Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
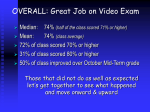
[ research report ] GLENN S. FLEISIG, PhD1 • BECKY BOLT, MS2 • DAVE FORTENBAUGH, MS3 KEVIN E. WILK, DPT4 • JAMES R. ANDREWS, MD5 Biomechanical Comparison of Baseball Pitching and Long-Toss: Implications for Training and Rehabilitation F ollowing a shoulder or elbow injury or surgery, a baseball pitcher or position player must progress through a multiphase rehabilitation program to return to competition. Such programs often begin with exercises to restore range of motion and strength of the affected joint, followed by more functional and aggressive rehabilitation exercises. The latter phases incorporate functional exercises, such as plyometrics and highspeed training, to prepare the player TTSTUDY DESIGN: Controlled laboratory study. TTOBJECTIVES: To test for kinematic and kinetic differences between baseball pitching from a mound and long-toss on flat ground. TTBACKGROUND: Long-toss throws from flat ground are commonly used by baseball pitchers for rehabilitation, conditioning, and training. However, there is controversy over the biomechanics and functionality of such throws. TTMETHODS: Seventeen healthy, college baseball pitchers pitched fastballs 18.4 m from a mound to a strike zone, and threw 37 m, 55 m, and maximum distance from flat ground. For the 37-m and 55-m throws, participants were instructed to throw “hard, on a horizontal line.” For the maximumdistance throw, no constraint on trajectory was given. Kinematics and kinetics were measured with a 3-dimensional, automated motion analysis system. Repeated-measures analyses of variance, with post hoc paired t tests, were used to compare the 4 throw types within pitchers. TTRESULTS: At foot contact, the participant’s shoulder line was nearly horizontal when pitching The interval throwing program starts skeletally mature players at a throwing distance of 45 ft (14 m) and progressively increases it to 180 ft (55 m).3,22 For all flat-ground throws, the player is verbally instructed to use “crow-hop” footwork, to throw SUPPLEMENTAL VIDEO ONLINE to throw. An interval long-toss “on a line” (a hard throw with a throwing program is the halllow trajectory), and to use proper mark of the return-to-activity phase.28,29 mechanics.3,22,28,29 The use of proper mechanics—the mechanics used by healthy players—is a critical aspect of the interfrom a mound and became progressively more val throwing program. It has been suginclined as throwing distance increased. At arm gested that pitching coaches and sports cocking, the greatest amount of shoulder external biomechanists provide a valuable service rotation (mean SD, 180° 11°), elbow flexion on a rehabilitation team to ensure proper (109° 10°), shoulder internal rotation torque mechanics.22 Thus an understanding of (101 17 Nm), and elbow varus torque (100 18 Nm) were measured during the maximum-distance healthy throwing mechanics is essential throws. Elbow extension velocity was also greatest for the rehabilitation of an injured player. for the maximum-distance throws (2573°/s If the player is a pitcher, the flat-ground 203°/s). Forward trunk tilt at the instant of ball throwing phases of the rehabilitation release decreased as throwing distance increased. program are followed by throwing off TTCONCLUSION: Hard, horizontal, flat-ground the mound. During the off-the-mound throws have biomechanical patterns similar to throwing phase, a pitcher progresses those of pitching and are, therefore, reasonable from partial-effort to full-effort pitches. exercises for pitchers. However, maximum-distance Theoretically, the progression of throwthrows produce increased torques and changes in ing phases allows an injured athlete kinematics. Caution is, therefore, advised in the to gradually recover his arm flexibility, use of these throws for rehabilitation and training. arm strength, and proper throwing meJ Orthop Sports Phys Ther 2011;41(5):296-303, chanics. 3,22,28,29 Interval throwing proEpub 5 January 2011. doi:10.2519/jospt.2011.3568 grams have been utilized to effectively TTKEY WORDS: crow-hop, elbow, interval throwing return pitchers and position players to program, kinematics, shoulder baseball.28 Research Director, American Sports Medicine Institute, Birmingham, AL. 2Biomechanist, American Sports Medicine Institute, Birmingham, AL. 3Biomechanist, American Sports Medicine Institute, Birmingham, AL. 4Associate Clinical Director, Champion Sports Medicine, Physiotherapy Associates, Birmingham, AL. 5Medical Director, American Sports Medicine Institute, Birmingham, AL. This study was approved by the Institutional Review Board of St Vincent’s Health System, Birmingham, AL. The authors have no financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript. Address correspondence to Dr Glenn S. Fleisig, Research Director, American Sports Medicine Institute, 833 St. Vincent’s Drive, Suite 100, Birmingham, AL 35205. E-mail: [email protected] 1 296 | may 2011 | volume 41 | number 5 | journal of orthopaedic & sports physical therapy 41-05 Fleisig.indd 296 4/20/2011 2:15:19 PM Flat-ground throwing is also used to improve strength and conditioning of healthy baseball players, especially pitchers. Theoretically, long-distance flat-ground throwing would require the pitcher’s arm to generate greater force, torque, range of motion, and speed than pitching would. Therefore, long-distance, flat-ground throwing may be used to train a pitcher to have greater arm strength, arm flexibility, arm speed, and ultimately pitch speed. Throwing programs for healthy players vary greatly. Some programs limit throws to a specific distance (55 m, for example), while others include maximum-distance throws. Some programs require the players to throw on a line, while others recommend throwing on an arc. Flat-ground throwing has been part of baseball rehabilitation and conditioning for decades. Recently, however, some have asked whether flat-ground throwing might be ineffective or even harmful for baseball pitchers and position players. There has also been controversy over limitations on throwing distance. While pitching biomechanics has been studied extensively, little is known about longtoss throwing biomechanics. In the only previous study on long-toss baseball throwing, Miyanishi et al20 compared the kinematics of 24 college baseball players throwing a ball on a horizontal line as fast as possible against throwing a ball as far as possible. No previous study has compared the biomechanics of flat-ground throwing and pitching. Therefore, it is still not known whether baseball pitchers use similar kinematics and kinetics during long-toss and pitching. Thus, the theoretical benefits of long-toss for pitchers remain unsubstantiated. The purpose of this study was to compare the biomechanics of pitching and long-toss throwing. The present study tested the hypotheses that there are kinematic (motion) and kinetic (torque and force) differences in the throwing shoulder and elbow between pitching and throwing various flat-ground distances. FIGURE. (A) Collection of long-toss data. (B) Collection of pitching data. METHODS P itchers from 3 college baseball teams were recruited for the study. Players who had been injured during the previous 12 months and those who pitched with sidearm or “submarine” mechanics were excluded. Seventeen baseball pitchers met the criteria and agreed to participate. All participants were experienced with long-toss, as all 3 colleges used long-toss in their conditioning and warm-ups. Each participant completed an informed consent form and provided medical history, physical information, and baseball background. The pitchers were (mean SD) 20.6 1.2 years of age and 186 6 cm in height, and had a mass of 89 10 kg. The study was approved by The Institutional Review Board of St Vincent’s Health System, Birmingham, AL. Each participant was tested during 2 sessions. For each session, 21 reflective markers (10 mm in diameter) were attached to the participant. This included markers attached bilaterally to the distal end of the third metatarsal, lateral malleolus, lateral femoral epicondyle, greater trochanter, lateral superior tip of the acromion, lateral humeral epicondyle, and journal of orthopaedic & sports physical therapy | volume 41 | number 5 | may 2011 | 297 41-05 Fleisig.indd 297 4/20/2011 2:15:21 PM [ research report ] TABLE 1 Comparison of Position Data Among Throws* Fastball Pitch (18.4 m) 37-m Throw 55-m Throw Maximum-Distance Throw (80 ± 9 m) Differences Foot contact Elbow flexion 78 17 79 18 79 18 86 20 Shoulder external rotation 53 30 56 28 60 28 58 26 Shoulder abduction 96 10 98 10 99 10 98 9 Shoulder horizontal abduction 21 11 19 12 19 11 21 11 Upper trunk tilt 6 7 13 9 15 8 24 8 Pelvis angle 37 12 37 11 39 11 40 11 Front knee flexion 47 9 46 8 44 7 42 6 Stride length, % participant's height 80 4 79 6 80 6 80 7 Foot position, cm 25 12 16 14 13 15 5 18 c,e,f† a,b,c,d,e,f† b,c,d,e† a,b,c,d,e,f† Arm cocking Maximum elbow flexion 101 11 103 10 104 11 109 10 c,e,f† Maximum shoulder external rotation 174 10 174 10 176 10 180 11 c,d,e,f† 17 6 18 7 18 7 17 7 Maximum shoulder horizontal adduction Ball release Shoulder abduction 88 7 89 9 89 9 88 8 Forward trunk tilt 34 8 27 8 25 7 18 8 Lateral trunk tilt 25 8 24 8 24 8 26 7 Front knee flexion 37 13 36 12 33 13 31 12 a,b,c,d,e,f† b,c,d,e,f† *Values are mean SD degrees, except where otherwise indicated. † Analysis of variance revealed significant difference among throws (P<.01). Post hoc t tests indicated significant differences between (a) pitch and 37-m throw, (b) pitch and 55-m throw, (c) pitch and maximum-distance throw, (d) 37-m and 55-m throws, (e) 37-m and maximum-distance throws, and ( f ) 55-m and maximum-distance throws. ulnar styloid. Additional markers were placed on the medial humeral epicondyle, radial styloid, and dorsal surface of the hand on the throwing extremity. Four markers were attached to a baseball hat on the front, back, top, and right sides of the head. The reflective markers were tracked with an 8-camera automated motion capture system (Eagle System, Motion Analysis Corporation, Santa Rosa, CA). Ball velocity was measured by a Stalker Sport radar gun (Stalker Radar, Plano, TX). For the first testing session, the motion capture system was set up in the outfield of a college baseball field. The 8 cameras were arranged in a ring around a designated throwing area. Because the motion capture system could not properly filter out sunlight, data collection for this session occurred at night under artificial stadium lighting (FIGURE). Pilot testing confirmed that the marker track- ing in this outdoor setup was reliable and the calibration coefficients were similar to values recorded during indoor testing. Distances were measured and marked from the throwing area. The x-axis was the direction of throwing, the z-axis was the vertical axis, and y was their cross product (z × x). Participants wore tight shorts, socks, and cleats. Reflective markers were attached to a pair of participants, who, by throwing to each other, took as much time as they needed to warm up. The pair started by throwing close to each other and progressively increased their distance apart, until they were throwing near their maximum distance. Each participant was then tested for five 37-m (120-ft), five 55-m (180-ft), and 5 maximum-distance throws to a coach. Each pitcher completed a total of 15 throws (5 throws at 3 distances), which provided a sufficient sample of data, without allowing the second pitcher in the pair to cool down while waiting his turn to be tested. Each participant was allowed to use the crow-hop footwork that he was comfortable with, as there is no description of crow-hop footwork in the published literature, and coaches, physical therapists, and athletic trainers have given varied opinions. While most agree that crowhop footwork is a sequence of steps of the front foot, back foot, then front foot, there is no consensus on whether the back foot steps behind, in front, or next to the front foot. The participant was instructed to throw “hard, on a horizontal line,” when performing the 37-m and 55-m throws. The participant was told to get the maximum distance on his final 5 throws, with no constraints on trajectory. The second testing session took place in an indoor biomechanics laboratory. The 8 cameras were mounted on the walls surrounding a portable pitching mound (FIGURE, ONLINE VIDEO). A home plate strike 298 | may 2011 | volume 41 | number 5 | journal of orthopaedic & sports physical therapy 41-05 Fleisig.indd 298 4/20/2011 2:15:22 PM TABLE 2 Comparison of Peak Velocity Data Among Throws* Maximum-Distance Throw Fastball Pitch (18.4 m) 37-m Throw 55-m Throw (80 ± 9 m) Differences Pelvis angular velocity, °/s 568 67 586 69 602 73 621 84 a,b,c,d† Upper trunk angular velocity, °/s 1120 99 1141 100 1153 99 1179 98 a,b,c,d† Shoulder internal rotation velocity, °/s 7640 1173 7590 1214 8139 1609 80401211 Elbow extension velocity, °/s 2480 255 2492 204 2540 176 2603 164 37 2 37 2 37 2 36 2 Ball velocity, m/s b,c† *Values are mean SD. † Analysis of variance revealed significant difference among throws (P<.01). Post hoc t tests indicated significant differences between (a) pitch and 55-m throw, (b) pitch and maximum-distance throw, (c) 37-m and maximum-distance throw, and (d) 55-m and maximum-distance throw. zone was placed 18.4 m (60.5 ft) from the pitching rubber. Participants wore tight shorts, socks, and athletic shoes. Reflective markers were attached to each participant, and each was allowed the time he needed to warm up. The participant then threw 10 maximum-effort fastball pitches for data collection. Because players warmed up individually before testing, there was no risk of a warmed-up player cooling down while waiting to be tested. Twenty-five parameters (16 position, 5 velocity, and 4 kinetic values) were calculated for each trial, according to methods previously described.5-10,14,16,17,19,25 Nine position parameters were measured at the instant of foot contact: elbow flexion, shoulder external rotation, shoulder abduction, shoulder horizontal abduction, upper trunk tilt, pelvis angle, front knee flexion, stride length, and foot position. Upper trunk tilt was defined as the angle between a line through the 2 shoulder joints and the horizontal plane. Pelvis angle was the angle between a line through the 2 hips and the x-axis. Stride length was the distance between the rear ankle’s location when the front leg was lifted to its maximum height and the front ankle’s location when the front foot landed. (For a right-handed pitcher, his “rear ankle” is his right ankle.) Foot position was the distance between the back ankle when it was against the pitching rubber and the front ankle at the time of foot contact, in the y direction. Three position parameters were calculated when the arm was cocked back: maximum elbow flexion, maximum shoulder external rotation, and maximum shoulder horizontal adduction. The other 4 position parameters were measured at the time of ball release: shoulder abduction, forward trunk tilt, side trunk tilt, and front knee flexion. Forward trunk tilt was the angle between the spine (measured as the line from the mid-hips to the mid-shoulders) and the z-axis, projected in the xz-plane. Lateral trunk tilt was the angle between the spine and the z-axis, projected in the yz-plane. Maximum values of pelvis angular velocity, upper trunk angular velocity, elbow extension velocity, shoulder internal rotation velocity, and ball velocity were computed. Pelvis and upper trunk velocities were measured by their rotations in the global reference frame. Elbow and shoulder velocities were computed as the rate of change of the joint angle. Maximum values for elbow and shoulder kinetics were computed. Values were reported as the force, or torque, applied by the proximal segment onto the distal segment at the joint. Though this convention was the opposite of that reported in a few previous papers,2,23,26 it was consistent with most studies.1,5-9,14-19,25,30 Maximum values were reported for elbow varus torque and shoulder internal rotation torque when the arm was cocked, and for elbow flexion torque and shoulder proximal force near the time of ball release. For each participant, mean values were computed for each throw type: pitching, 37 m, 55 m, and maximum distance. The differences among mean val- ues for the 4 throw types were analyzed for each parameter with a repeatedmeasures analysis of variance (ANOVA). When the ANOVA revealed a significant difference, post hoc paired t tests were performed among the throw types. To protect against type I error, an alpha level of .01 was used for all statistical analyses. RESULTS T he mean SD value for the maximum-distance throw among the 17 participants was 80 9 m (262 30 ft) and the range was 65 to 96 m (213315 ft). Differences in position parameters are shown in TABLE 1. There were 4 significant differences at the instant of foot contact: elbow flexion was greatest for the maximum-distance throw, and, as throwing distance increased from pitching to maximum distance, upper trunk tilt increased, while front knee flexion and foot position decreased. When the arm was in the cocked position, elbow flexion and shoulder external rotation were greatest for the maximum-distance throw. At the time of ball release, as throwing distance increased, both forward trunk tilt and front knee flexion decreased. Differences in velocity parameters are shown in TABLE 2. The pelvis and upper trunk rotational velocities were greatest for the maximum-distance throw. They were also significantly greater in the 55-m throws compared to the pitch. The elbow extension velocity was significantly greater for the maximum-distance journal of orthopaedic & sports physical therapy | volume 41 | number 5 | may 2011 | 299 41-05 Fleisig.indd 299 4/20/2011 2:15:23 PM [ research report ] TABLE 3 Comparison of Joint Forces and Torques Among Throws* Fastball Pitch (18.4 m) 37-m Throw 55-m Throw Maximum-Distance Throw (80 ± 9 m) Differences Arm cocking Elbow varus torque, Nm 92 19 90 18 95 19 100 18 a,b,c† Shoulder internal rotation torque, Nm 94 18 92 17 96 18 100 18 a,b,c† Ball release Elbow flexion torque, Nm 47 5 47 8 47 8 48 8 Shoulder proximal force, N 1172 159 1087 184 1139 202 1092 129 *Values are mean SD. † Analysis of variance revealed significant difference among throws (P<.01). Post hoc t tests indicated significant differences between (a) pitch and maximumdistance throw, (b) 37-m and 55-m throws, and (c) 37-m and maximum-distance throws. throws compared to both the pitch and the 37-m distance throw. No significant differences were detected among throw types in ball velocity. Differences in joint forces and torques are shown in TABLE 3. Peak elbow varus torque and peak shoulder internal rotation torque were both greater in the maximum-distance throw than in the fastball pitch and 37-m throw. These torques were also greater in the 55-m throw than in the 37-m throw. DISCUSSION T he data supported the hypotheses that there are kinematic and kinetic differences among the 4 throw types tested: pitching (18.4 m) from a mound, flat-ground throwing on a horizontal line at relatively short (37 m) distance, flat-ground throwing on a horizontal line at medium (55 m) distance, and flat-ground throwing at long (maximum) distance. As throwing distance increased, the player used a more inclined (more upward trunk tilt) position at foot contact. Also, as throwing distance increased, the player seemed to rely less on rotation in the sagittal plane (less forward trunk tilt and less knee flexion) and more on rotation in the transverse plane (greater pelvis angular velocity, upper trunk angular velocity, elbow flexion, and elbow extension velocity). Longer throws also produced greater elbow and shoulder torques in the arm-cocked position. The greater rotations in the transverse plane might have been caused by the greater arm-cocking torques; but this cause-and-effect relationship was beyond the focus of the current study. There were a greater number of significant differences between the maximum-distance throws and the other throws. The pitching biomechanics of the current study was consistent with previously published college pitching data.1,11,16,17,26 Flat-ground biomechanics in the current study showed some of the patterns found by Miyanishi et al.20 At the time of foot contact, both studies found significantly greater (7°) elbow flexion for the maximum-distance throws compared to the other long-toss distances but no difference in shoulder abduction between the distances. During the arm-cocking phase, each study found that maximum shoulder external rotation significantly increased as the throwing distance increased. However, the magnitude of this increase was noticeably greater in the Miyanishi et al20 study than in the current study (13° versus 4°, respectively). At the time of ball release, each study reported less forward trunk tilt (15° in the Miyanishi et al20 study and 7° in the current study) for the maximum-distance throws. In addition, Miyanishi et al20 also reported that, at ball release, maximum-distance throws had less shoulder abduction (24°) and greater lateral trunk tilt (9°), while the current study did not find significant differences for these parameters. Elbow Injury Mechanisms and Rehabilitation Previous studies have shown that maximum elbow varus torque in pitching occurs near the time of maximum shoulder external rotation and that this torque is associated with maximum tensile force in the ulnar collateral ligament (UCL).14,21,27 Repetition of high force in the UCL associated with high varus torque can lead to gradual attenuation of the UCL.2,18 Thus the progression of throwing phases during rehabilitation after UCL surgery should allow the athlete to regain his pitching mechanics, while progressively loading the UCL graft. Because the greatest elbow varus torque occurred during maximum-distance throwing, these throws should be avoided following UCL reconstruction or at least delayed until the clinician has found that the UCL graft has adequately healed. Similarly, caution is advised for maximum-distance throwing in rehabilitation following chondral defects in the lateral elbow, as varus torque is associated with compressive force between the radial head and the capitellum.14,23,27 Osteophytes in the posteromedial elbow result from varus torque during rapid elbow extension.2,14,27 Because maximumdistance throws exhibited both the greatest varus torque and the greatest elbow extension velocity, such throws should not be used early in rehabilitation after posteromedial osteophyte removal. 300 | may 2011 | volume 41 | number 5 | journal of orthopaedic & sports physical therapy 41-05 Fleisig.indd 300 4/20/2011 2:15:25 PM Shoulder Injury Mechanisms and Rehabilitation During arm cocking, a pitcher’s shoulder is abducted, horizontally abducted, and externally rotated. These motions produce tension in the shoulder’s anterior capsule.15,27 The current study reported no differences in abduction or horizontal abduction among the different throws; however, there was increased maximum shoulder external rotation for maximumdistance throws. Maximum-distance throws also produced the greatest internal rotation torque, which occurred near the time of maximum shoulder external rotation. Because of the increased shoulder external rotation and shoulder internal rotation torque, maximum-distance throwing should be avoided or delayed in rehabilitation after procedures such as anterior capsular plication, capsulolabral repair, or labral repair, until adequate tissue healing has occurred. Excessive external rotation of the abducted shoulder is also the mechanism for symptoms of internal impingement of the infraspinatus and supraspinatus.30 Therefore, caution is advised for use of maximum-distance throwing in the rehabilitation of infraspinatus injury. While certain aspects of pitching mechanics vary among successful pitchers, shoulder abduction is consistently near 90° at both foot contact and ball release.9,10,16 Excessive abduction may result in subacromial impingement of the bursa. Insufficient abduction is also a risk factor due to misalignment of force vectors among the deltoid, rotator cuff, and other shoulder stabilizers. Because no differences were reported in shoulder abduction among the various throws in the current study, there is no specific concern in throw types for rehabilitation from these injuries. Fleisig et al14 described the mechanism of injury for a superior labral anteriorto-posterior (SLAP) lesion as distal force applied by the long head of the biceps to the superior labrum. This biceps force is applied at its origin, near the time of ball release, when the biceps is contracting to both resist glenohumeral distraction and decelerate elbow extension. Burkhart and Morgan4 proposed an alternate SLAP lesion mechanism, in which the biceps tendon “peels back” the anterior labrum. Shepard et al24 measured in vitro strength of the biceps-labral complex during both the distal force and peelback mechanisms, and concluded that SLAP lesions most likely occur from repetition of both peel-back and distal forces. Shoulder external rotation and shoulder internal rotation torque may be related to the peel-back mechanism of the cocked arm, and shoulder proximal force and elbow flexion torque may be related to the biceps pull-out force near the time of ball release. Although the current study found no differences in ball release kinetics (shoulder proximal force and elbow flexion torque), both shoulder external rotation and shoulder internal rotation torque were greatest in maximum-distance throws. Thus longer distance throwing should be delayed until the clinician feels that the glenoid labrum has had adequate time to heal. Maximum-distance throws may create the largest peel-back forces and should be avoided, or at least delayed, after SLAP repair. Near the time of ball release, a large proximal force is produced at the shoulder to resist distraction. The combination of this proximal force and the rapid internal rotation velocity at the shoulder may produce a grinding of the humeral head against the anterior glenoid labrum.14 The current study found no differences in proximal force or internal rotation velocity among throw types. However, because maximum-distance throws were identified in the current study as being the most stressful to the anterior labrum during arm cocking, caution is advised for use of maximumdistance throws after any anterior labrum injury. Training It has often been hypothesized that long-distance throwing is beneficial to the throwing athlete for increasing flexibility, ball speed, arm strength, and endurance. A previous comparison of adult pitchers with high versus low ball velocity demonstrated 3 kinematic differences.19 Namely, pitchers with high ball velocity had greater maximum shoulder external rotation, forward trunk tilt at the time of ball release, and lead knee extension velocity. For longer throws, the current study found greater maximum shoulder external rotation but less forward trunk tilt. Furthermore, the current study found no differences in ball velocity for various throw distances, and approximately 10° of knee extension from foot contact to ball release for all throws. Thus the current study did not find greater similarity between particular distances of throws and the pitching mechanics of pitchers with high ball velocity. In another study investigating changes within individual pitchers, several characteristics correlated with greater ball velocity.25 Kinetic values near the time of ball release (elbow flexion torque, shoulder proximal force, and elbow proximal force) increased with pitch velocity. For pitches with higher ball velocity, at the time of ball release, pitchers displayed decreased shoulder horizontal adduction, decreased shoulder abduction, and increased forward trunk tilt. The current study showed no differences among throw types in ball velocity, kinetics at the time of ball release, shoulder horizontal adduction, or abduction. Forward trunk tilt decreased with throwing distance. Thus, the current study did not indicate that particular throwing distances were superior in training to increase ball velocity. The current study did find greater range of motion (maximum shoulder external rotation), speed (angular velocities of the pelvis, upper trunk, and elbow), and arm torque (elbow varus and shoulder internal rotation) in long-toss, which indicates that these throws may be beneficial in training. However, longdistance throws also produced changes in throwing mechanics at foot contact (up- journal of orthopaedic & sports physical therapy | volume 41 | number 5 | may 2011 | 301 41-05 Fleisig.indd 301 4/20/2011 2:15:26 PM [ hill trunk tilt and foot position) and at ball release (forward trunk tilt and front knee flexion). Furthermore, maximumdistance throws produced the greatest elbow and shoulder torques, without any change in ball velocity, making these the least efficient throws, as they produced the most torque for comparable ball velocity. The benefits or detriments of longtoss cannot truly be determined without prospective studies comparing performance and safety between groups trained with and without long-toss. Limitations and Future Direction The current study’s findings suggest that the 55-m distance may be a good choice for the longer throw on a line, as all participants were able to throw this distance without increasing the ball trajectory. With unconstrained trajectories, all participants threw 65 m or greater. However, the fact that only 3 distances (37 m, 55 m, and maximum distance) were tested for flat-ground throws was a limitation of the current study. Also, the effects of throwing distance and trajectory were not separated. Studying players with a variety of crow-hop techniques and proficiency would also be valuable. Data from throws for a greater variety of players and distances, with different trajectories and throwing techniques, are needed to determine optimal long-toss throwing distances for college pitchers. The current study used only healthy pitchers, even though flat-ground longtoss is relevant for injury rehabilitation. As stated above, players in rehabilitation throwing programs are instructed to use proper throwing mechanics, and the current study provides proper throwing data based upon a sample of healthy college pitchers. Future studies of player rehabilitation would be helpful to determine whether certain injuries lead to mechanical compensations and adjustments in throwing mechanics. The current study included baseball players from only 1 level (college) and 1 position (pitcher), which was also a limitation. To enhance our understand- research report ] ing of throwing biomechanics, data are needed for baseball players from a range of levels, various positions, and more distances. Skeletally immature throwers may require specific consideration due to poor mechanics and open growth plates. On the other end of the spectrum, professional players may require specific consideration due to their strength, length of season, and abilities to generate ball velocity, ball distance, and joint torque. Both clinical and longitudinal studies would prove valuable. Clinical studies could be designed to compare baseball success of groups of athletes after various long-toss programs. Longitudinal studies could measure throwing biomechanics at various time intervals for players involved with various rehabilitation or training protocols. CONCLUSION B ased on the results of this study, a college baseball pitcher should not be expected to throw long, flat throws without kinematic and kinetic differences in his pitching biomechanics. As reported here, the increased kinetic and kinematic values with increased throw distance support our clinical experience that long-toss too early in rehabilitation may lead to shoulder and or elbow soreness. The use of long-toss in rehabilitation should be under the supervision of a clinician to monitor tissue healing and joint range of motion. It is the opinion of the authors that long-toss throwing on a line is a safe exercise for rehabilitation and training; however, the use of long-toss throwing for maximum distance may not be beneficial. This advice against maximum-distance throwing is based upon the high magnitudes of elbow varus torque, shoulder internal rotation torque, and upper trunk tilt, and low magnitude of forward trunk tilt. More biomechanical data are needed to quantify various long-toss throwing distances, techniques, and protocols for players of various ages, skill levels, and health levels. Performance and safety data after various long-toss throwing programs may be valuable in determining clinical efficacy. t KEY POINTS FINDINGS: In a comparison of 4 types of throws (pitching from a mound and 3 long-toss throws from flat ground), shoulder and elbow angles and torques increased as throwing distance increased. Differences in leg and trunk kinematics were also noticed. The greatest number of differences was found between maximum-distance throwing and pitching, 37-m throws, and 55-m throws. IMPLICATION: Because shoulder and elbow torques increase with throwing distance, progression of throwing during rehabilitation should be under the supervision of a physical therapist or other clinician, to monitor tissue healing and joint range of motion. While long-toss thrown on a line seems biomechanically sound for rehabilitation and training, the use of long-toss throws for maximum distance may be more harmful than beneficial. CAUTION: Data were collected solely from healthy, college-age pitchers. ACKNOWLEDGEMENTS: The authors express their gratitude to the coaches and players of the Samford University, Birmingham-Southern College, and University of Alabama at Birmingham baseball teams for their participation in this study. The authors also thank Ryosuke Ito and Andrew Chappell for their assistance in data processing and literature review. REFERENCES 1. A guinaldo AL, Buttermore J, Chambers H. Effects of upper trunk rotation on shoulder joint torque among baseball pitchers of various levels. J Appl Biomech. 2007;23:42-51. 2. Anz AW, Bushnell BD, Griffin LP, Noonan TJ, Torry MR, Hawkins RJ. Correlation of torque and elbow injury in professional baseball pitchers. Am J Sports Med. 38:1368-1374. http://dx.doi. org/10.1177/0363546510363402 3. Axe MJ, Snyder-Mackler L, Konin JG, Strube MJ. 302 | may 2011 | volume 41 | number 5 | journal of orthopaedic & sports physical therapy 41-05 Fleisig.indd 302 4/20/2011 2:15:27 PM 4. 5. 6. 7. 8. 9. 10. 11. 12. Development of a distance-based interval throwing program for Little League-aged athletes. Am J Sports Med. 1996;24:594-602. Burkhart SS, Morgan CD. The peel-back mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy. 1998;14:637-640. Chu Y, Fleisig GS, Simpson KJ, Andrews JR. Biomechanical comparison between elite female and male baseball pitchers. J Appl Biomech. 2009;25:22-31. Dun S, Fleisig GS, Loftice J, Kingsley D, Andrews JR. The relationship between age and baseball pitching kinematics in professional baseball pitchers. J Biomech. 2007;40:265-270. http:// dx.doi.org/10.1016/j.jbiomech.2006.01.008 Dun S, Kingsley D, Fleisig GS, Loftice J, Andrews JR. Biomechanical comparison of the fastball from wind-up and the fastball from stretch in professional baseball pitchers. Am J Sports Med. 2008;36:137-141. http://dx.doi. org/10.1177/0363546507308938 Dun S, Loftice J, Fleisig GS, Kingsley D, Andrews JR. A biomechanical comparison of youth baseball pitches: is the curveball potentially harmful? Am J Sports Med. 2008;36:686-692. http:// dx.doi.org/10.1177/0363546507310074 Escamilla R, Fleisig G, Barrentine S, Andrews J, Moorman C, 3rd. Kinematic and kinetic comparisons between American and Korean professional baseball pitchers. Sports Biomech. 2002;1:213-228. Escamilla R, Fleisig G, Barrentine S, Zheng N, Andrews J. Kinematic comparisons of throwing different types of baseball pitches. J Appl Biomech. 1998;14:1-23. Escamilla RF, Barrentine SW, Fleisig GS, et al. Pitching biomechanics as a pitcher approaches muscular fatigue during a simulated baseball game. Am J Sports Med. 2007;35:23-33. http:// dx.doi.org/10.1177/0363546506293025 Fleisig G, Chu Y, Weber A, Andrews J. Variability in baseball pitching biomechanics among 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. various levels of competition. Sports Biomech. 2009;8:10-21. Fleisig G, Escamilla R, Andrews J, Matsuo T, Satterwhite Y, Barrentine S. Kinematic and kinetic comparison between baseball pitching and football passing. J Appl Biomech. 1996;12:207-224. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239. Fleisig GS, Barrentine SW, Escamilla RF, Andrews JR. Biomechanics of overhand throwing with implications for injuries. Sports Med. 1996;21:421-437. Fleisig GS, Barrentine SW, Zheng N, Escamilla RF, Andrews JR. Kinematic and kinetic comparison of baseball pitching among various levels of development. J Biomech. 1999;32:1371-1375. Fleisig GS, Kingsley DS, Loftice JW, et al. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am J Sports Med. 2006;34:423-430. http://dx.doi.org/10.1177/0363546505280431 Fortenbaugh D, Fleisig G, Andrews J. Baseball pitching biomechanics in relation to injury risk and performance. Sports Health: A Multidisciplinary Approach. 2009;1:314-320. Matsuo T, Escamilla R, Fleisig G, Barrentine S, Andrews J. Comparison of kinematic and temporal parameters between different pitch velocity groups. J Appl Biomech. 2001;17:1-13. Miyanishi T, Fujii N, Ae M, Kunugi Y, Okada M. A three-dimensional comparative study of the motions between speed throw and distance throw in the university baseball players. Japan J Physical Ed. 1995;40:89-103. Nissen CW, Westwell M, Ounpuu S, et al. Adolescent baseball pitching technique: a detailed three-dimensional biomechanical analysis. Med Sci Sports Exerc. 2007;39:1347-1357. http:// dx.doi.org/10.1249/mss.0b013e318064c88e Reinold MM, Wilk KE, Reed J, Crenshaw K, Andrews JR. Interval sport programs: guidelines for baseball, tennis, and golf. J Orthop Sports Phys Ther. 2002;32:293-298. 23. S abick MB, Torry MR, Lawton RL, Hawkins RJ. Valgus torque in youth baseball pitchers: a biomechanical study. J Shoulder Elbow Surg. 2004;13:349-355. http://dx.doi.org/10.1016/ S1058274604000308 24. Shepard MF, Dugas JR, Zeng N, Andrews JR. Differences in the ultimate strength of the biceps anchor and the generation of type II superior labral anterior posterior lesions in a cadaveric model. Am J Sports Med. 2004;32:1197-1201. http://dx.doi.org/10.1177/0363546503262643 25. Stodden DF, Fleisig GS, McLean SP, Andrews JR. Relationship of biomechanical factors to baseball pitching velocity: within-pitcher variation. J Appl Biomech. 2005;21:44-56. 26. Werner SL, Guido JA, Jr., Stewart GW, McNeice RP, VanDyke T, Jones DG. Relationships between throwing mechanics and shoulder distraction in collegiate baseball pitchers. J Shoulder Elbow Surg. 2007;16:37-42. http://dx.doi.org/10.1016/j. jse.2006.05.007 27. Whiteley R. Baseball throwing mechanics as they relate to pathology and performance: a review. J Sports Sci Med. 2007;6:1-20. 28. Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30:136-151. 29. Wilk KE, Obma P, Simpson CD, Cain EL, Dugas JR, Andrews JR. Shoulder injuries in the overhead athlete. J Orthop Sports Phys Ther. 2009;39:38-54. http://dx.doi.org/10.2519/ jospt.2009.2929 30. Zheng N, Fleisig G, Andrews J. Biomechanics and injuries of the shoulder during throwing. Athl Therapy Today. 1999;4:6-10. @ MORE INFORMATION WWW.JOSPT.ORG VIEW Videos on JOSPT’s Website Videos posted with select articles on the Journal’s website (www.jospt.org) show how conditions are diagnosed and interventions performed. For a list of available videos, click on “COLLECTIONS” in the navigation bar in the left-hand column of the home page, select “Media”, check “Video”, and click “Browse”. A list of articles with videos will be displayed. journal of orthopaedic & sports physical therapy | volume 41 | number 5 | may 2011 | 303 41-05 Fleisig.indd 303 4/20/2011 2:15:28 PM