Survey
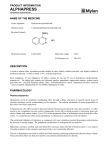
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al. vasodilator drugs on transcapillary fluid exchange in the renal cortex. Am J Physiol 230: 1148, 1976 29. Krakoff LR, Guia DD, Vlachakis N, Stricker J, Goldstein M: Effect of sodium balance on arterial blood pressure and renal responses to prostaglandin A, in man. Cire Res 33: 539, 1973 30. Merrill AJ: Mechanisms of salt and water retention in heart failure. Am J Med 6: 357, 1949 31. Earley LE, Schrier RW: Intrarenal control of sodium excretion by hemodynamic and physical factors. In Handbook of Physiology. Section 8: Renal Physiology, edited by Orloff T, Berlinger RW. Washington, DC, American Physiological 323 Society, 1973, pp 721-762 32. LeJemtel T, Hellman C, Elkayam U, Strom J, Blaufox MD, Frishman W, Ribner H, Sonnenblick E: Hemodynamic and renal response to oral hydralazine therapy in severe heart failure. Circulation 56 (suppl III): 111-9, 1977 33. Birch AA, Boyce WH: Changing renal blood flow following sodium nitroprusside in patients undergoing nephrolithotomy. Anesth Analg 56: 102, 1977 34. Pagani M, Vatner SF, Braunwald E: Hemodynamic effects of intravenous sodium nitroprusside in the conscious dog. Circulation 57: 144, 1978 Effect of Hydralazine on Renal Failure in Patients with Congestive Heart Failure Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 GORDON L. PIERPONT, M.D., PH.D., DAVID C. BROWN, M.D., JOSEPH A. FRANCIOSA, M.D., AND JAY N. COHN, M.D. SUMMARY Hydralazine is known to improve cardiac function in patients with congestive heart failure (CHF), but its effects on renal function in CHF are less clear. Sodium retention is known to occur with longterm use of hydralazine to treat hypertension; if this occurs in patients with CHF it could be deleterious. Therefore, in a metabolic unit we studied renal effects of hydralazine in patients with stable class III or IV CHF. In a single-blind study, the patients were given placebo twice daily for 3 days (period P-1), 100 mg of oral hydralazine twice daily for 3 days (period P-H), and placebo for 3 more days (period P-2). The average 24-hour creatinine clearance was 69.7 ± 7.7 ml/min (mean i SEM) in P-1, increased to 76.3 i 9.0 ml/min with hydralazine (p < 0.01) and fell again when hydralazine was stopped (P-2) to 68.5 i 7.8 ml/min (p < 0.02). Though the slight improvement in sodium excretion was not statistically significant (60.2 ± 12.1 mEq in P-1, 64.5 ± 12.4 mEq in P-H, 52.3 ± 7.7 mEq in P-2), serum osmolality decreased from 288 ± 1.8 mosM in P-1 to 283 ± 1.9 mosM in P-H (p < 0.02) and rose to 286 ± 1.9 mosM in P-2 (NS). During the three periods, serum sodium, chloride, potassium, carbon dioxide, blood urea nitrogen, creatinine and glucose were unchanged, as were weight and urine volume. Systolic blood pressure was 109.6 ± 3.6 mm Hg in P-1, 110.1 ± 3.9 mm Hg in P-H (NS), and 114.2 ± 5.0 mm Hg in P-2 (p < 0.05). Diastolic blood pressure, heart rate and respirations were unchanged. Thus, we found no evidence of sodium or water retention during hydralazine administration in patients with CHF, and renal function was actually improved, as evidenced by the increased creatinine clearance. HYDRALAZINE improves left ventricular performance in patients with congestive heart failure (CHF)' and may be effective for long-term oral therapy of patients with chronic CHF.1 2 However, hydralazine can lead to sodium and fluid retention when used to treat hypertension,3-5 and sodium retention has been reported during administration of hydralazine in a patient with CHF.6 Such a response to hydralazine in patients with CHF might limit the value of this drug for long-term therapy or necessitate larger doses of diuretics. The present study assesses the effects of hydralazine on renal function and sodium balance in patients with CHF. From the Department of Medicine, Cardiovascular and Renal Sections, University of Minnesota Hospitals, and Veterans Administration Medical Center, Minneapolis, Minnesota. Address for correspondence: Gordon L. Pierpont, M.D., Veterans Administration Medical Center, Cardiovascular Section, Minneapolis, Minnesota 55417. Received March 9, 1979; revision accepted August 20, 1979. Circulation 61, No. 2, 1980. Methods Nine male patients with New York Heart Association functional class III or IV heart failure (three class IV and six class III) who were on conventional therapy were studied. The patients were ages 47-64 years (average 59 years). Three of the patients had primary myocardial disease and six had ischemic heart disease. Exclusion criteria included: insulindependent diabetes mellitus, severe pulmonary disease (Po2 < 50 mm Hg or Pco2 > 50 mm Hg), renal insufficiency (BUN > 40 mg/dl or creatinine > 2.0 mg/dl), abnormal serum electrolytes, angina requiring nitrate therapy, myocardial infarction within the past 3 months, significant primary heart valve disease, hypertension requiring nondiuretic antihypertensive agents or heart failure due to restrictive heart disease. After giving written informed consent, the patients were admitted to a special diagnostic and treatment unit (SDTU) of the Minneapolis Veterans Administration Medical Center for evaluation. All patients were clinically stable with a steady body weight when admitted to the SDTU. All patients were 324 CIRCULATION VOL 61, No 2, FEBRUARY 1980 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 receiving a constant dose of diuretics, and eight of nine were taking digitalis at the time of admission. These medications, as well as any other medication the patient was taking regularly, were continued at a con- TABLE 1. Clinical Data from the Three Study Periods stant dose throughout the study period. One patient had been receiving isosorbide dinitrate, which was stopped more than 24 hours before entry into the study. On admission to the SDTU a dietary history was taken by a nutritionist and a diet constructed to match the usual sodium intake for each patient. Sodium and fluid intake were kept constant for the duration of the study and patients were allowed their normal level of activity. Supine blood pressure, heart rate, respirations and temperature were monitored four times daily, and the patients were weighed twice daily. The study protocol consisted of three periods of 3 days each. The first period consisted of 3 days of placebo administration (two tablets twice daily). This was followed by 3 days of active hydralazine therapy, 100 mg (two tablets twice daily) and another 3-day placebo period. The investigators, but not the patients, knew when hydralazine was being given. Each morning blood was drawn for determination of serum urea nitrogen, creatinine, glucose, sodium, chloride, total CO2, potassium and osmolality. In the last five patients studied, blood samples for plasma renin activity (PRA) were drawn on the third day of each period in the early morning with the patient supine. Urine was collected at 8-hour intervals throughout the study and analyzed for creatinine, potassium, sodium and osmolality. Creatinine clearances were calculated for each of the three daily 8-hour urine collections using the serum creatinine value obtained at the end of the day. All data were analyzed using the paired t test and differences were considered statistically significant for p values less than 0.05. The mean of all values obtained during each 3-day period were compared, and analysis of the data was repeated by averaging the values from the two placebo periods and comparing them with the values from the hydralazine period. Combining the placebo periods would tend to correct for trends during the course of hospitalization that might occur independent of hydralazine therapy. In order to examine the data for possible changes within each drug period, an additional analysis of the more pertinent variables was performed using an analysis of BP (mm Hg) HR (beats/min) variance. Results Table 1 shows the mean values during each period for mean arterial pressure (calculated as the diastolic pressure plus one-third of the pulse pressure), heart rate, body weight, serum creatinine, serum sodium, serum chloride, serum potassium and urine volume. None of these parameters changes significantly during hydralazine therapy when compared with each placebo period or with the average of the two placebo periods. In addition to the data presented in table 1, there P1 Study period H P2 84 -2.0 85 2.1 87 3.4 83 - 3.0 84 - 3.3 84 2.7 178 9.8 179- 9.8 177 10.1 Weight (lbs) Creat (mg/ml) 1.4 0.15 1.4- 0.18 1.4 0.16 BUN (mg/dl) 24 - 4.7 25 - 3.9 25 4.0 Na+ (mEq/l) 141 - 1.0 139 :1.5 140 1.6 Cl- (mEq/l) 100 1.4 99 1.9 99 1.9 K+ (mEq/l) 4.3 0.1 4.3 0.1 4.2 +0.1 Urine vol (1/24 hr) 2.1 0.26 2.2 0.27 2.1 i0.27 Values are average - SEM. None of the changes were statistically significant when compared from one period to another. Abbreviations: BP = mean blood pressure; HR = heart rate; Creat = creatinine; BUN = blood urea nitrogen; Na+ = serum sodium; Cl- = serum chloride; K+ = serum potassium; P1 = first placebo period; P2 = second placebo period; H = hydralazine. were no significant changes in respiratory rate, serum glucose, serum total CO2, creatinine excretion, sodium balance or combined sodium plus potassium excretion. Potassium excretion did not change from the first placebo period (102 ± 10.5 mEq/24 hours) to the drug period (103 ± 11.8 mEq/24 hours), but the decrease to 98 ± 11.1 mEq/24 hours in the second placebo period was statistically significant (p < 0.05) when compared with the active drug period. Because of this decrease during the second placebo period, potassium excretion was statistically higher (p < 0.05) during hydralazine therapy compared with the average of the two placebo periods. The effect of hydralazine on creatinine clearance, sodium excretion and serum osmolality are shown in figure 1. The average of all values during each period is shown for every patient, as well as the mean + SEM for the whole group. Creatinine clearance increased from an average of 69.7 i 7.7 ml/min during the first placebo period to 76.3 ± 9.0 ml/min during hydralazine therapy (p < 0.01). In no patient did creatinine clearance fall during administration of hydralazine. The creatinine clearance fell again during the second placebo period to 68.5 ± 7.8 ml/min, which was significantly lower than during hydralazine (p < 0.02). This value was not significantly different from the first placebo period. When compared with the average of the two placebo periods, the increase in creatinine clearance during hydralazine was significant (p < 0.01). Sodium excretion increased from 60.2 ± 12.1 mEq/ 24 hours during placebo to 64.5 ± 12.4 mEq/24 hours during hydralazine and decreased again to 52.3 ± 7.7 mEq/24 hours after hydralazine was stopped. These changes were not statistically significant when the hydralazine response was compared with each placebo period separately or with the pooled placebo periods. RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al. 125 1251 100t t 1001 325 295 E ' E NI E z z FIGURE 1. Individual values for creatinine clearance, sodium excretion and serum osmolality are shown for the first placebo period (PJ, for hydralazine administration (H), and for the second placebo period (P2). The solid lines connect the values for a given patient, the dotted line represents the mean for the group and the shaded area represents the standard error of the mean. E 290 CJ W 4 75 z 75 1 0 285 -J c) Z z W 50- 2 280 50- (n 4 0 25- C,)1 275 25270- P1 H P2 p1 H P2 Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Serum osmolality decreased during hydralazine in measured. 288 ± 2.6 mosM to 283 2.7 mosM during hydralazine (p < 0.02), and returned toward baseline during the second placebo period (286 + 2.7 mosM). The change in serum osmolality during hydralazine compared with the average of the two placebo periods was significant (p < 0.02). Although neither sodium excretion nor mean arterial blood pressure changed significantly during administration of hydralazine in these nine patients, it is of interest to examine the relationship of these two variables in individual patients. Figure 2 shows the changes in blood pressure and sodium excretion from the combined placebo periods to hydralazine administration for each patient. Sodium excretion was lower during hydralazine in only three of nine patients. A decrease in mean arterial blood pressure occurred during hydralazine in all three of these patients. The largest decrease in sodium excretion occurred in the patients who had the largest decrease in blood pressure. In the three patients whose mean arterial blood pressure increased, sodium excretion also increased. In no patient did the blood pressure increase and sodium excretion decrease, and three patients had an increase in sodium excretion despite a decrease in blood pressure. Creatinine clearance and serum osmolality were further analyzed using the analysis of variance for single-factor experiments with repeated measures on the same elements.7 This analysis also showed the increase in creatinine clearance during hydralazine to be significant (p < 0.01), as well as the decrease in serum osmolality (p < 0.005), with no differences between the first and second placebo periods. Examination of the data for changes within each period revealed no significant differences from day o day in any period for either creatinine clearance or serum osmolality. We conclude that the patients were indeed stable during the initial placebo periods, and that they returned to control levels and stayed unchanged during the second placebo period, with no evidence of prolonged seven of the eight patients in whom it was The mean serum osmolality dropped from P H P 1 ~~~2 effect after cessation of hydralazine. Also, because there was no significant change from day to day during hydralazine therapy, there is no evidence of tolerance or cumulative effect over the 3-day hydralazine period. PRA increased during hydralazine administration in all five patients in whom it was measured. The average PRA increased from 4.2 1.18 ng/ml/hr during the first placebo period to 8.5 2.05 ng/ml/hr during hydralazine (p < 0.02), and decreased slightly to 7.6 ± 3.13 ng/ml/hr during the second placebo period. Discussion Most studies of the renal effects of hydralazine were performed in hypertensive patients in the early 1950s. These studies were stimulated in part by Reubi's8 find- A * NaoEXCRETION (meq / 24 hrs) 0 0 0 -8 -6 -4 -2 8 MABP (m m Hg) A 0 0 -30 -40 FIGURE 2. The changes in sodium excretion (ANa+ excretion) and in the mean arterial blood pressure (AMABP) from the combined placebo periods to hydralazine administration are plotted for each of the nine patients. 326 CIRCULATION Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 ing of increased renal plasma flow with no change in glomerular filtration rate when six patients with hypertension and four normal subjects were given 10 mg of hydralazine subcutaneously. Similar results in patients with hypertension were subsequently reported by other investigators.9"'4 In other studies in hypertensive patients, the renal hemodynamic responses to hydralazine were more variable.'5-17 Falch et al.15 found no change in effective renal plasma flow in 11 patients with hypertension, but the dose of hydralazine was only 25 mg given orally, twice a day. In six patients with essential hypertension, Gjorup and Hilden'6 observed a variable response to intravenous hydralazine. They suggested that if the decrease in blood pressure was not marked, renal blood flow increased, whereas it decreased if blood pressure dropped markedly. Our data suggest that this might also be true in patients with CHF, as sodium retention during hydralazine, if it occurred, appeared to be associated with a fall in blood pressure. Schroeder'8 found no change in urea clearance or excretion of phenyl red in 50 hypertensives treated with 50-120 mg of hydralazine for 10-30 days, Despite the variability of some of these studies, the evidence suggests an increase in renal blood flow with little change in glomerular filtration rate as the usual response of hypertensive patients given hydralazine. A similar response is likely in normal subjects if the data obtained by Moyer et al.19 in nonhypertensive dogs are applicable to humans. Because the pathophysiology of CHF differs significantly from that of hypertension, we cannot readily assume that the renal responses to hydralazine would be the same in the two groups. In hypertension, the renal homeostatic mechanisms are altered toward increased salt excretion.20 In contrast, in CHF, the kidneys tend to retain salt and water, at least partly because of renal vasoconstriction.21 Thus, it might be expected that a vasodilator could improve salt excretion in CHF if renal perfusion is enhanced without a decrease in blood pressure. Data on renal vascular effects of hydralazine in patients with heart failure are scarce. Two studies-2' 23 have reported on the renal responses of patients with mitral stenosis given hydralazine, but these patients are not comparable to our study group. Judson et al.23 included five patients with "cardiac insufficiency" in their series, but four of the five were also hypertensive. Our study therefore represents one of the first attempts to analyze the effects of hydralazine systematically in nonhypertensive patients with CHF due to left ventricular dysfunction. In an uncontrolled study, Packer et al.24 noted a brisk diuresis in some of their refractory heart failure patients placed on maintenance hydralazine therapy, but no further analysis of renal function is described. Preliminary reports of improved renal blood flow with hydralazine administration in heart failure patients have also been presented by LeJemtel et al.,25 Mantle et al.26 and Cogan et al.27 In the patients of Cogan et al.,27 glomerular filtration increased insignificantly. Because we wanted to keep the study noninvasive VOL 61, No 2, FEBRUARY 1980 and were reluctant to water-load class III or IV heart failure patients, we did not measure para-aminohippurate or inulin clearance in our patients. Nonetheless, creatinine clearance increased, consistent with a rise in glomerular filtration rate. Because hydralazine is known to increase cardiac output in patients with CHE," 2 it is likely that the improved creatinine clearance was accompanied by an increase in renal blood flow. We can thus infer that in contrast to patients with hypertension, glomerular filtration rate and renal blood flow are increased by hydralazine in patients with CHF. This response could in part be attributed to the fact that renal blood flow and glomerular filtration rate are functionally reduced in CHF, probably because of renal vasoconstriction, which can then be relaxed as the cardiac output increases. Although we did not measure PRA in all patients, PRA did increase during the period of hydralazine administration in all five patients in whom it was measured. An increase in PRA also occurs when hydralazine is given to hypertensives, and has been thought to be related to the decrease in blood pressure. In this subgroup of five patients, renin increased even though blood pressure did not fall significantly and the control PRA tended to be elevated. In these five patients, no relationship was apparent between the change in mean blood pressure and change in PRA. Curtis et al.28 and Gavras et al.29 noted a wide range of values for resting PRA in heart failure patients receiving diuretics, with many patients having quite high levels. They postulated a role of renin in maintaining the abnormally high peripheral resistance observed in heart failure and noted hemodynamic improvement with inhibition of the renin-angiotensin system. These observations suggest that activation of the reninangiotensin system may tend to counteract the vasodilator effect of hydralazine in CHF, and could also contribute to sustained renal vasoconstriction. The combination of a converting enzyme inhibitor with hydralazine might therefore be appropriate for vasodilator therapy in heart failure. The rapidity of onset of changes in PRA and the duration of effect have not been studied, and our data are far too few to help define the time course of changes in PRA. In this study, neither weight loss nor diuresis occurred during the 3-day hydralazine period, despite the effect on creatinine clearance. Our patients were considered stable and reasonably well compensated before entry into the study. It is entirely possible that hydralazine administration to patients with CHF and acute volume overload would initiate or enhance diuresis. However, because of the instability of patients with volume overload during hospitalization, the present study was limited to patients who were relatively free of edema. The decrease in serum osmolality that occurred with hydralazine is probably related to changes in serum sodium concentration. Increased sodium excretion or water retention or both could alter the serum sodium concentration and the osmolality. As we noted no increase in body weight or decrease in urine output, RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al. Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 the slight (but statistically insignificant) increase in sodium excretion may be the major reason for the decrease in osmolality. The absence of a significant decrease in blood pressure or increase in heart rate is consistent with previous observations with hydralazine in heart failure."' 2 The dose of hydralazine chosen has been confirmed effective in increasing cardiac output, which allows systemic vascular resistance to fall without changing blood pressure significantly. Although we did not measure central hemodynamics, it is reasonable to presume that similar responses were attained in the patients in this study. In summary, our data show improved renal function during hydralazine administration in patients with CHF, as manifested by increased creatinine clearance. Although an occasional patient may tend to retain sodium in response to hydralazine, this apparently is confined to patients whose blood pressure falls. Although our data suggest that sodium retention is not likely to be an important factor in the majority of patients, the patients in our study received hydralazine only for a period of 3 days. Extrapolation of these findings to chronic therapy must be made with caution, and the efficacy of long-term hydralazine therapy in CHF remains to be established by longterm, controlled clinical trials. Acknowledgment We gratefully acknowledge the technical assistance of Irene LaSota and secretarial help of Margaret Chelmo. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. References 21. 1. Franciosa JA, Pierpont G, Cohn JN: Hemodynamic improvement after oral hydralazine in left ventricular failure: a comparison with nitroprusside infusion in 16 patients. Ann Intern Med 86: 388, 1977 2. Chatterjee K, Parmely WW, Massie B, Greenburg B, Werner J, Klausen S, Norman A: Oral hydralazine therapy for chronic refractory heart failure. Circulation 54: 879, 1976 3. Hollander W, Judson WE: Electrolyte and water excretion in arterial hypertension. II. Studies in subjects with essential hypertension after antihypertensive drug treatment. Circulation 17: 576, 1958 4. Ibsen H, Rasmussen K, Aerenlund Jensen H, Leth A: Changes in plasma volume and extracellular fluid volume after addition of hydralazine to propranolol treatment in patients with hypertension. Acta Med Scand 203: 419, 1978 5. Werk6 AL, Ek J, Ellasch H, Varnauskas R, Holmgren A, Bucht H: The effect of apresoline on pulmonary and renal hemodynamics in hypertensive cardiovascular disease and mitral stenosis. Nord Med 49: 397, 1953 6. Laslet LJ, DeMaria AN, Amsterdam EA, Mason DT: Hydralazine-induced tachycardia and sodium retention in heart failure: hemodynamic and symptomatic correction by prazosin therapy. Arch Intern Med 138: 819, 1978 7. Winer BJ: Statistical Principles in Experimental Design, 2nd ed. New York, McGraw-Hill, pp 261-308 8. Reubi FC: Renal hyperemia induced in man by a new phthalazine derivative. Proc Soc Exp Biol Med 73: 102, 1950 9. Judson WE, Hollander W: Comparative effects of intravenous and chronic oral 1-Hydrazinophthalazine on the cardiorenal hemodynamics and the excretion of sodium in hypertensive 22. 23. 24. 25. 26. 27. 28. 29. 327 patients with and without congestive heart failure. Clin Res Proc 2: 70, 1954 VanderKolk K, Dontas AS, Hoobler SW: Renal and hypotensive effects of acute and chronic oral treatment with 1Hydrazinophthalazine. Am Heart J 48: 95, 1954 Wilkinson EL, Backman H, Hecht HH: Cardiovascular and renal adjustments to a hypotensive agent (1-Hydrazinophthalazine: CIBA BA-5968: Apresoline). J Clin Invest 31: 872, 1952 Crosley AP, Rowe GG, Crumpton CW: The hemodynamic and metabolic response of the human hypertensive kidney to a standard dose of l-Hydrazinophthalazine (hydralazine). J Lab Clin Med 44: 104, 1954 Judson WE, Hollander W, Wilkins RW: The effects of exercise in the supine position on cardiovascular and renal function in hypertensive patients before and during chronic oral hydralazine therapy. J Lab Clin Med 49: 672, 1957 Crumpton CW, Crosley AP, Rowe GG: The hemodynamic, metabolic and electrolyte responses of the human hypertensive kidney to the intravenous administration of sodium p-Sulfamyl Benzoate. J Lab Clin Med 42: 797, 1953 Falch DK, Qdegaard AE, Norman N: Renal plasma flow and cardiac output during hydralazine and propranolol treatment in essential hypertension. Scand J Clin Lab Invest 38: 143, 1978 Gjorup S, Hilden T: The effect of hydralazine (Apresoline) on kidney function and sodium excretion. Scand J Clin Lab Invest 8: 273, 1956 Stein DH, Hecht HH: Cardiovascular and renal responses to the combination of hexamethonium and 1-Hydrazinophthalazine (Apresoline) in hypertensive subjects. J Clin Invest 34: 867, 1955 Schroeder HA: The effects of l-hydrazinophthalazine in hypertension. Circulation 5: 28, 1952 Moyer JH, Handley CA, Huggins RA: Some pharmacodynamic effects of l-hydrazinophthalazine (C-5968) with particular reference to renal function and cardiovascular response. J Pharmacol Exp Ther 103: 368, 1951 Buckalew VM, Puschett JB, Kinitzel JE, Goldberg M: Mechanism of exaggerated natriuesis in hypertensive man: impaired sodium transport in the loop of Henle. J Clin Invest 48: 1007, 1969 Cannon PJ: The kidney in heart failure. N Engl J Med 296: 26, 1977 Werk6 L, Varnauskas E, Ek J, Bucht H, Thomasson B, Bergstrom J, Eliasch H: Studies on the renal circulation and renal function in mitral valvular disease. II. Effect of Apresoline and noradrenaline. Circulation 9: 700, 1954 Judson WE, Hollander W, Wilkins RW: The effects of intravenous Apresoline (hydralazine) on cardiovascular and renal function in patients with and without congestive heart failure. Circulation 13: 664, 1956 Packer M, Moller J, Gorlin R, Teichholz L, Herman M: Dosedependent reduction in right and left ventricular filling pressures with hydralazine. Am J Cardiol 41: 420, 1978 LeJemtel T, Hellman C, Elkayam U, Strom J, Blaufox MD, Frishman W, Ribner H, Sonnenblick E: Hemodynamic and renal response to oral hydralazine therapy in severe heart failure. Circulation 56 (suppl III): 111-9, 1977 Magorien KD, Triffin D, Desch CE, Unverferth DV, Leier CV: Prazosin and hydralazine in congestive heart failure: drug- and dose-related variations in regional blood flow. Clin Res 27: 185A, 1979 Cogan J, Humphreys M, Carlson J, Rapaport E: Afterload reduction increases renal blood flow and maintains glomerular filtration rate in patients with congestive heart failure. Clin Res 27: 3A, 1979 Curtiss C, Cohn JN, Vrobel T, Franciosa JA: Role of reninangiotensin system in the systemic vasoconstriction of chronic congestive heart failure. Circulation 58: 763, 1978 Gavras H, Faxon DP, Berkoben J, Brunner HR, Ryan TJ: Angiotensin converting enzyme inhibition in patients with congestive heart failure. Circulation 58: 770, 1978 Effect of hydralazine on renal failure in patients with congestive heart failure. G L Pierpont, D C Brown, J A Franciosa and J N Cohn Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017 Circulation. 1980;61:323-327 doi: 10.1161/01.CIR.61.2.323 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1980 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/61/2/323.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/