Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
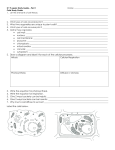
n Feature Article Anatomy and Histology of the Transverse Humeral Ligament Brian J. Snow, MD; Steven J. Narvy, MD; Reza Omid, MD; Roscoe D. Atkinson, MD†; C. Thomas Vangsness Jr, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20130920-23 The classic literature describes the transverse humeral ligament (THL) as a distinct anatomic structure with a role in biceps tendon stability; however, recent literature suggests that it is not a distinct anatomic structure. The purpose of this study was to evaluate the gross and microscopic anatomy of the THL, including a specific investigation of the histology of this ligament. Thirty frozen, embalmed cadaveric specimens were dissected to determine the gross anatomy of the THL. Seven specimens were evaluated histologically for the presence of mechanoreceptors and free nerve endings. Two tissue layers were identified in the area described as the THL. In the deep layer, fibers of the subscapularis tendon were found to span the bicipital groove with contributions from the coracohumeral ligament and the supraspinatus tendon. Superficial to this layer was a fibrous fascial covering consisting of distinct bands of tissue. Neurohistology staining revealed the presence of free nerve endings but no mechanoreceptors. This study’s findings demonstrate that the THL is a distinct structure continuous with the rotator cuff tendons and the coracohumeral ligament. The finding of free nerve endings in the THL suggests a potential role as a shoulder pain generator. Figure: Photograph of dissection showing the transverse humeral ligament spanning the intertubercular groove. The superficial layer in distinct bundles is visible. The authors are from the Department of Orthopaedic Surgery (BJS, SJN, RO, CTV) and the Department of Pathology (RDA), Keck School of Medicine, University of Southern California, Los Angeles, California. The authors have no relevant financial relationships to disclose. †Deceased. Correspondence should be addressed to: C. Thomas Vangsness Jr, MD, Department of Orthopaedic Surgery, Keck School of Medicine, University of Southern California, 1520 San Pablo St, #2000, Los Angeles, CA 90089 ([email protected]). doi: 10.3928/01477447-20130920-23 OCTOBER 2013 | Volume 36 • Number 10 e1295 n Feature Article T he rotator interval of the shoulder is a triangular space in the shoulder capsule bordered by the base of the coracoid medially, the anterior margin of the supraspinatus tendon superiorly, the superior border of the subscapularis tendon inferiorly, and the transverse ligament laterally. Aspects of the interval region have been the topic of controversy in the literature in both anatomic and functional aspects.1-8 The transverse humeral ligament (THL) was first described in 1889 by Brodie9 as a broad band of trapezoidal fibrous tissue between the greater and lesser tuberosities of the humerus. It has been described in similar fashion by other early works, including in Anatomy: Descriptive and Surgical by Gray10 and Applied Anatomy by Davis.11 Its described function was to help retain the long head of the biceps tendon within the intertubercular groove as it emerges from beneath the coracohumeral ligament. Although the insertional anatomy and function of the rotator cuff have been studied extensively, little attention has been given to the THL. Few precise anatomic or functional descriptions of the THL exist, and no consensus has been reached regarding its lateral insertion and exact structure.6,12-17 Magnetic resonance imaging evidence suggests that the structure classically described as the THL may be a direct continuation of the tendon of the subscapularis.18 The purposes of this study were to provide an accurate anatomic description of the THL and to define the neural structures it contains. Materials and Methods Thirty frozen, embalmed cadaver shoulders of uncertain age were dissected under loupe magnification. The skin and subcutaneous tissue were removed. The deltoid muscle was sharply released from its origins and reflected distally. The short head of the biceps and the pectoralis major muscles were also released and e1296 reflected. Blunt dissection was used to reach the long head of the biceps tendon on the surface of the humerus and free it below the level where the THL has been described. The superior and inferior borders of the fibrous tissue overlying the intertubercular groove were then demarcated, and all connective and adipose tissue were removed to aid in visualization. The origin, insertion, and nature of the fibers composing the ligament were defined and described. A standard caliper was then used to measure the height and width of the ligament. Seven specimens were subsequently removed, frozen, and sectioned with a 25-µm-wide sliding microtome, which produced 240 continuous tissue sections mounted on 100 slides per specimen. A modified Zimny gold chloride technique consisting of 90% formic acid, 1% aqueous gold chloride, and lemon juice was then used to identify the neural tissue within each section.19 The slides were reviewed by a single neuropathologist (R.D.A.). 1 Figure 1: Photograph of dissection showing the transverse humeral ligament spanning the intertubercular groove. The superficial layer in distinct bundles is visible. Results The anatomic region described as the THL consisted of 2 layers of tissue: a thin, superficial layer consisting of fibers in distinct bundles and a deeper layer of fibrous tissue spanning the intertubercular groove (Figure 1). Proximally, this deep layer was a continuance of fibers from the rotator cuff tendons and the coracohumeral ligament. Fibers of the subscapularis continued from the superomedial side, whereas the supraspinatus tendon contributed fibers laterally. The coracohumeral ligament fibers blended with the rotator cuff tendons at the proximal superior edge of the groove. Distally, the fibers of the subscapularis muscle were predominant. Average width of the bicipital groove was 10 mm. The tissue spanning the groove averaged 14 mm wide and 14 mm high. Histologic staining revealed flat sheets of collagen consisting of dense regular connective tissue centrally and dense irregular connective tissue at the periphery near 2 Figure 2: Photograph showing an unmyelinated free nerve ending (arrow) in the periphery of the ligament near the greater tuberosity. the humeral tuberosities. No mechanoreceptors were noted after the modified gold chloride stain was applied. Free nerve endings were noted in both tissue layers, particularly in the areas of dense irregular connective tissue (Figure 2). Both myelinated and unmyelinated nerves were present in all specimens examined. Discussion Much anatomic variation exists within the rotator interval, and the literature is ORTHOPEDICS | Healio.com/Orthopedics Transverse Humeral Ligament | Snow et al controversial regarding the existence of the THL as a discrete anatomic structure traversing the intertubercular groove. Gleason et al20 performed anatomic, magnetic resonance imaging, and histology studies on 7 matched pairs of freshfrozen cadaveric shoulders. Two layers of distinct tissue were noted, as were observed in the current study, but the authors determined that the fibers covering the intertubercular groove were composed of a sling formed mainly by fibers of the subscapularis, with contributions from the supraspinatus tendon and coracohumeral ligament. No separate ligamentous structure, consistent with the described THL, was identified traversing the bicipital groove.20 MacDonald et al21 performed a similar dissection study involving 85 embalmed cadaver shoulders. In all specimens, a fibrous expansion was found arising from the posterior lamina of the tendon of the pectoralis major; however, a discrete THL could not be identified within this fibrous tissue in any specimen. Significant variation in the insertion of the subscapularis was again noted, leading the authors to conclude that the structure overlying the intertubercular groove consists of tendinous fibers of subscapularis rather than a separate THL.21 Regarding the neural anatomy of the shoulder, Soifer et al22 evaluated the neural elements within the subacromial space in 14 cadaveric shoulders. Neurofilaments and peripheral nerves were identified within the subacromial bursa, rotator cuff tendon, biceps tendon and tendon sheath, and THL; a significantly richer supply of free nerve fibers was found in the bursa compared with other tissues. Previously, Vangsness et al23 studied the sensory innervations of the superior, middle, and inferior glenohumeral ligaments in 8 fresh, unembalmed cadavers and found that the ligaments contained proprioceptive mechanoreceptors, such as Ruffini and Pacinian corpuscles, as well as free nerve endings. These OCTOBER 2013 | Volume 36 • Number 10 results were compared with the current study’s finding of only free nerve endings of the THL. The current study is an anatomic descriptive basic science study that adds to the body of evidence about the true nature of the THL. Prior work has cast doubt on the existence of the THL, instead describing contributions of the subscapularis tendon across the intertubercular groove. In a magnetic resonance imaging study of 58 shoulders, Cash et al18 noted significant variability in this region and found a discrete THL in only 36% of specimens. The current study identifies a distinct structure with contributions from the rotator cuff and the coracohumeral ligament to the THL. The reasons for these contrasting findings are unclear; however, the smaller sample size in the current study is a significant limitation given the extensive variability within this anatomic region. The THL identified in the current study lacks the pressure and proprioceptive mechanoreceptors that are present in other stabilizing shoulder structures, such as the superior, middle, inferior, and posterior glenohumeral ligaments. However, the presence of myelinated and unmyelinated free nerve endings suggests a potential role of the THL as a pain generator in the clinical situations of impingement, biceps tendonitis, hypertrophy or subluxation, rotator cuff tears or tendonitis, and rotator interval lesions. Further study of the anatomy of the rotator interval using a larger number of study specimens could provide more conclusive data regarding the existence and clinical relevance of the THL. References 1. Bennett WF. Visualization of the anatomy of the rotator interval and bicipital sheath. Arthroscopy. 2001; 17(1):107-111. 2. Bennett WF. Subscapularis, medial, and lateral head coracohumeral ligament insertion anatomy: Arthroscopic appearance and incidence of “hidden” rotator interval lesions. Arthroscopy. 2001; 17(2):173-180. 3. Boardman ND, Debski RE, Warner JJ, et al. Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg. 1996; 5(4):249-254. 4. Burkart AC, Debski RE. Anatomy and function of the glenohumeral ligaments in anterior shoulder instability. Clin Orthop Relat Res. 2002; (400):32-39. 5. Cole BJ, Rodeo SA, O’Brien SJ, et al. The anatomy and histology of the rotator interval capsule of the shoulder. Clin Orthop Relat Res. 2001; (390):129-137. 6. Cooper DE, O’Brien SJ, Arnoczky SP, Warren RF. The structure and function of the coracohumeral ligament: an anatomic and microscopic study. J Shoulder Elbow Surg. 1993; 2(2):70-77. 7. Edelson JG, Taitz C, Grishkan A. The coracohumeral ligament. Anatomy of a substantial but neglected structure. J Bone Joint Surg Br. 1991; 73(1):150-153. 8. Neer CS II, Satterlee CC, Dalsey RM, Flatow EL. The anatomy and potential effects of contracture of the coracohumeral ligament. Clin Orthop Relat Res. 1992; (280):182-185. 9. Brodie CG. Note on the transverse-humeral, coraco-acromial, and coraco-humeral ligaments. J Anat Physiol. 1890; 24:247-252. 10. Gray H. Anatomy: Descriptive and Surgical. New York: Lea Brothers & Co; 1901. 11. Davis GG. Applied Anatomy. Philadelphia, PA: J.B. Lippincott Co; 1910. 12.Clark JM, Harryman DT. Tendons, liga ments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am. 1992; 74(5):713-725. 13. Clark JM, Sidles JA, Matsen FA. The relationship of the glenohumeral joint capsule to the rotator cuff. Clin Orthop Relat Res. 1990; (254):29-34. 14. Jost B, Koch PP, Gerber CH. Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg. 2000; 9(4):336-341. 15.Sethi N, Wright R, Yamaguchi K. Disor ders of the long head of the biceps tendon. J Shoulder Elbow Surg. 1999; 8(6):644-654. 16. Weishaupt D, Zanetti M, Tanner A, Gerber C, Hodler J. Lesions of the reflection pulley of the long biceps tendon: MR arthrographic findings. Invest Radiol. 1999; 34(7):463469. 17. Werner A, Mueller T, Boehm D, Gohlke F. The stabilizing sling for the long head of the biceps tendon on the rotator cuff interval. Am J Sports Med. 2000; 28(1):28-31. 18. Cash CJ, MacDonald KJ, Dixon AK, Bearcroft PW, Constant CR. Variations in the MRI appearance of the insertion of the tendon of subscapularis. Clin Anat. 2009; 22(4):489494. 19. Zimny M, St. Onge M, Schutte M. A modified gold chloride method for the demonstra- e1297 n Feature Article tion of nerve endings in frozen sections. Stain Technol. 1985;60(5):305-6. 20. Gleason PD, Beall DP, Sanders TG, et al. The transverse humeral ligament: A separate anatomic structure or a continuation of the osseous attachment of the rotator cuff? Am J e1298 Sports Med. 2006; 34(1):72-77. 21. MacDonald K, Bridger J, Cash C, Parkin I. Transverse humeral ligament: does it exist? Clin Anat. 2007; 20(6):663-667. 22. Soifer T, Levy H, Miller-Soifer F, Kleinbart F, Vigorita V, Bryk E. Neurohistology of the subacromial space. Arthroscopy. 1996; 12(2):182-186. 23. Vangsness CT, Ennis M, Taylor JG, Atkinson R. Neural anatomy of the glenohumeral ligaments, labrum, and subacromial bursa. Arthroscopy. 1995; 11(2):180-184. ORTHOPEDICS | Healio.com/Orthopedics