Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
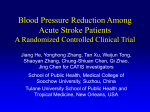
Antihypertensive Medications Prescribed at Discharge After an Acute Ischemic Cerebrovascular Event Bruce Ovbiagele, MD; Nancy K. Hills, PhD, MBA; Jeffrey L. Saver, MD; S. Claiborne Johnston, MD, PhD; for the CASPR Investigators Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Background and Purpose—Hypertension is poorly controlled in stroke survivors, thereby placing them at increased risk for recurrent events. Clinical trial evidence suggests that antihypertensive treatment may be beneficial for stroke prevention in hypertensive and normotensive stroke patients. We aimed to evaluate the discharge antihypertensive prescription patterns in patients hospitalized for an ischemic cerebrovascular event and to determine factors associated with treatment utilization. Methods—We analyzed patients diagnosed with ischemic stroke or transient ischemic attack (TIA) in the California Acute Stroke Prototype Registry (CASPR). We used generalized estimating equations to identify factors independently associated with receiving antihypertensives at the time of hospital discharge. Results—Data were collected on 764 consecutive patients with ischemic stroke or TIA encountered at 11 hospitals representative of facilities in the state of California. Overall, the rate of discharge with a prescription for any antihypertensive in the CASPR cohort was 69.4%. Hospital-specific rates were heterogeneous (P⫽0.04), varying from 55% to 100%. In multivariate analysis, independent predictors of prescription for antihypertensive medication at discharge were a history of hypertension (P⬍0.0001), diabetes (P⫽0.0009), and older age. Conclusions—About two-thirds of patients hospitalized with acute ischemic cerebrovascular events are discharged from the hospital on ⱖ1 antihypertensive medication. However, there is great variability in prescription rates between hospitals and considerable room for improvement. (Stroke. 2005;36:1944-1947.) Key Words: hypertension 䡲 secondary prevention 䡲 stroke H ypertension is a potent yet modifiable risk factor for recurrent stroke,1 and the use of antihypertensive treatment has been shown to reduce this risk substantially.2– 4 Nonetheless, blood pressure is poorly controlled among individuals who have experienced a previous stroke.5 Indeed, with recent community-based data revealing a high early risk of secondary stroke6,7 and evidence indicating the presence of hypertension at the time of hospital discharge as a predictor of such risk,8 there is a need to improve antihypertensive treatment rates in stroke survivors, including those who are normotensive.4 A potential bridge for the antihypertensive knowledge– treatment divide could be the systematic and appropriate prescription of antihypertensives before the patient leaves the hospital or after admission for an acute ischemic stroke or transient ischemic attack (TIA).9 This strategy is attractive because it can be safe,10 studies suggest that in-hospital behavior strongly influences postdischarge community practice,11 and moderate reductions in blood pressure during the first week after hospital admission have been associated with improved short-term functional outcome in patients with acute ischemic stroke.12 However, no previous study has analyzed the frequency and patterns of discharge prescription for antihypertensives in patients with ischemic stroke or TIA. In a cohort study derived from representative Californian hospitals, we evaluated the frequency and patterns of discharge antihypertensive utilization in a large, multicenter cohort of hospitalized stroke and TIA patients and assessed the impact of recent national hypertensive guidelines and clinical trial evidence on discharge prescription behavior. Patients and Methods Data from the California Acute Stroke Prototype Registry (CASPR) were analyzed. CASPR collected data prospectively on acute stroke care in individuals with a diagnosis of suspected stroke or TIA in 11 hospitals in 5 major population regions of California from November 1, 2002, through January 31, 2003, and from November 1, 2003, through January 31, 2004. The CASPR study methods have been described previously.13 Human subject review boards at each participating center approved CASPR. For these analyses, we included all patients with a discharge diagnosis of ischemic stroke or TIA who were admitted during either time period. We first examined rates of antihypertensive use among hospitals to determine whether intrahospital variability existed at a Received April 16, 2005; accepted May 30, 2005. From the Stroke Center and Department of Neurology (B.O., J.L.S.), UCLA Medical Center, Los Angeles, Calif; Department of Neurology (B.O., J.L.S.), Olive View—UCLA Medical Center, Los Angeles, Calif; and Department of Neurology (N.K.H., S.C.J.), University of California, San Francisco. Correspondence to Bruce Ovbiagele, MD, Stroke Center and Department of Neurology, University of California at Los Angeles, 710 Westwood Plaza, Los Angeles, CA 90095. E-mail [email protected] © 2005 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000177522.80092.b7 1944 Ovbiagele et al Antihypertensive Prescription After Ischemic Stroke significant level. We identified the rates of use of different classes of medication categorizing antihypertensives into the following groups: angiotensin-converting enzyme inhibitors (ACEIs), -adrenergic blocking agents, calcium channel blockers, angiotensin receptor blockers, diuretics, and “other” antihypertensives, including centrally acting adrenergics, peripherally acting antiadrenergics, and vasodilators. We then examined characteristics potentially associated with receipt of any antihypertensive medication at discharge in the overall cohort. Because this analysis could potentially reflect risk factors for hypertension as well as predictors of treatment with antihypertensive medications, we also analyzed patients with and without a history of hypertension separately. Statistical Analysis Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 The 2 test for homogeneity was used to evaluate whether or not the hospitals were homogeneous with respect to the proportion of patients treated with antihypertensive medications. Because a significant difference in treatment rates was observed, generalized estimating equations were used for univariate and multivariate analyses to account for within-hospital and between-hospital variances. Variables significant at the ␣⫽0.05 level in univariate analysis were included in multivariate analysis. SAS (version 8e; SAS Institute) was used for all statistical analysis. Results Overall, 764 patients were diagnosed with either ischemic stroke or TIA at the 11 CASPR hospitals. Subjects in the overall cohort were 53.4% women, 55.4% white, 9.9% black, with an average age of 70.4 (⫾15.4) years. Among these, 530 patients (69.4%) received a discharge prescription for any antihypertensive. However, rates among hospitals were heterogeneous (P⫽0.04), ranging from a low of 55% to a high of 100%. Across the entire cohort, 17 (2.2%) were discharged on ⱖ4 antihypertensive agents, 60 (7.9%) on 3, 177 (23.2%) on 2, and 276 (36.1%) on 1. Factors associated in univariate analysis with receipt of antihypertensives at discharge included older age, diagnosis of ischemic stroke (versus TIA), history of coronary artery disease, history of congestive heart failure, history of hypertension, history of diabetes, and history of atrial fibrillation (Table). Patients who received tissue plasminogen activator who were ambulatory at discharge or who were discharged home were less likely to receive antihypertensives (Table). In multivariate analysis, history of hypertension, history of diabetes, and older age (those who were 73 years of age compared with those who were ⱕ60 years of age) remained significantly associated with receiving antihypertensives at discharge (Table). In separate analyses of patients without a history of hypertension (n⫽242), 39% received antihypertensive medication at discharge. Older age and a history of atrial fibrillation were significantly associated with higher rates of antihypertensive usage at discharge among those with no previous history of hypertension, whereas those patients with independent ambulation were less likely to receive treatment. Patients with a documented history of hypertension were more likely to receive antihypertensives at discharge if they had a history of dyslipidemia or diabetes (multivariate analysis; results not shown). ACEIs were the most prescribed class of antihypertensives in 303 patients (39.7% of the cohort), as seen in the Figure. Among the 254 patients in the entire cohort taking 2 or more antihypertensives, the most common combination regimen 1945 was ACEI and a -blocker, which was used in 59 patients (23%). Discussion This study shows that at representative hospitals in California, a substantial majority of individuals discharged from the hospital after an ischemic stroke or TIA are prescribed ⱖ1 antihypertensive agents, but 1 of every 3 patients is discharged on no antihypertensive therapy. Strengths of our study are the inclusion of multiple hospitals in different healthcare settings and the examination of characteristics associated with receipt of antihypertensive treatment at discharge. We found that older individuals and those with a history of hypertension or diabetes were more likely to receive a prescription for an antihypertensive at the time of hospital discharge. At first glance, the fact that a majority of hospitalized ischemic stroke and TIA patients are discharged on ⱖ1 antihypertensive drug may seem encouraging. However, the evidence that large numbers of stroke survivors with hypertension remain poorly controlled5,14 suggests there is either ineffective implementation or suboptimal long-term maintenance of these therapies. Studies have shown that strategies such as low-dose combination therapy, for instance, increase antihypertensive treatment efficacy and reduce adverse effects, and current national guidelines specifically call for combination therapy in stroke survivors.15–17 However, only 33.2% of patients in our study were discharged on combination antihypertensive regimens. It should also be noted that in our study, a history of a previous stroke or TIA was not independently associated with antihypertensive prescription. This is despite current guidelines16 and a large secondary stroke prevention trial,4 indicating the benefit of antihypertensive treatment for secondary stroke prevention among those with relatively normal blood pressures. Such omission after ⱖ2 cerebrovascular events is cause for concern because it is inappropriate to assume that therapy will be initiated in a timely fashion, if at all, after hospitalization for a vascular event.11 Another finding from our study, was that although national guidelines recommend that thiazide-type diuretics be used in drug treatment for most hypertensive patients either alone or combined with drugs from other classes,16 we found a lower prescription of these medications compared with ACEIs and -blockers among our patients. A wide variation in discharge antihypertensive treatment rates existed among CASPR hospitals. This is perhaps not surprising given the paucity of data and guidelines pertaining to the appropriate timing for systematic, safe, and appropriate antihypertensive drug initiation after an ischemic stroke or TIA. Supporting an early rather than delayed approach to antihypertensive agent initiation, a recent study showed that systematic in-hospital initiation of antihypertensives before hospital discharge after an ischemic stroke or TIA was associated with high treatment adherence rates 3 months after hospitalization.18 The results of the ACCESS trial, in which improved outcomes were observed in patients receiving an antihypertensive agent early after stroke onset, lends further credence to the potential safety and effectiveness of this strategy.10 The first few weeks and months after initial TIA or 1946 Stroke September 2005 Discharge Prescription of Antihypertensive Medication After Ischemic Stroke/TIA Hospitalization Antihypertensive at Discharge (n⫽522) Characteristics n No (%) Univariate† OR (95% CI) P Value Adjusted† OR (95% CI) P Value Age in quartiles ⬍60 years 183 102 (55.7) Reference 60–73 years 180 128 (71.1) 2.17 (1.25, 3.77) ⬍0.006 1.50 (0.85, 2.61) 0.16 73–82 years 188 144 (76.6) 2.98 (2.13, 4.16) ⬍0.0001 2.08 (1.54, 2.83) ⬍0.0001 ⬎82 years 213 156 (73.2) 2.45 (1.72, 3.48) ⬍0.0001 1.46 (1.06, 2.01) 0.02 Female 408 290 (71.1) Reference Male 356 240 (67.4) 0.83 (0.62, 1.09) Reference Gender 0.18 Ethnicity Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Black 76 54 (71.1) Reference Other 688 476 (69.2) 1.09 (0.58, 2.04) TIA 172 108 (63) Reference Ischemic stroke 592 422 (71) 1.45 (1.05, 2.00) Year 1 516 355 (68.8) Reference Year 2 248 175 (70.6) 1.16 (0.70, 1.92) 0.57 Hypertension 516 431 (83.5) 8.03 (6.08, 10.6) ⬍0.0001 Stroke/TIA 277 203 (73.3) 1.36 (0.97, 1.90) 0.07 Myocardial infarction or coronary artery disease 160 126 (78.8) 1.84 (1.31, 2.57) 0.0004 0.79 Event type Reference 0.02 1.25 (0.74, 2.11) 0.39 7.25 (5.16, 10.2) ⬍0.0001 Treatment year History of* Heart failure 1.35 (0.85, 2.14) 0.2 83 67 (80.7) 2.00 (1.24, 3.23) 0.005 1.13 (0.65, 1.97) 0.67 Diabetes 199 160 (80.4) 2.17 (1.70, 2.77) ⬍0.0001 1.58 (1.21, 2.07) 0.0009 Dyslipidemia 243 188 (77.4) 1.80 (1.40, 2.30) ⬍0.0001 1.11 (0.89, 1.38) 0.38 Atrial fibrillation 125 102 (81.6) 2.19 (1.30, 3.69) 0.003 2.10 (0.97, 4.56) 0.06 No 748 523 (69.9) Yes 16 7 (43.8) 0.35 (0.17, 0.72) 0.005 0.36 (0.11, 1.17) 0.09 Ambulation status** 400 257 (64.3) 0.60 (0.50, 0.71) ⬍0.0001 0.80 (0.50, 1.29) 0.36 Discharged home 501 333 (66.5) 0.67 (0.50, 0.91) 0.009 1.04 (0.58, 1.88) 0.89 Received tissue plasminogen activator Reference Reference †All analyses performed using generalized estimating equations; *reference category consists of all patients without a history of the given characteristic; **at discharge. ischemic stroke is the period of highest risk for recurrence,6 making early implementation of optimal secondary prevention therapies highly desirable. Interestingly, we observed that a substantial proportion of individuals with no history of hypertension were discharged on antihypertensive agents. However, this finding may reflect the influence of clinical trial results that suggest stroke survivors with normal blood pressures may reap benefit from antihypertensive treatment,5 or these agents may have been prescribed for other therapeutic reasons such as -blocker use for cardiac rate control or ACEIs for heart failure. Although we collected data on history of hypertension among CASPR subjects, we did not collect data on the premorbid use of antihypertensive agents. We are also limited by a paucity of information on the potential contraindications or adverse reactions that might have prevented the use of certain antihypertensive medications. CASPR investigators also did not collect information on stroke/TIA mechanisms, which could have influenced the decision to initiate antihypertensive therapies, particularly in patients with nonatherosclerotic mechanisms such as hypercoagulable states, vasculitis, etc, for their event. Finally, we have no information on actual blood pressure measurements during hospitalization; and although these may have impacted treatment decisions, it has been shown that blood pressures in the majority of acute stroke patients may not return fully to baseline levels for several days to weeks after the index event,19 and so stroke hospitalization blood pressures may not be the best parameter by which to judge the treatment needs of an individual stroke patient. Furthermore, the approach of using blood pressure measurement as the sole determinant in the decision whether to initiate antihypertensives for the majority of ischemic Ovbiagele et al Antihypertensive Prescription After Ischemic Stroke Percentage of total patients with ischemic stroke or TIA who were treated with each specific class of antihypertensive medication at discharge. Percentages for each group do not total to 100% because some patients received ⬎1 antihypertensive medication. Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 stroke/TIA patients may not be as relevant as thought previously because the key to the efficacy of antihypertensive treatment in stroke prevention may lie in blood pressure reduction4 and perhaps additional mechanisms,20 –22 not just treatment of diagnosed hypertension. Acknowledgments This study was supported by the Centers for Disease Control (U50 CCU920271). References 1. Wolf P, Clagett GP, Easton JD, Goldstein LB, Gorelick PB, Kelly-Hayes M, Sacco RL, Whisnant JP. Preventing ischemic stroke in patients with prior stroke and transient ischemic attack: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke. 1999;30:1991–1994. 2. Gueyffier F, Boissel JP, Boutitie F, Pocock S, Coope J, Cutler J, Ekbom T, Fagard R, Friedman L, Kerlikowske K, Perry M, Prineas R, Schron E. Effect of antihypertensive treatment in patients having already suffered from stroke. Gathering the evidence. The INDANA (INdividual Data ANalysis of Antihypertensive intervention trials) Project Collaborators. Stroke. 1997;28:2557–2562. 3. PATS Collaborating Group. Post-stroke antihypertensive treatment study. A preliminary result. Chin Med J (Engl). 1995;108:710 –717. 4. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358:1033–1041. 5. Qureshi A, Suri MF, Guterman LR, Hopkins LN. Ineffective secondary prevention in survivors of cardiovascular events in the US population: report from the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2001;161:1621–1628. 1947 6. Coull A, Lovett JK, Rothwell PM. Population-based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organisation of services. BMJ. 2004;328:326. 7. Johnston S, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. J Am Med Assoc. 2000;284: 2901–2906. 8. Hankey G. Long-term outcome after ischaemic stroke/transient ischemic attack. Cerebrovasc Dis. 2003;16:14 –19. 9. Ovbiagele B, Saver JL, Fredieu A, Suzuki S, McNair N, Dandekar A, Razinia T, Kidwell CS. PROTECT: a coordinated stroke treatment program to prevent recurrent thromboembolic events. Neurology. 2004; 63:1217–1222. 10. Schrader J, Luders S, Kulschewski A, Berger J, Zidek W, Treib J, Einhaupl K, Diener HC, Dominiak P. The ACCESS Study: evaluation of Acute Candesartan Cilexetil Therapy in Stroke Survivors. Stroke. 2003; 34:1699 –1703. 11. Fonarow G. The role of in-hospital initiation of cardiovascular protective therapies to improve treatment rates and clinical outcomes. Rev Cardiovasc Med. 2003;4:S37–S46. 12. Rodriguez-Garcia J, Botia E, de La Sierra A, Villanueva MA, GonzalezSpinola J. Significance of elevated blood pressure and its management on the short-term outcome of patients with acute ischemic stroke. Am J Hypertens. 2005;18:379 –384. 13. California Acute Stroke Pilot Registry (CASPR) Investigators. Prioritizing interventions to improve rates of thrombolysis for ischemic stroke. Neurology. 2005;64:654 – 659. 14. Hillen T, Dundas R, Lawrence E, Stewart JA, Rudd AG, Wolfe CD. Antithrombotic and antihypertensive management 3 months after ischemic stroke: a prospective study in an inner city population. Stroke. 2000;31:469 – 475. 15. Law M, Wald NJ, Morris JK, Jordan RE. Value of low-dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326:1427. 16. Chobanian A, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. J Am Med Assoc. 2003;289:2560 –2572. 17. Khan N, McAlister FA, Campbell NR, Feldman RD, Rabkin S, Mahon J, Lewanczuk R, Zarnke KB, Hemmelgarn B, Lebel M, Levine M, Herbert C. The 2004 Canadian recommendations for the management of hypertension: Part II—therapy. Can J Cardiol. 2004;20:41–54. 18. Ovbiagele B, Saver JL, Fredieu A, Suzuki S, Selco S, Rajajee V, McNair N, Razinia T, Kidwell CS. In-hospital initiation of secondary stroke prevention therapies yields high rates of adherence at follow-up. Stroke. 2004;35:2879 –2883. 19. Carlberg B, Asplund K, Hagg E. The prognostic value of admission blood pressure in patients with acute stroke. Stroke. 1993;24:1372–1375. 20. Ruland S, Gorelick PB. Are cholesterol-lowering medications and antihypertensive agents preventing stroke in ways other than by controlling the risk factor? Curr Neurol Neurosci Rep. 2003;3:21–26. 21. Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995–1003. 22. Schrader J. Blood pressure control and beyond: secondary prevention of stroke with eprosartan (MOSES Study), in XXVI European Society of Cardiology Congress, 2004: Munich, Germany. Antihypertensive Medications Prescribed at Discharge After an Acute Ischemic Cerebrovascular Event Bruce Ovbiagele, Nancy K. Hills, Jeffrey L. Saver and S. Claiborne Johnston Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Stroke. 2005;36:1944-1947; originally published online July 28, 2005; doi: 10.1161/01.STR.0000177522.80092.b7 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/36/9/1944 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/