Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
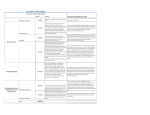
WHO Recommendations for the Prevention of Postpartum Haemorrhage Results from a WHO Technical Consultation – October 18-20, 2006 Deborah Armbruster, POPPHI/PATH White Ribbon Alliance/ Core Group/ POPPHI September 25, 2007 Summary of Recommendations • Active management of the third stage of labor should be offered by skilled attendants to all women. • In the context of AMTSL: Skilled attendants should offer oxytocin in preference to ergometrine, methylergometrine, Syntometrine, misoprostol, Carboprost. • In the absence of AMTSL, a uterotonic drug (oxytocin or misoprostol) should be offered by a health worker trained in its use for prevention of PPH. • Because of the benefits to the baby, the cord should not be clamped earlier than is necessary for applying controlled cord traction in AMTSL. • For the sake of clarity, it is estimated that this will normally take around 3 minutes Background While there is general agreement on the beneficial effects of AMTSL, there are several unresolved issues: • Clear definitions of components • AMTSL under conditions of limited resources: Timing of uterotonic Drug to use Route of administration Can non-skilled providers use controlled cord traction? Background • Is early clamping of cord necessary? • What does ‘early’ mean? • Suggestions to provide misoprostol where oxytocin not available to non-skilled providers and women themselves • Concerns that misuse of misoprostol can lead to significant maternal morbidity and even death Rationale for WHO Technical Consultation In light of these issues, WHO held a Technical Consultation on PPH in Geneva on 18-20 October 2006 to: • Discuss various issues related to prevention of PPH • Develop recommendations Methods • Questions drafted by WHO staff (MPS, RH, Medicines, Policies and Standards) on various intervention described for prevention of atonic PPH (AMTSL and its components) • Each question was subdivided to address “skilled” or “non-skilled” provider • These questions and proposed outcomes to consider were sent to international panel of experts (58 experts in 6 WHO regions – 37 responses received) Methods • Helped define “critical outcomes” vs. “important but not critical” • Responses were reviewed by WHO core team • External organization commissioned to review and grade the evidence to answer the questions, using the GRADE methodology Methods • Evidence-based recommendations in response to the questions asked were drafted • Draft methodology, results, and recommendations were sent to sub-group of experts prior to their participation in the WHO Technical Consultation on PPH • This draft and supporting evidence were reviewed at the Technical Consultation and changes made based on the recommendations of the expert panel. Grades of Recommendation Assessment, Development and Evaluation 1. Assess the quality of evidence, prepare evidence profiles 2. Choose questions and rate importance of outcomes for decision making (before considering the evidence) 3. Assess the overall risk-benefit ratio, considering cost, access, and feasibility Categories of quality • High: Further research is very unlikely to change our confidence in the estimate of effect. ++++ • Moderate: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. +++ • Low: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. ++ • Very low: Any estimate of effect is very uncertain. + Judgements about the balance between benefits and harms • Strong recommendation: the panel is confident that the desirable effects of adherence to a recommendation outweigh the undesirable effects. • Weak recommendation: the panel concludes that the desirable effects of adherence to a recommendation probably outweigh the undesirable effects, but is not confident. Critical beneficial outcomes Fewer maternal deaths 8.5 Fewer admissions to intensive care unit 6.4 Less blood loss > 500 mL 6.3 Less blood loss > 1000 mL 7.7 Less need for blood transfusion 7.8 What are the most important beneficial or “priority” outcomes of interventions to prevent PPH? • Reduction in maternal mortality • Less blood loss > 1000 ml Less need for additional uterotonics 5.9 Decreased mean blood loss 5.6 Less postpartum anaemia 6.1 Earlier establishmend of breast feeding 5.1 Less anaemia in infancy 4.8 • Less use of blood transfusion • Less use of uterotonics (added by the expert panel) Evidence and Recommendations 1. Should AMTSL be offered by skilled attendants to all women 1 systematic review 5 trials UK, Ireland, UAE Different combinations of the components Recommendation: • AMTSL should be offered by skilled attendants to all women • Recommendation: STRONG • Quality of evidence: MODERATE • The panel does not recommend AMTSL by non-skilled attendants Remarks: Although no evidence was found for or against the use of AMTSL by non-skilled providers, the group placed high value on the potential risks – such as uterine inversion – that may result from inappropriate cord traction. 2. Should oxytocin (10 IU parenterally) or ergometrine/methylergometrine (0.25 mg parenterally) be offered in AMTSL? 2 systematic reviews > 9,000 women Oxytocin vs. ergometrine vs. syntometrine Oxytocin dose (2-10 IU), IM/IV Only one trial with direct comparison (1049 women) Recommendation: • Oxytocin 10 IU IM should be offered to all women in preference to ergometrine • If oxytocin is not available ergo/methylergo or syntometrine should be offered to women without hypertension and heart disease • Recommendation: STRONG • Quality of evidence: LOW Remarks: The recommendation places a high value on avoiding the adverse effects of ergometrine, and assumes similar benefit for oxytocin and ergometrine. 3. Should oral misoprostol (600 mcg) be offered instead of oxytocin (10 IU IM) in AMTSL? One systematic review 7 trials with direct comparison Largest trial > 18,000 women Recommendation: • In the context of AMTSL skilled attendants should offer oxytocin in preference to oral misoprostol (600 mcg). • Recommendation: STRONG • Quality of evidence: HIGH Remarks: This recommendation places a high value on the relative benefits of oxytocin in preventing blood loss compared to misoprostol, as well as the increased adverse effects of misoprostol compared to oxytocin 4. Should sublingual misoprostol (600 mcg) be offered instead of oxytocin (10 IU IM)? One systematic review 2 trials < 200 women 1 trial compared to syntometrine Recommendation: • In the context of AMTSL skilled attendants should not offer sublingual misoprostol for prevention of PPH in preference to oxytocin • Recommendation: STRONG • Quality of evidence: VERY LOW Remarks: Further research is needed to define the role of sublingual misoprostol administration for prevention of PPH 5. Should rectal misoprostol (600 mcg) be offered instead of oxytocin (10 IU IM)? Two systematic reviews Two oxytocin trials (one with 5 IU the other 10IU, 1221 women in total) One misoprostol trial (1620 women, auxiliary nurse-midwives) Recommendation: • In the context of AMTSL skilled attendants should not offer rectal misoprostol for prevention of PPH in preference to oxytocin • Recommendation: STRONG • Quality of evidence: LOW Remarks: This recommendation places a high value on the known benefits of oxytocin and notes the significant uncertainty about whether rectal misoprostol is equivalent. Misoprostol has more adverse effects and a higher purchase cost. 6. Should carboprost 0.25 mg/sulprostone 0.5 mg) be offered instead of oxytocin (10 IU IM)? One systematic review Eight trials comparing injectable prostaglandins with other injectable uterotonics No study has compared carboprost/sulprostone with 10 IU oxytocin IM Recommendation: • In the context of AMTSL skilled attendants should not offer carboprost/sulprostone in preference of oxytocin • Recommendation: STRONG • Quality of evidence: VERY LOW Remarks: This recommendation is based on the paucity of evidence comparing the two treatments and the known effectiveness of oxytocin. 7. In the absence of AMTSL, should uterotonics be used alone for prevention of PPH? Two systematic reviews Two oxytocin trials (one with 5 IU the other 10IU, 1221 women in total) One misoprostol trial (1620 women, auxiliary nurse-midwives) Recommendation: • In the absence of AMTSL, a uterotonic drug (oxytocin or misoprostol) should be offered by a health worker trained in its use for prevention of PPH • Recommendation: STRONG • Quality of evidence: MODERATE Remarks: For misoprostol, this recommendation places a high value on the potential benefits of avoiding PPH and ease of administration of an oral drug in settings where other care is not available, but notes there is only one study. The only trial relevant to this recommendation used 600 mcg of misoprostol. The efficacy of lower doses has not been evaluated. There is still uncertainty about the lowest effective dose and optimal route of administration. 8. When should the cord be clamped to maximize benefits for mother and baby? One systematic review three additional trials varying definitions of early clamping (10 sec – 1 min) and delayed (2 min – stopping pulsation) no priority outcomes reported, but newborn anemia as an important outcome unclear whether timing of cord clamping has an effect on PPH Recommendation: • Because of the benefits to the baby, the cord should not be clamped earlier than necessary for applying cord traction in AMTSL. • Recommendation: WEAK • Quality of Evidence: LOW For the sake of clarity, it is estimated that this will normally take around 3 minutes Early clamping may be required if the baby is asphyxiated and requires immediate resuscitation. 9. Should the placenta be delivered by controlled traction in all women? Recommendation: • Given the current evidence for AMTSL includes cord traction, the panel does not recommend any change in the current practice. Further research is needed. • Recommendation: STRONG • Quality of evidence: VERY LOW Key discussion points Who is a skilled attendant? • Discussed extensively in context of components of AMTSL • Combines WHO, FIGO, ICM definition of 2004 with earlier definition by WHO, UNFPA, UNICEF and World Bank • Older definition is broader and considers variable conditions on many low and middle-income developing countries • Can include auxiliary nursemidwives, community midwives, village midwives and health visitors who have acquired appropriate skills, if specially trained Key discussion points Implementation of recommendations • Support from international professional organizations and partner agencies for changes in policy and regulation • Work through regional and country offices (WHO and partners) • Press release and co-publication • Misoprostol in EDL for PPH indications • Translation of recommendations • Disseminaton and implementation of recommendations • Develop a feedback mechanism • Develop a “virtual PPH network” Research Priorities Not in priority order • What dose and route of administration of misoprostol are preferred for best riskbenefit ratio (in AMTSL and expectant management) • Can oxytocin be administered safely by unskilled attendants? • What is role of buccal and sublingual use of oxytocin? • What is the effect of uterotonics on breastfeeding Research Priorities • With AMTSL, should misoprostol be used in addition to oxytocin • What is the optimal time for cord clamping in the context of physiologic management and AMTSL? • What is the optimum time for oxytocin administration in AMTSL to optimize the timing of cord clamping? • What is the role of individual components of AMTSL? Summary of Recommendations • Active management of the third stage of labor should be offered by skilled attendants to all women. • In the context of AMTSL: Skilled attendants should offer oxytocin in preference to ergometrine, methylergometrine, Syntometrine, misoprostol, Carboprost. • In the absence of AMTSL, a uterotonic drug (oxytocin or misoprostol) should be offered by a health worker trained in its use for prevention of PPH. • Because of the benefits to the baby, the cord should not be clamped earlier than is necessary for applying controlled cord traction in AMTSL. • For the sake of clarity, it is estimated that this will normally take around 3 minutes Program Implications and Next Steps For you to define… but could be: • Educate policy-makers about the need to adopt and operationalize these new guidelines • Increase resources to fund AMTSL training or ensure that sufficient oxytocin is available for every women at birth. • Get misoprostol registered in-country and create protocols for its use • Document successes and communicate to the media and decision-makers