with the addition of everolimus (an mTOR inhibitor; Fig. 5B). Interestingly, RET fusions were mutually exclusive with MAPK signaling pathway (which includes NF1, KRAS, NRAS, and BRAF that were seen with RET mutations/amplifications) and infrequently associated with aberrations in other tyrosine kinase families [7.4% (2/27); Fig. 3; Supplementary Table S6], which is consistent with a previous report (15). However, coaberrations in effectors of MAPK signaling or other tyrosine kinases were readily (greater than 20%) seen among tumors with either RET mutations or amplifications (Fig. 3; Supplementary Table S6). The extent to which this holds true in larger groups of patients merits investigation. There are several limitations to the current data. First, correlations with overall disease outcome were not feasible, as the data were not clinically annotated. Second, the impact of germline mutations [especially important for medullary thyroid carcinoma and pheochromocytoma that can be associated with MEN (9, 10)] was not evaluable. Third, the possibility of sample size bias exists as the number of cases in each Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 RET Aberrations in Cancer malignancy relied on the number of specimens submitted by physicians for NGS. Finally, the diagnosis was determined on the basis of the submitting physician's designation. However, despite these limitations, the current report provides a large and comprehensive analysis of RET aberrations in diverse cancers. In conclusion, we have evaluated 4,871 patients with diverse cancers and shown that aberrations in RET are found in 1.8% (88/ 4,871) of cases. We have also identified a novel SQSTM1-RET fusion (n ¼ 1) in a papillary thyroid tumor. Most patients [81.8% (72/88)] had coexisting genomic aberrations that accompanied their RET alterations. In the vast majority of individuals [98.6% (71/72)], at least one of the coalterations was pharmacologically tractable. Although various trials targeting RET aberrations are ongoing (Supplementary Table S1), the current report suggests that individualized cotargeting of multiple aberrant genes along with RET inhibition may be required for optimal clinical outcome. Disclosure of Potential Conflicts of Interest V. Subbiah reports receiving commercial research grants from Novartis. S.K. Elkin and J.L. Carter have ownership interest (including patents) in N-of-One. R. Kurzrock is an employee of and has ownership interests (including patents) in Novena Inc. and Curematch, Inc.; is a consultant/ advisory board member for Actuate Therapeutics, Squenom, and Xbiotech; and reports receiving commercial research grants from Foundation Medi- cine, Genentech, Guardant, Merck, Pfizer, and Squenom. No potential conflicts of interest were disclosed by the other authors. Authors' Contributions Conception and design: S. Kato, E. Marchlik, S.K. Elkin, J.L. Carter, R. Kurzrock Development of methodology: S. Kato, E. Marchlik, S.K. Elkin Acquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): V. Subbiah, E. Marchlik, S.K. Elkin Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): S. Kato, V. Subbiah, E. Marchlik, S.K. Elkin, R. Kurzrock Writing, review, and/or revision of the manuscript: S. Kato, V. Subbiah, E. Marchlik, S.K. Elkin, J.L. Carter, R. Kurzrock Administrative, technical, or material support (i.e., reporting or organizing data, constructing databases): V. Subbiah Study supervision: R. Kurzrock Grant Support This study was funded in part by the Joan and Irwin Jacobs fund. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Received July 7, 2016; revised August 22, 2016; accepted September 4, 2016; published OnlineFirst September 28, 2016. References 1. Airaksinen MS, Saarma M. The GDNF family: signalling, biological functions and therapeutic value. Nat Rev Neurosci 2002;3:383–94. 2. Santoro M, Melillo RM, Fusco A. RET/PTC activation in papillary thyroid carcinoma: European Journal of Endocrinology Prize Lecture. Eur J Endocrinol 2006;155:645–53. 3. Houvras Y. Completing the Arc: targeted inhibition of RET in medullary thyroid cancer. J Clin Oncol 2012;30:200–2. 4. Amiel J, Sproat-Emison E, Garcia-Barcelo M, Lantieri F, Burzynski G, Borrego S, et al. Hirschsprung disease, associated syndromes and genetics: a review. J Med Genet 2008;45:1–14. 5. Moura MM, Cavaco BM, Pinto AE, Domingues R, Santos JR, Cid MO, et al. Correlation of RET somatic mutations with clinicopathological features in sporadic medullary thyroid carcinomas. Br J Cancer 2009; 100:1777–83. 6. Dvorakova S, Vaclavikova E, Sykorova V, Vcelak J, Novak Z, Duskova J, et al. Somatic mutations in the RET proto-oncogene in sporadic medullary thyroid carcinomas. Mol Cell Endocrinol 2008;284:21–7. 7. Elisei R, Cosci B, Romei C, Bottici V, Renzini G, Molinaro E, et al. Prognostic significance of somatic RET oncogene mutations in sporadic medullary thyroid cancer: a 10-year follow-up study. J Clin Endocrinol Metab 2008;93:682–7. 8. Kurzrock R, Sherman SI, Ball DW, Forastiere AA, Cohen RB, Mehra R, et al. Activity of XL184 (cabozantinib), an oral tyrosine kinase inhibitor, in patients with medullary thyroid cancer. J Clin Oncol 2011;29:2660–6. 9. Moline J, Eng C. Multiple endocrine neoplasia type 2: an overview. Genet Med 2011;13:755–64. 10. Jhiang SM. The RET proto-oncogene in human cancers. Oncogene 2000; 19:5590–7. 11. Ciampi R, Nikiforov YE. RET/PTC rearrangements and BRAF mutations in thyroid tumorigenesis. Endocrinology 2007;148:936–41. 12. Rabes HM, Demidchik EP, Sidorow JD, Lengfelder E, Beimfohr C, Hoelzel D, et al. Pattern of radiation-induced RET and NTRK1 rearrangements in 191 post-chernobyl papillary thyroid carcinomas: biological, phenotypic, and clinical implications. Clin Cancer Res 2000;6:1093–103. 13. Takeuchi K, Soda M, Togashi Y, Suzuki R, Sakata S, Hatano S, et al. RET, ROS1 and ALK fusions in lung cancer. Nat Med 2012;18:378–81. 14. Wang R, Hu H, Pan Y, Li Y, Ye T, Li C, et al. RET fusions define a unique molecular and clinicopathologic subtype of non-small-cell lung cancer. J Clin Oncol 2012;30:4352–9. www.aacrjournals.org 15. Drilon A, Wang L, Hasanovic A, Suehara Y, Lipson D, Stephens P, et al. Response to cabozantinib in patients with RET fusion-positive lung adenocarcinomas. Cancer Discov 2013;3:630–5. 16. Kohno T, Ichikawa H, Totoki Y, Yasuda K, Hiramoto M, Nammo T, et al. KIF5B-RET fusions in lung adenocarcinoma. Nat Med 2012;18:375–7. 17. Lipson D, Capelletti M, Yelensky R, Otto G, Parker A, Jarosz M, et al. Identification of new ALK and RET gene fusions from colorectal and lung cancer biopsies. Nat Med 2012;18:382–4. 18. Suehara Y, Arcila M, Wang L, Hasanovic A, Ang D, Ito T, et al. Identification of KIF5B-RET and GOPC-ROS1 fusions in lung adenocarcinomas through a comprehensive mRNA-based screen for tyrosine kinase fusions. Clin Cancer Res 2012;18:6599–608. 19. Mulligan LM. RET revisited: expanding the oncogenic portfolio. Nat Rev Cancer 2014;14:173–86. 20. Shaw AT, Hsu PP, Awad MM, Engelman JA. Tyrosine kinase gene rearrangements in epithelial malignancies. Nat Rev Cancer 2013;13: 772–87. 21. Falchook GS, Ordonez NG, Bastida CC, Stephens PJ, Miller VA, Gaido L, et al. Effect of the RET inhibitor vandetanib in a patient with RET fusionpositive metastatic non-small-cell lung cancer. J Clin Oncol 2016;34: e141–4. 22. Elisei R, Schlumberger MJ, Muller SP, Schoffski P, Brose MS, Shah MH, et al. Cabozantinib in progressive medullary thyroid cancer. J Clin Oncol 2013;31:3639–46. 23. Subbiah V, Meric-Bernstam F, Mills GB, Shaw KR, Bailey AM, Rao P, et al. Next generation sequencing analysis of platinum refractory advanced germ cell tumor sensitive to Sunitinib (Sutent(R)) a VEGFR2/PDGFRbeta/c-kit/FLT3/RET/CSF1R inhibitor in a phase II trial. J Hematol Oncol 2014;7:52. 24. Subbiah V, Berry J, Roxas M, Guha-Thakurta N, Subbiah IM, Ali SM, et al. Systemic and CNS activity of the RET inhibitor vandetanib combined with the mTOR inhibitor everolimus in KIF5B-RET rearranged non-small cell lung cancer with brain metastases. Lung Cancer 2015;89:76–9. 25. Hong DS, Cabanillas ME, Wheler J, Naing A, Tsimberidou AM, Ye L, et al. Inhibition of the Ras/Raf/MEK/ERK and RET kinase pathways with the combination of the multikinase inhibitor sorafenib and the farnesyltransferase inhibitor tipifarnib in medullary and differentiated thyroid malignancies. J Clin Endocrinol Metab 2011;96:997–1005. Clin Cancer Res; 2017 Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. OF9 Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 Kato et al. 26. Hong DS, Sebti SM, Newman RA, Blaskovich MA, Ye L, Gagel RF, et al. Phase I trial of a combination of the multikinase inhibitor sorafenib and the farnesyltransferase inhibitor tipifarnib in advanced malignancies. Clin Cancer Res 2009;15:7061–8. 27. Hong D, Ye L, Gagel R, Chintala L, El Naggar AK, Wright J, et al. Medullary thyroid cancer: targeting the RET kinase pathway with sorafenib/tipifarnib. Mol Cancer Ther 2008;7:1001–6. 28. Frampton GM, Fichtenholtz A, Otto GA, Wang K, Downing SR, He J, et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat Biotechnol 2013;31: 1023–31. 29. Thomas RK, Nickerson E, Simons JF, Janne PA, Tengs T, Yuza Y, et al. Sensitive mutation detection in heterogeneous cancer specimens by massively parallel picoliter reactor sequencing. Nat Med 2006;12:852–5. 30. Wagle N, Berger MF, Davis MJ, Blumenstiel B, Defelice M, Pochanard P, et al. High-throughput detection of actionable genomic alterations in clinical tumor samples by targeted, massively parallel sequencing. Cancer Discov 2012;2:82–93. 31. Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov 2012;2:401–4. 32. Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal 2013;6:pl1. 33. Cuccuru G, Lanzi C, Cassinelli G, Pratesi G, Tortoreto M, Petrangolini G, et al. Cellular effects and antitumor activity of RET inhibitor RPI-1 on MEN2A-associated medullary thyroid carcinoma. J Natl Cancer Inst 2004;96:1006–14. OF10 Clin Cancer Res; 2017 34. Muzza M, Cordella D, Bombled J, Bressac-de Paillerets B, Guizzardi F, Francis Z, et al. Four novel RET germline variants in exons 8 and 11 display an oncogenic potential in vitro. Eur J Endocrinol 2010;162: 771–7. 35. Chau NG, Haddad RI. Vandetanib for the treatment of medullary thyroid cancer. Clin Cancer Res 2013;19:524–9. 36. Kurzrock R, Atkins J, Wheler J, Fu S, Naing A, Busaidy N, et al. Tumor marker and measurement fluctuations may not reflect treatment efficacy in patients with medullary thyroid carcinoma on long-term RET inhibitor therapy. Ann Oncol 2013;24:2256–61. 37. Takeuchi K, Soda M, Togashi Y, Ota Y, Sekiguchi Y, Hatano S, et al. Identification of a novel fusion, SQSTM1-ALK, in ALK-positive large B-cell lymphoma. Haematologica 2011;96:464–7. 38. Farago AF, Le LP, Zheng Z, Muzikansky A, Drilon A, Patel M, et al. Durable clinical response to entrectinib in NTRK1-rearranged non-small cell lung cancer. J Thorac Oncol 2015;10:1670–4. 39. Lazar V, Rubin E, Depil S, Pawitan Y, Martini JF, Gomez-Navarro J, et al. A simplified interventional mapping system (SIMS) for the selection of combinations of targeted treatments in non-small cell lung cancer. Oncotarget 2015;6:14139–52. 40. Schilsky RL. Highlights from the 2015 WIN Symposium: novel targets, innovative agents, and advanced technologies-a WINning strategy? Ecancermedicalscience 2015;9:564. 41. Schwaederle M, Parker BA, Schwab RB, Daniels GA, Piccioni DE, Kesari S, et al. Precision Oncology: The UC San Diego Moores Cancer Center PREDICT Experience. Mol Cancer Ther 2016;15:743–52. 42. Kurzrock R, Giles FJ. Precision oncology for patients with advanced cancer: the challenges of malignant snowflakes. Cell Cycle 2015;14:2219–21. Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research. Published OnlineFirst September 28, 2016; DOI: 10.1158/1078-0432.CCR-16-1679 RET Aberrations in Diverse Cancers: Next-Generation Sequencing of 4,871 Patients Shumei Kato, Vivek Subbiah, Erica Marchlik, et al. Clin Cancer Res Published OnlineFirst September 28, 2016. Updated version Supplementary Material E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-16-1679 Access the most recent supplemental material at: http://clincancerres.aacrjournals.org/content/suppl/2016/09/28/1078-0432.CCR-16-1679.DC1 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2016 American Association for Cancer Research.