Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Discussing Diagnosis and Natural History: Genetic Counseling Somali Refugees
Thanks to Lauren Grote, University of Dayton undergraduate student in the SURF Program (Summer
Undergraduate Research Fellowship), Cincinnati Children’s Hospital Medical Center for her work as a
contributing author for this case.
Commentary by Marie Runyon, MS, Genetic Counselor, Hennepin County Medical Center, Minneapolis,
MN
Learning Objectives
By the end of this case, genetic counselors will be able to:
1. Summarize the challenges faced by refugees prior to and after arriving in the U.S.
2. List the characteristics of health care provision that convey respect for Somali culture.
3. When discussing diagnosis and natural history, apply the mnemonic device, ETHNIC, to
understand how culture may affect a patient’s treatment.
A Somali family arrived in the United States as refugees three months ago. Upon receiving the typical
medical screening, a U.S. public health clinic discovered their 8 year old son, Asad, has sickle cell
anemia. The family acknowledges that their son endured chronic pain, headaches, and fevers from early
on in life. However, their traditional healing methods had previously offered respite from his pain, and they
are confused as to why the diagnosis should change their efforts. They have been referred to genetic
counseling to discuss the diagnosis and natural history of sickle cell anemia. On the day of their
appointment, the entire family including Asad’s mother, father, three healthy siblings, and two paternal
uncles arrive one hour early. An interpreter was present upon arrival but Asad’s father refused his
services.
Personal Reflections
What is your first reaction to this situation?
What experience do you have working with refugees?
What experience do you have working with Somali families?
Why do you think the entire family was present?
Why do you think Asad was not diagnosed with sickle cell disease in Somalia?
Perspectives
What might the family be thinking and feeling regarding the genetic counseling session?
What should the counselor consider before the appointment begins?
What are some potential difficulties that could arise in this situation?
Refugee Defined
According to the 1951 Refugee Convention, a refugee is a person who has “a well-founded fear of being
persecuted for reasons of race, religion, nationality, membership of a particular social group or political
opinion, is outside of the country of his nationality and is unable, or owing to such fear, is unwilling to avail
himself of the protection of that country…” (United Nations, 1951, p. 16). The key piece of this definition is
that refugees do not voluntarily choose to move. The term refugee is often used interchangeably with
several other terms including migrant and asylum-seeker. A migrant makes the choice to immigrate to
another country in search of a better quality of life. Reasons for migration often include increased
opportunities for careers, education, and living arrangements (The UN Refugee Agency, 2007). An
asylum-seeker is someone who claims to need international protection as a refugee, but whose status
has not yet been confirmed by the country of asylum. If the asylum-seeker is not granted refugee status,
he/she may be sent back to his/her home country (The UN Refugee Agency, 2009).
There are a few other groups of people considered to have refugee-like status. Internally displaced
people (IDP) are forced to move to another part of the country to avoid ill effects of war, government
tyranny, and human rights violations but they never cross international borders. Stateless people are not
considered to be a national of any state due to government discrimination regarding minority groups,
conflicts between state laws, and failure to include all residents when a state secedes. People who were
once refugees but have voluntarily returned home in safety are called returnees (The UN Refugee
Agency, 2007).
The Refugee Experience
The refugee experience is typically divided into three stages: premigration, migration, and postmigration.
Prior to escaping from their home country, refugees are in the premigration stage. This phase is often
accompanied by chaos, violence, sexual abuse, war, anxiety, and torture. When the migration phase
begins the refugees may be uncertain about the present and the future. On the trek to an asylum country
refugees are most concerned about food, water, and shelter. They also experience underlying anxiety
about the future and their reception and treatment upon arrival (Crowley, 2009). Any person seeking
refugee status is interviewed by the office of the United Nations High Commissioner for Refugees
(UNHCR). If qualified as a refugee, UNHCR seeks to find a durable solution for the refugee’s situation.
There are three such solutions including: voluntary repatriation to the home country, integration into the
country of asylum, and resettlement into a third country. The best solution for any refugee is to allow them
to safely return to their home country. If a refugee’s home country is no longer safe, then the second best
choice is to assimilate him/her into the country of asylum. If neither option is appropriate, resettlement into
a third country is the chosen alternative (Cultural Orientation Resource Center, 2009). Countries including
Australia, Canada, Denmark, Finland, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and
the United States have ongoing resettlement programs. Other countries accept refugees on an individual
basis. However, only about 1% of all refugees are actually offered resettlement. The other 99% of
refugees return home or reside permanently in a country of asylum (U.S., 2009).
To be accepted into the United States Refugee Resettlement Program, a refugee must be referred by the
U.S. embassy in the country of asylum or UNHCR. After receiving a referral, a representative from the
Immigration and Naturalization Service travels to interview the refugees in their country of asylum. There
are three characteristics that make a person eligible to be resettled in the U.S.: a history of persecution,
membership of an ethnic or religious group that is considered by the United States to be of “special
humanitarian concern,” or relation to a resettled refugee as a spouse, parent, or unmarried child in the
U.S. (U.S., 2009). Once approved, the refugee will be matched with one of ten U.S. resettlement
organizations. In 2008, only one third of all the refugees and asylum-seekers who sought settlement in
the United States were approved.
Prior to coming to America, refugees must complete several procedures that can take anywhere from two
months to two years to complete. First, the resettlement agency must assure the Department of State
that it has the resources to accept the refugee. Then, each refugee must be medically screened for any
public health concerns. The overseas medical screening looks for certain conditions that would give
reason to deny a person entry into the United States. These conditions include tuberculosis, Hansen’s
disease, human immunodeficiency virus (HIV) infection, AIDS, certain sexually transmitted diseases, drug
abuse or addiction, and a current or past mental or physical disorder associated with harmful behavior.
However, there is a waiver process to allow some individuals with these conditions into the U.S. based on
their personal circumstances. All other conditions are not considered to be detrimental to public health
and do not prevent entry into the U.S. The refugee is then subjected to a specific security clearance
depending on his/her country of origin. Lastly, all refugees must receive American cultural orientation
concerning what to expect in America during the resettlement phase (U.S., 2009). This cultural
orientation, lasting between 3 hours and a few days, consists of pre-departure processing, travel
arrangements, rights and responsibilities of refugees, housing, employment, transportation, education,
health care, money management, cultural adjustment, and other topics (United, 2008).
Travel to the United States is coordinated by the International Organization for Migration. Refugees who
cannot pay their way are required to repay the U.S. government once they are established (U.S., 2009).
Upon arrival, the Reception and Placement Program coordinates the resettlement process by ensuring
appropriate agencies have been assigned to the refugee (United, 2008). An agency arranges for housing
and basic supplies and refers refugees to employment and social services (Cultural, 2009). Upon arrival
at the airport, each passenger is assessed for signs of illness. Those with previously acknowledged
conditions are reminded to report to a local health department for evaluation. The airport personnel also
send notice to the state health department to ensure follow up. Within the first 90 days, new medical
exams are conducted for all refugees, regardless of previous conditions. There are four levels of
examination provided. Level I evaluates solely for tuberculosis. Level II consists of a complete physical
exam and an assessment of immunizations. Level III involves listening for a normal heart rate or
abnormal lung sounds as well as other testing as appropriate. Level IV entails case management, if the
patient’s condition warrants it. Refugees with health problems are then referred to a local physician or a
health department clinic nearby. Children have measurements taken to evaluate their growth, are
assessed for their developmental milestones, and screened for genetic conditions including sickle cell
anemia and thalassemia. Adults may receive education about HIV, cancer, and cardiovascular disease
(Virginia, 2004).
During the first thirty days in the United States all refugees are registered for a social security number,
children are enrolled into school, and English language training is provided. Within the first six months,
refugees are required to find a job. After one year, refugees can apply for Permanent Resident Alien
status and after five years, they are eligible to apply for U.S. citizenship (U.S., 2009).
The postmigration phase presents an entirely new set of concerns for refugees. Upon arrival to their new
country, refugees may feel excitement and relief. As reality sets in they may be filled with confusion,
bewilderment, fear and/or anxiety. While they may have escaped previous problems, new challenges
quickly appear. The refugees must now begin the process of acculturation. “Acculturation comprehends
those phenomena which result when groups of individuals sharing different cultures come into continuous
first-hand contact, with subsequent changes in the original culture patterns of either or both groups”
(Abreu & Kim, 2001, p. 395-396). As discussed in Abreu & Kim, 2001, Berry et al. presented four
acculturation attitudes for the adherence to host and indigenous cultures: integration, assimilation,
separation, and marginalization. Integration is when an individual continually interacts with the host
culture while still remaining proficient in their indigenous culture. Assimilation is when a person rejects
their indigenous culture in favor of the host culture. Separation occurs where the value is placed solely
with the native culture and persons of the host culture are avoided. Marginalization includes individuals
who maintain interest in neither culture (Abreu & Kim, 2001).
Some of the struggles refugees may encounter during the acculturation process include: learning a new
language, finding a job, adjusting to new legal structures, and supporting themselves financially. Social
hierarchies may collapse as children tend to learn English more quickly than adults and become
interpreters for their elders. Religious values may change as western dress and/or dietary habits do not
coincide with previous beliefs (Mercer, 2004). The attitudes listed above are examples of how refugees
may relate to their host and indigenous cultures, but the acculturation status of each individual must be
specifically assessed.
Before coming to the United States, many Somali families lived in refugee camps with little food or water
and inadequate medical supplies. They may have faced sexual abuse and the death of loved ones. In the
U.S., these families are continuing to cope with past experiences and may have trouble adjusting to their
new environment. During the immigration process, many families lose their family systems and
experience a loss of support. They may feel isolated in the United States and struggle to achieve a new
family balance. Children often become responsible for paying bills, reading mail, and communicating with
the outside world due to their English language proficiency, thus having power over the parents in certain
situations. Not only do parents face difficulties learning the language, but they experience problems
holding jobs or finding jobs that pay above minimum wage, acquiring housing for their large families, and
simply keeping food on the table (Alarcón et al., 2007).
Health Disparities
Refugees often face health disparities, regardless of their country of origin. Health care in the United
States is expensive, and frequently, a lack of insurance and impossible payment plans discourage many
refugees from seeking necessary health care. They may opt instead to seek health care services only in
emergency situations which can require more complicated methods of treatment as well as more
expensive procedures. For certain refugee populations, preventative treatment is not used or understood
(Burgess, 2002). Standard health screenings for conditions such as high blood pressure, diabetes, and
depression are not typically completed on refugees. Untreated chronic conditions and mental health
problems are common in the refugee population (Minnesota Immigrant Health Task Force, 2005).
Refugees who can afford health care often avoid it due to language and cultural barriers. The inability to
effectively communicate medical history, current needs, and personal health practices may result in
misdiagnosis and lack of adherence to medication regimens (Minnesota, 2005). According to Burgess,
2004, the refugee population is “prone to medical mistakes.” Because health care providers specifically
trained to work with refugees are not frequently incorporated into health care delivery systems, it is
essential for other physicians and counselors to be culturally aware when treating refugee patients.
Cultural, language, and educational barriers may limit quality of care. Many new refugees may feel more
comfortable with a physician of the same gender or race. In fact, less acculturated minorities tend to trust
and prefer an ethnically similar counselor (Atkinson, Morten, & Sue, 1998).
Medical care of refugees is often impacted by the inability to accept the past and move forward. The
influence of trauma on an individual varies based on the duration of the traumatic event, the number of
times the event occurred, personal coping skills, personality characteristics, and the presence of a
support system (Schuchman & McDonald, 2004). Past and current challenges faced by refugees may
generate a “‘collision course’ with enormous mental health implications” (Alarcón et al., 2007, p. 582).
Each group of refugees, and each individual refugee, has different experiences and challenges. We will
focus on general health care issues relating to the Somali refugee population.
Somalia: A Country and Its Culture
Until 1949, when the nation became a territory of the U.N., Somalia was controlled by England, Ethiopia,
France, and Italy. In 1960, Somalia was granted independence as a democratic nation. After nine years,
General Barre led a coupe and created a socialist military government which was, at first, highly
supported. As years passed, dissention grew and clan-based militias were formed. Civil war erupted in
1988 and since Barre’s overthrow in 1991, the various militias have contended for control (Diversity,
2007). Prior to the civil war, Somalia had an estimated population of 7.7 million people. Forty-five percent
of the population has been displaced internally or fled the country altogether and around 400,000 people
have died of famine, disease or have been killed in the war (Noor & Putman, 1993). Thousands of
refugees initially sought protection in Kenyan refugee camps directly across the border. However, clan
fighters were located in very close proximity and often came into the camps to prey on the refugees,
rendering these camps unsafe (Adams & Assefi, 2002). Currently, 561,000 Somalis are seeking refuge in
other countries; this makes them the third largest group of refugees in the world (The UN, 2009). In 2008,
2,523 Somali people were admitted to the United States as refugees (U.S. Department, 2009).
Somalia is slightly smaller than the state of Texas and is bordered by the Indian Ocean, Gulf of Aden,
Ethiopia, and Kenya (Alarcón et al., 2007). The population is mostly rural, consisting of farmers and
herders who share a uniform culture, language, and religion (Diversity, 2007; Lewis, 1996). Somalis
speak the language Somali, though many people also speak Arabic and Swahili. A small percentage of
people speak English as well (Noor & Putman, 1993). Most members of the Somali population are Sunni
Muslims. Their culture is intertwined with Islamic tradition affecting social customs, dress, diet, gender
roles, and attitudes (Lewis, 1996; Diversity, 2007). In urban areas of Somalia and in the United States,
many women dress according to western cultural norms. However, some women follow the Islamic
tradition which requires them to be covered from neck to ankle in non-form fitting clothing. In addition,
women may wear veils to cover their faces. Men also have dress requirements and are often covered
from neck to knee (Diversity, 2007).
(Central, 2009)
Family Life
Family is the ultimate focus in the Somali community. Elders are respected and addressed as “aunt” and
“uncle” even if there is no relation. Men are in charge of the household, at least in public, but Somali
women play major roles in keeping the finances and supporting the children. In fact, most women are
forced to find work outside of the home due to financial difficulties caused by the war. There is a great
deal of community support in Somalia that makes it possible for mothers to be away from the home.
Childbearing usually begins immediately after marriage because the status of a Somali woman is
enhanced based on the number of children she has. There is no concept of planning or child spacing in
Somali culture other than abstaining from sex while the mother is breastfeeding. Most births occur at
home with a midwife. After birth, the mother and baby stay inside for forty days while the female relatives
and friends visit to help take care of them. They bring certain foods and teas for the mother. Both mother
and child wear special jewelry to ward off the evil eye (see Medical Beliefs and Traditional Healing
below). Incense is burned twice a day to protect the baby from ordinary smells of the world. After the 40
day period, a naming ceremony is held. The child’s first name is original, given specifically to him or her.
The child’s second name is the name of his/her father and the third is of the paternal grandfather (Lewis,
1996).
Medical Beliefs and Traditional Healing
According to Somali tradition, illness can be caused by evil spirits, God, or one’s own or others’ behaviors
(Children’s, 2003 & Schuchman, n.d.). God may use the illness as a form of punishment, or it may simply
be God’s decision to give an illness to someone (Children’s, 2003). It is believed that humans can cause
one another to be ill; this is called the “evil eye.” The concept of the “evil eye” entails purposeful or
inadvertent praise of another person, causing harm or illness to occur. For example, Somali mothers are
often upset if the doctor compliments their child by describing him/her as “big and fat.” They fear that the
evil eye will harm their child (Alarcón et al., 2007). Illnesses such as measles, hepatitis, chicken pox,
mumps, hunch-back, broken bones, and tuberculosis are treated by traditional healers. These healers,
typically men, have learned their expertise from family members. To cure these diseases they use
combinations of fire-burning, herbs, and prayer. Fire-burning involves heating one end of a stick from a
special tree and applying it to various points on the skin to cure an illness. Hepatitis, tuberculosis, and
diarrhea are cured by applying the stick once to each wrist and four times to the abdomen to stimulate the
immune system. Malnutrition is treated by applying the stick to the head in order to reduce the person’s
head size. Herbs and prayer are used to cure other ailments such as seizures, backaches, stomachaches, rashes, and more (Lewis, 1996; Children’s, 2003). Somalis also use massage therapy with certain
oils primarily as treatment for pain, headaches, and backaches (Diiriye, Guerin, Guerin, & Yates, 2004).
Spirit possession is believed to be another cause of some illnesses in the Somali culture. Every
individual has spirits inside of them and angering those spirits can lead to fever, headaches, dizzy spells,
or weakness (Children’s, 2003). Psychotic symptoms are attributed to spirit possession as well. In order
to cure an illness caused by spirits, a ceremony led by a traditional healer or waddad is performed that
includes eating special foods, incense burning, and readings from the Koran (Alarcón et al., 2007; Lewis,
1996). The chosen readings are selected carefully based on the condition and can be read for a few
hours or a few days (Diiriye et al., 2004).
Differences in Healthcare: Somalia versus the United States
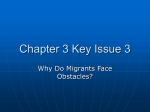
There are several differences concerning healthcare between Somalia and the United States. The table
below lists the main variations in policies for each country. The countries have differing laws regarding
specific practices such as newborn screening. In the United States, the newborn screening process
requires sickle cell disease screening in every state, and thus the majority of cases are discovered early
after birth (Department, 2009). Despite a high incidence of consanguinity and hemoglobin disorders in
the general area of the world that includes Somalia, there has been slow progress in implementing
newborn screening programs in many countries in the Middle East and North Africa (Saadallah, 2007).
According to the International Society for Neonatal Screening “there is no newborn screening in Somalia”
(J.G. Loeber, personal communication, July 21, 2009). There are also differences regarding
appointments and expectations. The Somali culture’s concept of time is relaxed, therefore appointment
times are viewed more as general suggestions. A family may arrive an hour early or late to the health
care appointment. Variations on physical examinations are also present. In Somalia, many women cover
their body based on religious beliefs. Special care must be taken to preserve their modesty during a
physical examination. United States health care providers must be careful to respect their modesty while
not compromising the necessary exam (Adams & Assefi, 2002).
Somali Health Care System
Government owned/managed system
Centralized system
Focus on curative medicine
On-the-spot diagnosis & treatment
Few diagnostic tests
Questions pertain to current illness
Medications usually prescribed
Prescriptions free while in hospital
Payment for services: low cost/free
No appointment necessary
Predictable waiting times
No forms to fill out: oral culture
No insurance needed
Spirituality acknowledged
Sickle Cell Disease
United States Health Care System
Combined public/private system
Decentralized
Focus on preventive medicine
Complex referral and triage systems
Many diagnostic tests used
Many questions re: history & family
Medications not always prescribed
Prescriptions never free
Services typically expensive
Appointments required – weeks or months ahead
Unpredictable waiting times
Many forms: literacy required
Insurance necessary
Body, mind & spirit usually separated
Clinical effects of sickle cell disease include variable degrees of hemolysis and episodes of vascular
occlusion resulting in tissue ischemia and chronic organ dysfunction. Hemolysis can cause jaundice,
chronic anemia, delayed growth and sexual maturation, and other crises. Tissue ischemia can cause
injury to all organs of the body especially the brain, kidneys, lungs, and spleen. Typically, the earliest
signs of sickle cell disease are the swelling of hands and/or feet and severe pain in the extremities, back,
chest, abdomen, and head. The pain is what most often brings sickle cell patients into the hospital and
causes the greatest disruptions to the activities of daily living (Vichinsky & Schlis, 2006).
Sickle cell anemia is inherited in an autosomal recessive manner. Parents of patients with sickle cell
anemia must have both passed on the affected Hb S gene for their child to be affected. For other types of
sickle cell disease, parents must pass on different hemoglobin, beta mutations. Each sibling born to
parents who are carriers has a 25% chance of being affected, a 50% chance of being a carrier, and a
25% of being unaffected and not a carrier (Vichinsky & Schlis, 2006). These percentages also apply to
any subsequent pregnancies a family may have. Sickle cell disease is most common in persons of
African, Mediterranean, Middle Eastern, and Indian ancestry although it can affect people of any
background. In African-American populations, a mutated copy of Hb S is found in 8-10% of people.
Therefore, every year in the United States, about 2,000 African-Americans are born with sickle cell
anemia.
It is essential to have lifetime care for this disease to prevent early death, morbidity, and to increase
quality of life. Parents, providers, and the affected individual all need to be properly educated in order to
make appropriate use of medical care. All families need to understand the importance of medications
and maintenance visits, be aware of warning signs, have access to a 24 hour medical facility, and
develop plans to deal with episodes of pain based on the severity. Patients should know to avoid
dehydration, extreme temperatures, and physical exhaustion. Most affected individuals benefit from
routine screenings that assess developmental and/or neurocognitive progress, nutritional and dental
health, and assessments regarding support systems, lifestyle, and availability of resources. Several tests
including liver function tests, assessments of iron status, a cbc and reticulocyte count, BUN, urinalysis,
and serum concentration of creatinine must be administered yearly to monitor the disease (Vichinsky &
Schlis, 2006).
The Genetic Counseling Session
Current genetic counseling job tasks were determined by the American Board of Genetic Counseling as
the outcome of a Genetic Counseling Practice Analysis (Hampel et al., 2009). The following is a list of
the Diagnosis and Natural History tasks:
1. Formulate counseling agenda
2. Integrate natural history, characteristics, and symptoms of working diagnosis
3. Incorporate client specific findings and needs
4. Develop management plan
5. Convey information about the following:
a. diagnosis/indication
b. etiology
c. natural history
d. variable expressivity
e. penetrance
f. prognosis
g. prevention
h. treatment
i. management
6. Assess client understanding and response
7. Tailor management plan according to client circumstances
8. Modify counseling based on client’s understanding and response
Many Somali immigrants will only seek genetic counseling after receiving a referral from another provider.
Most will not know what genetic counseling entails or understand the potential benefits. This situation
applies to our case study, as the family was referred after a routine medical screening for refugees.
Genetic counseling Somali refugees may be conducted through an interpreter, which presents additional
challenges to communication and time. When beginning the counseling session with this family, the
counselor should “first introduce her/himself and ask all the family members to do the same. While only
one member of the family may speak with me throughout the session, [this inclusive introduction] allows
me to welcome every member of the family. I feel this helps show that I acknowledge that the family is an
important part of the patient’s care” (Runyon (2010), personal communication). The genetic counselor
should then discuss the nature of genetic counseling. It is important that the clients understand the
purpose of the appointment and be aware of the anticipated proceedings. The genetic counselor should
make an effort to assess acculturation. During this step it is crucial to establish trust with the family; some
Somalis have acknowledged withholding information from providers due to mistrust. They may harbor
fears that their confidentiality could be compromised during the session. Greeson, et al. (2001) suggest
using empathy to establish this trust. By recognizing the patients’ potential doubts about the session and
asking questions regarding the patient’s perceptions of and hopes for the appointment, a counselor can
build rapport with the client (Greeson, et al., 2001).
It can be difficult to describe genetic conditions to a family of a different culture. When explaining sickle
cell anemia, a counselor may need to explain the basic genetics behind inheritance before describing the
specific disorder. The counselor speaking with Asad’s family might say the following:
“The body is made up of millions of cells. Each cell contains information known as DNA that
makes us who we are today. Our DNA is located on structures called genes, which are located on
the chromosomes inherited from both parents. There is no operation to fix DNA, genes or
chromosomes if they are changed (or damaged). This is the case with your son, Asad. He
inherited two changed genes that cause sickle cell disease and there is no way to fix them. You
are already doing a good job keeping Asad feeling well. Let’s talk more about how to keep Asad
from having fevers, headaches and pain.”
While describing sickle cell disease to this family, it is important to keep their cultural beliefs in mind. In
order to appreciate how the Somali culture will affect the patient’s treatment, we suggest the use of the
mnemonic tool, ETHNIC. “ETHNIC is neither a scoring sheet nor a detection scheme to uncover hidden
cultural issues but rather a clinically applicable tool for eliciting and negotiating cultural issues during
healthcare encounters” (Kobylarz et al., 2002). ETHNIC helps health care providers build a framework to
create an atmosphere that is welcoming and understanding of the patient’s diverse perceptions on
sickness and symptoms, and to include various healing techniques of their culture.
E: Explanation
Consider asking such psychosocial questions as:
- How do you think this illness happened to you?
- What do you think may be the reason you have these symptoms?
- What do friends, family, and others say about these symptoms?
- Do you know anyone else who has had or has this kind of problem?
- Have you heard about/read/seen it on television/radio/newspaper/internet?
- If the patient cannot provide an explanation, consider asking them “What concerns you
about the problem?”
Some individuals may be reluctant to give their impression because they feel that diagnosis is a
doctor’s job. However, the use of normalizing phrases like “I often learn important things from
hearing people’s ideas about why they are ill and what they think should be done about it” can
gently prod patients into meaningful discussion (Kobylarz et al., 2002).
Case Application
During the case study described above, the counselor implements the first step of the ETHNIC
technique by exploring the family’s explanations for their Asad’s condition. The family explains
that God created their son with this illness and that he is meant to experience these symptoms.
Their family and friends suspect that an evil spirit may be the cause because Asad appeared fine
for the first two years of his life. They believe that spirits are often the cause of headaches and
fever, which Asad experiences frequently. Their strong Muslim faith supports their belief that the
illness is consistent with God’s will. Prior to a few weeks ago, the family had never heard of sickle
cell disease.
“In my experience with the Somali population, I have found that the belief in God’s will is very
powerful. A majority of the community may share the belief that a condition or illness has affected
a family members because it was as God wished. In my counseling sessions when addressing
the natural history/inheritance issues I try to address “how” it happened rather than “why” it
happened. This helps to show the patient that I acknowledge their “why.” It also helps keep the
discussion open as I do not have to make a statement that may be seen as a challenge to the will
of God. It also appears to help the patients as they do not feel that they are challenging the will of
God by discussing the condition” (Runyon (2010), personal communication).
T: Treatment
Consider asking such psychosocial questions as:
- What kind of medicines, home remedies, or other treatments have you tried for the
symptoms?
- Is there anything you eat, drink, do, or avoid on a regular basis to stay healthy?
- What kind of treatments are you seeking from me? (Kobylarz et al., 2002).
Case Application
The family opens up about various treatments they have used to help Asad. Initially they relied on
the Koran (Qur’an) to heal him, but the pain would only subside momentarily. They began to
implement other techniques including fire burning, herbs, and more frequent prayer. When Asad
was old enough to identify and express where he felt pain, they began to use massage
techniques with special oils to ease the aches.
As Muslims, the Somali people are forbidden to eat pork or lard or to drink alcohol. They follow
strict practices when preparing meat for a meal. They feel that these behaviors keep them healthy
and pure. Consider how the family’s observance of Ramadan may influence treatment
procedures. Ramadan is the ninth month of the Muslim calendar, when it is believed the Holy
Koran Qur’an “was sent down from heaven, a guidance to men, a declaration of direction, and a
means of Salvation.” During this entire month, Muslims fast (the Fast of Ramadan), abstaining
from food and drink during daylight hours. During Ramadam, Muslims concentrate on their faith
through workship and contemplation, and spend less time on everyday concerns. Smoking and
sexual relations are also forbidden during fasting. Because the timing of Ramadan is based on
the lunar calendar, in some years, Muslims are obliged to fast during long and hot summer days.
Fasting can induce physiologic changes that may impact the homeostasis of individuals with
chronic conditions, so it is important for health care providers to be sure that Muslim patients are
willing to take prescribed pills, etc during Ramadan. Consider whether a modified dosage
schedule will work, instead. In this case, Asad is still young and he is not yet required to fast, but
the family could be wondering whether Asad’s treatment will interfere with keeping the holiness of
Ramadan in the future.
The family is not sure what treatments, if any, they would like to learn from the session. They are
confused because their son had survived just fine in Somalia without knowing he had sickle cell
anemia. However, family is extremely important to their culture, and they do not want Asad to
suffer. They express interest discussing possible treatment options.
H: Healers
Consider asking such psychosocial questions as:
- Who else have you sought help from for this illness?
-
Have you sought help from alternative or folk healers, friends, or other people who are
not doctors for help with your problems?
Keep in mind that for more acculturated individuals, asking whether they rely on folk healers may
be insensitive. Instead, remember that this area includes all alternative health care, including
widespread Western alternatives such as seeking care from chiropractors and taking herbal
supplements (Kobylarz et al., 2002).
Case Application
Because this family has only been in the United States for three months and they have just
recently learned about their son’s condition, they most likely have not seen other providers in the
U.S. In Somalia, their family relied on a cousin who was a traditional healer. He was able to
preside over Koran (Qur’an) readings and fire burning procedures. Any immediate concerns
regarding Asad were addressed directly to the cousin.
N: Negotiate
Brainstorm mutually acceptable options by asking the following questions:
- What is the best way for me to help you?
- What options would be best, from your perspective?
Remember that your negotiations may extend beyond the patient to caregivers or extended family
members, depending on the cultural context of the encounter. The negotiation should seek to find
a solution agreeable to ALL participants in the patient’s care or decision-making unit (Kobylarz et
al., 2002).
Case Application
Your client’s family has already expressed uncertainty regarding Western treatment. They are
confused by and/or unaware of the available treatments. The family emphasizes that their
treatment in Somalia had worked well and they would like to continue to treat their son in the
same manner.
I: Intervention
Determine an intervention with your patient.
- This may include incorporation of alternative treatments, spirituality, and healers, as well
as other cultural practices (e.g., foods eaten or avoided both in general and when sick).
Case Application
It is important to emphasize the necessity of ongoing medical treatment and tests even if the
patient is currently feeling well. Asad should be monitored to avert the need for any extensive
treatments that may interfere with their beliefs.
The family expresses concern over finding a traditional healer in the United States who can help
their son. The counselor will talk to a social worker who is serving the Somali community to help
identify a local healer.
C: Collaborate
Collaborate with patient, family and/or healers to execute the intervention. Ask:
- How can we work together on this and who else should be involved? (Kobylarz et al.,
2002).
It is helpful to understand that finding a successful intervention may not be a one-time process,
and that these steps may need to be repeated to come to an intervention that is both culturally
sensitive and acceptable to the family. However, even if one clear intervention does not emerge
from the first encounter, using ETHNIC can help build essential trust between the patient and the
provider, thereby beginning to bridge the cultural gap.
Case Application
Everyone agrees that massage therapy should be used to treat Asad’s pain (Sickle, 2004). This
therapy has already been effective for the boy. The genetics professionals recognize the family’s
need to continue traditional health care treatment methods; they do not think that these will
interfere with the recommended Western medicine procedures such as routine testing. Shortly
after the doctors acknowledge the importance of continuing their traditional healing methods, the
family agrees to yearly checkups and testing in the medical center.
Summary: Discussing Diagnosis and Natural History
Providing genetic counseling to refugees presents unique challenges for diagnosing and managing
genetic conditions. This case discusses the challenges that might present in genetic counseling a Somali
family with fairly traditional beliefs and practices. Therefore, in this case, an interpreter was requested.
However, it is not uncommon for a Somali man to refuse an interpreter, even if he is the only member of
the family who can speak English. This conflict of wishes and needs presents a difficult dilemma for the
genetic counselor who wants to be sure both parents are fully informed about the condition--especially
the mother, who is the primary caretaker of the children.
When a genetic counselor's practice includes individuals who have come to the U.S. as refugees, the
counselor should ask him/herself:
•
What do I know about the socio-political situation of the client’s country of origin?
•
Do I have enough background information to be able to help this family?
•
Do I know why this family specifically sought refuge in the U.S.? Did they already have relatives
in the U.S.? If so, how extensive are the family’s U.S. roots?
It is important to realize that Somali refugees have been coming to the U.S. for several decades.
Therefore, not all patients of Somalian background will be as “traditional” as the family in this case.
Genetic counselors should assess the acculturation status of clients who are refugees.
•
Because this family has only been in the U.S. for three months, is it reasonable to presume that
they are most likely in the integration phase of acculturation?
•
Might the various family members find themselves in a range of stages in the acculturation
process?
•
Who exactly are the family members in the room? Why did they come to this appointment?
•
Sickle cell anemia is a serious disease with few "visible" features. What is the family's sense of
Asad's health and his illness? Do they consider illnesses with visible features more or less
burdensome than conditions that are visibly evident?
The focus of this case was on disease management. We used the mnemonic ETHNIC to help determine
the family's preferences in managing Asad's condition. ETHNIC also elucidated the role of the family's
Muslim faith in explaining the condition. In a real genetic counseling case, there would be other salient
issues to be addressed, including recurrence risk, genetic testing of other family members, and prenatal
diagnosis. If the counselor is successful in laying the groundwork of trust during the initial session, the
family will continue to obtain care from genetics professionals in the future for ongoing treatment,
discussion of preventative measures, and genetic counseling.
Cultural Competence
•
Allow patients extra time and return visits to confer with trusted family and community members
about important decisions.
•
Openly share your interest in learning about different cultures and beliefs with medical
interpreters. Interpreters can provide suggestions for helping you communicate more effectively
with individuals of specific backgrounds.
•
Be sure to explain the health care service of genetic counseling. Refugees may not understand
what to expect.
•
At the start of the session, introduce yourself, and ask everyone present to introduce themselves.
•
Use simple words and diagrams.
•
Provide context for any information you provide.
•
Use cultural mnemonics such as ETHNIC to understand a patient’s perceptions of health and
illness, build trust, and help patients with medical decisions and management.
•
Explain “how” a condition occurs rather than “why” it occurs. By doing so, the medical/genetic
and the spiritual or alternative explanations will complement, not contradict, each other.
References
Abreu, J.M. & Kim, B.S.K. (2001). Acculturation Measurement: Theory, Current Instruments,
and Future Directions. In J.G. Ponterotto, J.M, Casas, L.A. Suzuki & C.M. Alexander.
(Eds.), Handbook of Multicultural Counseling (2nd Ed.) (p. 394-424). Thousand Oaks, CA: Sage
Publications.
Adachi Sueyoshi, L., Rivera, L., & Ponterotto, J.G. (2001). The Family Genogram as a Tool in
Multicultural Career Counseling. In J.G. Ponterotto, J.M, Casas, L.A. Suzuki & C.M. Alexander.
(Eds.), Handbook of Multicultural Counseling (2nd Ed.) (p. 655-671). Thousand Oaks, CA: Sage
Publications.
Adams, K. & Assefi, N. (2002). Primary Care Refugee Medicine: General Principles in
the Post-Immigration Care of Somali Women. Primary Care Update for Ob/Gyns, 9(6), 210-217.
Alarcón, R.D., Lapeyre, A.C., Logan, K.M., Scuglik, D.L., & Williams, M.D. (2007,
December). When the Poetry No Longer Rhymes: Mental Health Issues Among Somali
Immigrants in the USA. Transcultural Psychiatry, 44(4), 581-595.
Atkinson, D.R. Morten, G., & Sue, D.W. (1998). Counseling American Minorities (5th ed.).
Boston: McGraw-Hill.
Bemak, F & Chung, R.C.Y. (2002). Counseling and Psychotherapy with Refugees. In P.B.
Pederson, J.G. Draguns, W.J. Lonner, & J.E. Trimble (Eds.). Counseling Across Cultures (5th
ed., p. 209-232).
Burgess, A. (2004, March/April). Health Challenges for Refugees and Immigrants. Refugee
Reports, 25(2). Retrieved from
http://www.refugees.org/data/refugee_reports/archives/2004/mar_apr.pdf
Central Intelligence Agency. (2009). The World Factbook. Retrieved November 5, 2009, from
https://www.cia.gov/library/publications/the-world-factbook/index.html
Children’s Hospitals and Clinics of Minnesota. (2003, August). Cultural and Medical
Traditions: Somali Culture and Medical Traditions. Retrieved from
http://www.childrensmn.org/Web/ClinicsAndDepts/025020.pdf
Crowley, C. (2009). The Mental Health Needs of Refugee Children: A Review of
Literature and Implications for Nurse Practitioners. Journal of the American Academy of Nurse
Practitioners, 21(6), 322-331.
Cultural Orientation Resource Center. (2009). US Refugee Program. Retrieved November 5, 2009, from
http://www.cal.org/co/refugee/#1
Department of State: Bureau of Population, Refugees, and Migration. (2009, March).
Summary of Refugee Admissions. Retrieved from
http://www.state.gov/documents/organization/120384.pdf
Diiriye, R.O., Guerin, B., Guerin, P., & Yates, S. (2004, July). Somali Conceptions
and Expectations Concerning Mental Health: Some Guidelines for Mental Health
Professionals. New Zealand Journal of Psychology, 33(2), 59-67.
Diversity Council. (2007). Somali Culture: An Overview. Retrieved from
http://www.diversitycouncil.org/toolkit_preview/Resources_TipSheet_SomaliCulture.pdf
Fong, R. (2004). Culturally Competent Practice with Immigrant and Refugee Children and
Families. New York: Guilford Press.
Food Security Analysis Unit, Somalia. (2007, December). Somali Knowledge Attitude and
Practices Study (KAPS). Retrieved from http://www.mihv.nonprofitoffice.com
/vertical/Sites/{39D93924-66F7-4895-89B2-CF36165444EF}/uploads/{14DE6184-7F42-486BB7EF-E4E025A7036F}.PDF
Greeson, C.J., LeRoy, B.S., & Veach, P.M. (2001, October). A Qualitative
Investigation of Somali Immigrant Perceptions of Disability: Implications for
Genetic Counseling. Journal of Genetic Counseling, 10(5), 359-378.
Hampel, H., Grubs, R.E., Walton, C.S., Nguyen, E., Breidenbach, D.H., Nettles, S., et al. (2009).
Genetic Counseling Practice Analysis. Journal of Genetic Counseling, 18(3), 205-216.
Kobylarz, F.A., Heath, J.M., & Like, R.C. (2002). The ETHNIC(S) Mnemonic: A clinical tool
for ethnogeriatric education. Journal of the American Geriatrics Society, 50(9), 1582-1589.
Lewis, T. (1996, August). Somalia Cultural Profile. Retrieved November 5, 2009, from
http://ethnomed.org/culture/somali/somali-cultural-profile
Mercer, E. (2004, March/April). Field Notes: Social Adjustment and Mental Health of Refugees.
Refugee Reports, 25(2), 12-14.
Minnesota Immigrant Health Task Force. (2005, January). Immigrant Health: A Call to Action.
Retrieved from http://www.health.state.mn.us/divs/idepc/refugee/topics/immhealthrpt.pdf
Noor, M.C. & Putman, D.B. (1993). The Somalis: Their History and Culture. Retrieved November 5, 2009,
from http://www.cal.org/co/somali/index.html
Prendes-Lintel, M. (2001). A Working Model in Counseling Recent Refugees. In J.G.
Ponterotto, J.M, Casas, L.A. Suzuki & C.M. Alexander. (Eds.), Handbook of
Multicultural Counseling (2nd Ed.) (p. 729-752). Thousand Oaks, CA: Sage Publications.
Runyon, M. (2010). Personal communication, January 6.
Saadallah, A.A. & Rashed, M.S. (2007). Newborn Screening in the Middle East and North Africa. Journal
of Inherited Metabolic Disease, 30(4), 482-489.
Schuchman, D.M. (n.d.). Somali Children and Families. Retrieved from
http://www.macmh.org/programs_services/education/conference/09conf/HOs/9DSchuchman.So
maliCh&Fam.pdf
Schuchman, D.M. & McDonald, C. (2004). Somali Mental Health. Bildhaan: An International
Journal of Somali Studies, 4(8), 65-77.
The UN Refugee Agency. (2007, December). Who We Help. Retrieved November 5, 2009, from
http://www.unhcr.org/pages/49c3646c11c.html
The UN Refugee Agency. (2009, June). 2008 Global Trends: Refugees, Asylum-seekers,
Returnees, Internally Displaced and Stateless Persons. Retrieved November 5, 2009, from
http://www.unhcr.org/4a375c426.html
United Nations. (1951). Convention and Protocol Relating to the Status of Refugees. New York:
United Nations Publications.
United States Department of State: Bureau of Population, Refugees, and Migration. (2008, June).
FY 2009 Reception and Replacement Program. Retrieved November 5, 2009, from
http://www.state.gov/g/prm/
United States Department of State: Bureau of Population, Refugees, and Migration. (2008,
September). 2009 Cultural Orientation Technical Assistance Program. Retrieved November 5,
2009, from http://www.state.gov/g/prm/109212.htm
U.S. Committee for Refugees and Immigrants. (2009). How Refugees Come to America.
Retrieved November 5, 2009, from http://refugeesusa.org/article.aspx?id=1082&subm=40&
ssm=47&area=About%20Refugees
U.S. Department of Homeland Security: Office of Immigration Statistics. (2009, June). Yearbook
of Immigration Statistics: Refugees and Asylees: 2008. Retrieved from
http://www.dhs.gov/xlibrary/assets/statistics/publications/ois_rfa_fr_2008.pdf
Vichinsky, E & Schlis, K. (2006). Sickle Cell Disease. Retrieved November 5, 2009, from
http://www.genetests.org
Virginia Department of Health: Refugee and Immigrant Health Program. (2004). Newcomer
Health Program Manual. Retrieved November 5, 2009, from
http://www.vdh.virginia.gov/epidemiology/DiseasePrevention/Programs/NewcomerHealth/polform
s.htm
Resources
Refugees
http://www.refugees.org
The US Committee for Refugees and Immigrants works for the needs of refugees by advancing public
policy and aiding in receipt of professional services. The USCRI helps refugees who are fleeing war find
immediate safety and refugees who are searching for a permanent home, helps refugee children who
may have been separate from their family, and works to resettle families into the US. Their website
outlines their initiatives and resettlement programs, results from the Refugee World Surveys, and how to
get involved.
http://www.refintl.org
Refugees International works for assistance and protection for all refugees. Their website describes their
policy recommendations, current projects and past successes, and outlines ways to get involved with
their cause.
http://www.unhcr.org
The United Nations High Commissioner for Refugees works in Africa, Asia and the Pacifics, the
Americas, Europe, Middle East and North Africa to help refugees, internally displaced persons, stateless
persons, asylum-seekers, children, elderly, people with disabilities, women, and returnees find safety and
peace. Their roles range from advocacy to fundraising to protection to asylum and migration. The UNHCR
website provides definitions of the various groups they serve and explanations for the work they do for
those groups. They also offer links to resources including maps, statistics, current research, publications,
archives and more.
http://www.youtube.com/watch?v=xZYI0_gU-o8.
“Passport Health Plan, a Medicaid managed care plan headquartered in Louisville, Kentucky, produced a
video in 2007 that chronicles the lives and stories of former refugees who now serve as medical
interpreters. Through interviews, each of the subjects discusses their personal journey to America, their
struggle to assimilate to a new culture, and along the way, dispel a number of common stereotypes. This
video is a great tool for both staff and professional training when discussing refugees, why they come to
the United States, and the contributions they make to an increasingly diverse America” (Lucy Ricketts,
Producer, personal communication, 07/22/09). A copy of this video, “They Bring the World”, along with a
Viewer’s Guide can be obtained by emailing Lucy Ricketts at [email protected].
Addressing Refugee Health Disparities
PowerPoint Presentation
This PowerPoint discusses adverse health risks in refugee populations, the scope of disparities, and
health issues related to return and repatriation. It was created by Dr. Brian Gushulak of Migration Health
Consultants, Inc. http://www.migrationhealth.com
Multilingual Resources
http://www.brycs.org
The Bridging Refugee Youth and Children’s Services website offers resources for Educators, Parents,
Practitioners, Program Managers, Researchers, and Policy Makers regarding health education, literacy,
multilingual pamphlets, program development, public policy and more.
http://www.cal.org/co/publications/welcome.html
Welcome to the United States: A Guidebook for Refugees is provided to refugees being resettled in the
United States. It offers information about what to expect in the U.S. and the services that are available to
them. The guide helps to create realistic expectations regarding health care, education, and employment
in the United States. It is available in 10 different languages.
http://www.healthinfotranslations.com/somali.php
This website offers quality translations of medical information in multiple languages.
http://www.nlm.nih.gov/medlineplus/languages/languages.html
Medline Plus offers translations of health information in over 45 languages.
http://www.childrensmn.org/Communities/FamiliesAndPatients.asp
The Children’s Hospitals and Clinics of Minnesota offer Patient/Family Education materials detailing
conditions, procedures, first aid and more. These materials are offered in Somali, Spanish, and Hmong.
Somalis
http://www.mainehospicecouncil.org/diversity/SomaliCultureClue4_05.pdf
The University of Washington Medical Center provides Culture Clues on Communicating with Your
Somali Patient. This article discusses how the Somali culture deals with illness, how medical decisions
are made, and the Somali culture’s norms about touch.
http://www.mihv.org/
The Minnesota International Health Volunteers provide a Center for Somali Health division. The program
includes research services, community health outreach, education and training services, and health
education resources for Somali people. They offer free health education videos, reference guides,
booklets and fact sheets for providers and patients.
PowerPoint Presentation
This PowerPoint presentation discusses the Somali population in Columbus, Ohio. It was created by the
Students for Community Cultural Awareness (SCCA), a club at Ohio State University. To learn more
about this organization visit http://www.geocities.com/s4cca.
http://medicalcenter.osu.edu/patientcare/interpreter_services/Pages/index.aspx
The Ohio State University Medical Center Interpreter Services office offers many patient education
materials for Somalis. This website also offers multilingual resources in other languages.
http://www.childrensmn.org/Communities/CrossCultural/Somali.asp
This video is a short presentation and open forum at Children’s Hospital in Minnesota led by two Somali
interpreters. They discuss Somalia and its culture, as well as the reasons Somalis have come to the
United States in large numbers in recent years. They also talk about cultural conflicts in the health care
system and how to avoid such situations.
http://www.somalifamily.org/SCBOContacts.htm
This website provides an interactive map that allows you to locate a Somali community center in your
state.
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_0784
09
Ramadan Health Guide, produced by Communities in Action, London, 2007.
Click on the pdf link on this webpage to learn more about Ramadan and maintaining good health.
Cultural Immersion Activities
http://www.theirc.org
The International Rescue Committee welcomes individuals to spend as much time as they want helping
refugees with resume writing, finding a job, learning English, and with simple activities of daily living.
International Rescue Committee, 122 East 42nd Street, New York, NY 10168 USA. Phone: (212) 5513000.
http://www.unrefugees.org/site/c.lfIQKSOwFqG/b.5106135/k.B3C4/World_Refugee_Day.htm
Each year the United Nations Refugee Agency celebrates World Refugee Day in order to keep the public
aware of the refugees’ situation. Their website offers information about the national celebration as well as
how to host a celebration in your city.
http://www.somalifamily.org/SCBOContacts.htm
Visit a Somali Community Center in your area. Take part in events or meetings.
http://www.refugees.org/article.aspx?id=1093
The U.S. Committee for Refugees and Immigrants offers information on ways to donate your time and
expertise to help refugees and immigrants in the United States. Contact information for organizations in
your community is available. At various centers you can volunteer to become a youth mentor or
community liaison, teach computer skills and job training, or house a refugee while a permanent
residence is found.
The Kite Runner - Read the novel (or watch the movie): by Khaled Hosseini (2003), Riverhead Books.
The book was adapted into a film in 2007. The Kite Runner tells the story of Amir a young boy from the
Kabul Afghanistan, who betrayed his best friend Hassan, the son of his father's servant. The story is set
against a backdrop of tumultuous events, from the fall of the monarchy in the country through the Soviet
invasion, the rise of the Taliban, the mass exodus of refugees to the U.S. and life after resettlement.
Sickle Cell Disease
http://www.sicklecellinfo.net
This website is designed to offer education to the public about sickle cell disease. It provides basic
information and describes current research on the disease.
http://www.ascaa.org
The American Sickle Cell Anemia Association offers diagnostic testing, evaluation, counseling and
supportive services to individuals and families at risk for Sickle Cell Disease. Their website allows
discussion with other families, provides educational materials, supplies information about support groups
and events in the United States, as well as listing current research studies and recent publications for
public viewing.
http://www.madisonsfoundation.org/
Madison’s Foundation works to improve the amount and quality of information available to parents of
children with life-threatening diseases. Their website offers communication pathways among parents,
physicians, and other providers.
http://ghr.nlm.nih.gov/condition=sicklecelldisease
National Library of Medicine Genetics Home Reference answers the most frequently asked questions
about sickle cell disease and provides numerous resources to find additional information.
http://www.sicklecelldisease.org
The Sickle Cell Disease Association of America advocates for the quality of life and services for
individuals affected by sickle cell disease. Their website offers information about the disease, sickle cell
disease organizations in your area, educational opportunities, information about current research, and
links to various resources.
Assessment and Evaluation Questions
Discussing Diagnosis and Natural History: Genetic Counseling Somali Refugees
1. True/False
The United States accepts refugees on one of the following three conditions: they have a history of
persecution, they are of “special humanitarian concern,” or they are related to a refugee currently in
the U.S.
2. True/False
Overseas medical screening resulting in the finding of HIV/AIDS, tuberculosis, Hansen’s disease
and others may prevent a person from entering the United States as a refugee.
3. True/False
According to Somali beliefs, an illness may be caused by God, evil spirits, or behavior of oneself or
others.
4. True/False
A child born in Somalia is likely to have had newborn screening for hemoglobinopathies.
5. True/False
The ETHNIC mnemonic device helps healthcare providers understand how a patient’s culture will
affect his/her treatment.
6. True/False
Most refugees to the U.S. are offered resettlement.
For questions 7-10, please read “A Qualitative Investigation of Somali Immigrant Perceptions of Disability:
Implications for Genetic Counseling” from the Journal of Genetic Counseling.
7. True/False
Having a child with a disability would change a Somali couple’s plans for future children.
8. True/False
Because Somali families take on the responsibilities of caring for a family member with a disability,
they may be offended if a counselor suggests an alternative home.
9. True/False
Traditional risk/inheritance counseling is not acceptable for Somali patients because they believe
Allah causes a disability or genetic condition, not heredity.
10. True/False
Prenatal genetic testing is accepted by Somali populations; however, the options of what to do with
a positive result are limited.
The following questions are for CEU learners only:
11. I feel I have achieved the following objective as a result of this learning activity:
Summarize the challenges faced by refugees prior to and after arriving in the U.S.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
12. I feel I have achieved the following objective as a result of this learning activity:
List the characteristics of health care provision that convey respect for Somali culture.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
13. I feel I have achieved the following objective as a result of this learning activity:
Apply the mnemonic device, ETHNIC, to understand how culture may affect a patient’s treatment.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
14. Please rate the overall effectiveness of this case in promoting learning.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
15. Please rate the overall quality of this case.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
16. The content of this case was presented without bias of any commercial drug or product.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
17. The technology used was appropriate and effective.
4= Great extent 3= Moderate extent 2= Slight extent 1= Not at all
Disclaimer
The purpose of the Genetic Counseling Cultural Competence Toolkit (GCCCT) is to improve the delivery
of culturally responsive, client-centered genetic counseling to diverse populations and to reduce health
disparities. The GCCCT is an educational resource; any suggestions do not define the standards of
clinical or educational practice. All cases and scenarios are hypothetical. The JEMF, NSGC and Nancy
Steinberg Warren, MS, CGC will not be liable for any medical or psychosocial applications connected with
the use of or reliance upon any information obtained from this website or associated links and resources.
________________________________________________________
This work has been supported by the Jane Engelberg Memorial Fellowship, the 2009 grant from the
Engelberg Foundation to the National Society of Genetic Counselors, Inc.
© 2010 Nancy Steinberg Warren, MS, CGC, all rights reserved.