Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
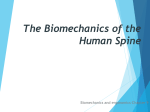
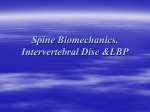
ANATOMY OF THE LUMBAR SPINE Lumbar Vertebra The lumbar spine consists of five lumbar vertebrae, five corresponding intervertebral discs, twelve zygapophyseal joints (T12-L1 to L5-S1), and multiple ligaments, muscular, and neurological contributions (Table 10.1). The design of the lumbar spine allows viscoelastic motion, absorbs energy, moves with six degrees of freedom, and has limited fatigue tolerance. These functions depend on muscular, bone, and ligamentous components for mechanical tasks (1). Table 10.1: General Information Regarding the Lumbar Spine Region. Concept Information Bones Number of dedicated joints Range of motion Five primary bones of the lumbar spine 18 joints, 6 intervertebral, and 12 zygapophyseal Theoretical resting Position Theoretical close-pack Position Theoretical capsular pattern Resting position = mid-way between flexion and extension Lumbar spine range of motion • Flexion = 50° • Extension = 15° • Rotation = 5° • Lateral flexion = 20° Close-pack position = extension Capsular pattern = side bend and rotation equally limited, extension The typical lumbar vertebrae display dramatic height increases when compared to the thoracic spine. The lower vertebrae and discs are wedge shaped, lending to the natural postural lordosis. The anterior aspect of the vertebrae is generally concave and the posterior aspects are flattened and stable (1). Lumbar vertebrae can be divided into three sections from anterior to posterior. The anterior portion of the vertebral body is essentially flat on the superior and inferior surfaces and provides contact points for the intervertebral disc (1). The middle section in the lumbar spine includes the pedicles, which are strong posterior projections. The posterior portion of the vertebral body includes the inferior and superior articular processes, the spinous processes, and the transverse processes. The spinous processes are heavy and rectangular. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ The Vertebral and Intervertebral Foramen The anterior wall of the vertebral canal is flattened, and the discs demonstrate no propensity of bulging into the spinal canal. The anterior wall of the vertebral canal is formed by the posterior surfaces of the lumbar vertebrae, and the posterior wall is formed by the lamina and ligamentum flava of the same vertebrae (1). The disc surrounds the intervertebral foramen anteriorly, the pedicle inferiorly and superiorly, and the zygapophyseal joints posteriorly (1). Figure 10.1: The Intervertebral Foramen Table 10.2: Joints of the Lumbar Spine. Joint Information Intervertebral disc • • Zygapophyseal (facet) joints • The intervertebral disc (IVD) connects the bodies of adjacent vertebrae together. It is classified as a symphysis or amphiarthrosis 3 components: 1) Annulus: collagen makes up 50–70% of its weight. Fibers are arranged in concentric rings around the nucleus. These concentric sheaths are called lamellae. They are orientated at an angle of 65–70° from the vertica,l with adjacent layers running in opposite 65° orientations from the vertical (i.e., they criss-cross). The outer portion of the annulus is the only innervated portion of the disc. 2) nucleus: comprises the central portion of the disc. There is no clear boundary between the nucleus and the annulus. The nucleus is 70–90% water. 3) vertebral end plate: is 0.6–1 mm thick The facets are oval in shape, are slightly curved or biplanar, and are oriented parallel to the frontal plane. The facet orientation angle changes with respect to the mid-sagittal plane (Bogduk): Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ • o L1–2 = 15° o L2–3 = 30° o L3–S1 = 45° Zygapophyseal joints take ~20% of the spinal weight-bearing load. With flexion, you increase the weight bearing on the disc and decrease the weight bearing on the facet joints The Zygapophyseal Joints The zygapophyseal joints, also known as facets or apophysial joints, are enclosed in a fibrous capsule that contains menisci. The menisci are invaginations of the joint capsule and may occasionally project into joint space (2). Facets do not have “free” motion as does the disc and are limited both structurally and by the capsule. Movement is generally restricted to large sagittal motions guided by the shape of the zygapophyseal joints. The facets flatten anteroposterior and run slightly dorsally and upward (1). The zygapophyseal joints and the surrounding structure represent attachment sites for several intertransverse ligaments and muscles. The intertransverse ligaments attach to each transverse process and limit side flexion to the opposite side. The transverse process of L5 attaches to the medial portion of the iliac crest by several strong strands of the iliolumbar ligament, which tends to ossify at older ages. The anterior portions of the lumbar facets orient coronally (promote side-bend forces). The posterior facets face sagittal and resist rotation and side-bend forces (2). Figure 10.2: Zygapophyseal Joints of the Lumbar Spine Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ The Intervertebral Disc (Interbody Joints) The intervertebral disc functions as a shock absorber and a deformable space, and resists compressive forces of the spine. There are three major components of the disc; 1) the annulus fibrosis, 2) the nucleus pulposis and 3) the cartilaginous end plate. The nucleus pulposis accounts for up to 50 percent of the disc area and includes collagen fibers without specific orientation. The major constituents include proteoglycans, collagen, and water. The nucleus is responsible for nutrient transport via osmosis of the middle cartilaginous end plate and articulation with the disc. The actual compression tolerance is derived from the properties in the water (at lower levels) through proteoglycans imbibitions of joint fluid. The nucleus transfers much of the weight to the annulus when loads are high or when damage has occurred to the intervertebral segment. The annulus gradually blends into the nucleus in a gradual transition rather than an abrupt transition between two separate structures (3). The annulus consists of multiple concentric rings called lamellae, which provide tension in all directions when force is encountered. The lamellae consist of concentric-oriented rings, lying at a 30-degree plane from the horizon (4). Lamellae are designed to counter compression, side bending, shear, and distraction forces. Nerve endings in the outer border of the annulus are responsible for pain generation and somatic referral of symptoms. The disc integrates with the vertebrae at the cartilaginous end plate. The inner twothirds of the disc attach to the cartilaginous end plate, while the outer two-thirds attach to the intervertebral body. The cartilaginous end plate is responsible for nutrient transfer to the disc from the vertebral body and becomes thicker and less permeable with increasing age. This structure is composed of hyaline cartilage and is thicker and more calcified at the periphery (5). The vertebral end plate also contributes in confining the annulus and nucleus (6). The intervertebral disc is the major load-bearing and motion control element in lateral and anterior shear, axial compression, flexion, and side flexion. The intervertebral disc guides the motion of rotation, while the facet restricts motion beyond disc boundaries (7,8). This is in contrast to the facet, which contributes to motion control during posterior shear, extension, and axial torsion. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ During lateral and anterior shear with high external forces, the facets may transmit a portion of the load (8). In a healthy lumbar spine, the disc evenly transmits forces to the ligaments of the back (specifically, the anterior longitudinal ligament and the posterior longitudinal ligament), through an interplay of the thoracolumbar fascia and abdominal musculature (8,9). In the nondamaged disc, up to 85 percent of the movement is controlled through the interplay of disc dispensation. A damaged disc will encounter a different percentage, typically dispensing force to the facets and other supportive structures including the vertebral end plate. The vertebral end plate is the most significant potential point of weakness and is the quickest healing area of the lumbar disc segment (1). Unfortunately, no known clinical examination features outline vertebral end plate damage; thus, these impairments may remain undetected. Nerves of the Lumbar Spine The spinal nerves of the lumbar spine subdivide into ventral and dorsal rami. Each spinal nerve lies within the intervertebral foramen and is numbered according to the vertebra above the nerve. Subsequently, the L4 nerve root runs below the L4 vertebra, in between L4 and L5. Each spinal nerve arises from a ventral and a dorsal nerve root, which meet to form the spinal nerve in the intervertebral foramen (1). Each dorsal root communicates to a dorsal root ganglion that contains the cell bodies of the sensory fibers of the dorsal roots. The dorsal root transmits sensory fibers, while the ventral root primarily transmits motor fibers (10). Each spinal nerve exits the intervertebral foramen with dural structures, an extension of the dura mater and arachnoid mater, commonly referred to as the dural sleeve (10). In the intervertebral foramen, the amount of space is extremely limited; thus, the structures in this region are predisposed to problems associated with space-occupying lesions. Branching from each ventral rami are sinuvertebral nerves that are considered mixed (motor and sensory) nerves. The sinuvertebral nerve complex innervates the posterior longitudinal ligament and the outer border of the annulus, and contributes fibers to the joint capsule and articular facet. Posteriorly, the lumbar spine is innervated by branches of the dorsal rami that run to Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ the zygapophyseal joints and muscles. Anterior and posterior plexuses innervate the anterior longitudinal ligament (ALL) and posterior longitudinal ligament (PLL), additionally supplying innervation to the intervertebral disc and periosteum of the vertebral bodies (1,10). This complex innervation pattern reduces the likelihood of unambiguous pain-referral patterns from one specific structure (Table 10.3). Table 10.3: Nerve Root Muscular Innervation of the Lumbar Spine. Nerve Root L1-L2 Test Action Hip flexion L3 Knee extension L4 Ankle dorsiflexion L5 Toe extension S1 S2 Ankle DF, eversion, hip extension, knee flexion Knee flexion S3 --- Muscles Psoas, iliacus, sartorius, gracilis, pectineus, adductor longus, and adductor brevis Quads, adductor longus, adductor magnus, and adductor brevis Tibialis anterior, quadriceps, tensor fascia latae, adductor magnus, obturator externus, and tibialis posterior Extensor hallucis longus, extensor digitorum longus, glut medius and minimus, obturator internus, semimemb and semitend, peroneus tertius, and popliteus Gastroc and soleus, glut maximus, obturator internus, piriformis, biceps femoris, semitendinosis, popliteus, peroneus longus and brevis, and extensor digitorum brevis Biceps femoris, piriformis, soleus, gastroc, flexor digitorum longus, flexor hallucis longus, and intrinsic foot muscles Intrinsic foot muscles (except abductor hallucis), flexor hallucis longus, flexor digitorum brevis, and extensor digitorum brevis Ligaments of the Lumbar Spine Numerous ligaments restrain free motion (Table 10.4). The anterior longitudinal ligament (ALL) and posterior longitudinal ligament (PLL) interconnect the vertebral bodies and are deeply associated with the annulus fibrosis of the discs. The ALL serves primarily to resist vertical separation of the anterior ends of the vertebral bodies and resists anterior bowing during extension movements (1). The PLL also resists separation of vertebrae and aids in posterior support with the intimate connection with the annulus fibrosis (1). Posterior ligaments include the ligamentum flavum, the interspinous ligaments, and the supraspinous ligament. The ligamentum flavum is a short, thick ligament that joins each lamina of consecutive vertebrae. This ligament also resists separation of vertebrae, although the exact mechanics of the ligament are unknown (1,5). The interspinous ligaments connect adjacent spinous Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ processes and most likely resist separation of the spinous processes. The supraspinous ligament attaches to the posterior ends of the spinous processes and are likely heavily embedded with proprioceptive nerve endings (11). In general, the posterior spinous ligaments are slack in upright standing but will tighten during forward flexion and rotation. The iliolumbar ligaments are well-developed ligaments, are anterior, superior, and vertical in nature, and are one of few structures that actually cross the sacroiliac joint (12). Bogduk and Twomey (12) outlined five separate bands of the iliolumbar ligament, which traverse from the transverse process of L5 to the quadratus lumborum, the iliac crest, and the posterior aspect of the iliac tuberosity. The iliolumbar ligament ossifies by the fifth decade and is demarcated from the quadratus lumborum muscle (13). The iliolumbar ligament appears to restrict sagittal nutation and counternutation of the sacroiliac (12,14). Table 10.4: Ligaments and Connective Tissue of the Lumbar Spine. Name Location Function Ligament flavum Located between the anterior surfaces of lamina (i.e., is in the canal, posterior aspect). Located between the spinous processes Limits flexion Intertransverse ligament Located between the transverse processes Limits side bending Posterior longitudinal ligament Covers posterior vertebral bodies inside the vertebral canal Stabilizes and limits extension Anterior longitudinal Ligament Covers the anterior vertebral bodies Stabilizes and limits extension Capsule and zygapophyseal joints Surrounds each zygapophyseal joint Supports and stabilizes the facet joints Iliolumbar ligament Located between the L5 transverse process to the sacrum (iliac crest area) Restricts side flexion and stabilizes the lumbopelvic complex Supra- and interspinous ligaments Limits flexion Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ Muscular Stabilization of the Spine Stability of the lumbar spine is a joint responsibility of the passive and active structures of the lumbar spine. Studies have suggested that the multifidi are responsible for postural, multidirectional, and individual segmental control (15–17). The multifidi are the largest and most medial of the lumbar paraspinal muscles, originating from a spinous process and spreading caudolaterally from the mid-line, and inserting into the mamillary processes of the facet joint, the iliac crest, and the sacrum. The multifidi maintain lumbar lordosis by acting like a bowstring transmitting some of the axial compression force to the ALL. These muscles protect discs by preventing unwanted wobbling movements associated with torsion and flexion. The transverse abdominus plays an important role in dynamic isometric stabilization during twisting and rotation motions (18–21). Selected authors have suggested that, for individuals with passive spine instability, sagittal torsion or rotation strains are more responsible for damaging structures than linear forces (22). The hypothesized contribution occurs through increasing the stiffness of lumbar spine (i.e., increasing intra-abdominal pressure and tensioning the thoracolumbar fascia resisting torsion). The transverse abdominus increases in stiffness in anticipation of limb movement and limits intersegmental translation and rotational forces. This action may provide a more stable lever with the other trunk muscles (21). Other contributors to spine movement and stability include the erector spinae, external and internal obliques, and the thoracolumbar fascia. The thoracolumbar fascia that inserts on the gluteus maximus and latissimus dorsi and integrates with the deep lamina of the inferior aspect of the lumbar pedicle works in concert with the lumbar musculature to stabilize during dynamic movement. The internal and external obliques work in concert with the thoracolumbar fascia to stabilize the core pressure but are primarily prime movers of diagonal rotational motions and poor stabilizers of the lumbar spine. The erector spinae consist of the longissimus thoracic and iliocostalis lumborum groups (23). Van Dieën et al. (24) reported that subjects with low back pain demonstrated a higher recruitment of the lumbar erector spinae in an effort to increase stability. The psoas major is not a significant contributor to spine stability and is primarily a hip flexor (23). The psoas fibers originate near the anterior spine (T12 through L4-5) and transverse process Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ and inserts on the hip. This lever mechanism is too inefficient to produce lumbar movement (23). Many clinicians misperceive the role of the psoas as a significant contributor to low back pain. Bogduk states, “The isometric morphology of the psoas indicates that the muscle is designed exclusively to act on the hip” (23). Although a maximum contraction can increase intradiscal loads (23), this muscle may not contribute to stabilize the spine. Summary • • • • Much of low back movement is controlled and guided by the intervertebral disc. The shape of the lumbar vertebral body and disc promotes a natural lordosis. The orientation of the facets limits lumbar rotation and aids in stability during rotation. Several muscles of the lumbar spine are the primary source of dynamic stability, functioning as prime movers and stabilizers. BIOMECHANICS OF THE LUMBAR SPINE The lumbar spine has six degrees of freedom and is generally described by movements associated with flexion, extension, rotation, and side flexion (Table 10.5). Table 10.5: Specific Biomechanics and Movement of the Lumbar Spine Region Flexion Biomechanics and Movement • • • Extension • • • • The lower lumbar segments rotate forward from a backward tilted position (reducing umbar lordosis). The lumbar lordosis typically will only reach the neutral position and rarely achieves a kyphosis. The superior vertebra rotates anteriorly in the sagittal plane on the inferior vertebra, raising the inferior articular process of the superior vertebra upward and slightly backward, and opening a small gap between the superior and inferior articular facets. Anterior sagittal plane translation then occurs (as a result of gravity or muscular contraction), closing this gap. Impaction of the inferior facet against the anteromedial portion of the superior facet restricts anterior sagittal plane translation. Tension of the articular capsule also limits flexion The sacrum nutates the forward nodding movement of the sacrum between the hip bones (innominates) with the sacral base moving anterior and inferior and the sacral apex moving posterior and superior Consists of a posterior sagittal plane rotation combined with a small posterior sagittal plane translation The facet joints have a limited role in restricting extension The ALL and annulus restrict extension along with SP approximation The canal spinal and the intervertebral foramen diameter decrease Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ by up to 20% Side flexion • • Rotation • • The ipsilateral superior facet slides down the adjacent inferior facet, while the contralateral superior facet slides upward in relation to the contralateral inferior facet Can be thought of as unilateral flexion on the contralateral side and unilateral extension on the ipsilateral side Impaction of the contralateral articular facets limit axial extension The joint space is very narrow; therefore, ROM permitted is small Many manual therapy disciplines base specific mobilization and manipulation techniques on selected theories of lumbar coupling direction, theories that are often inconsistently reported (25). Biomechanical analysis including investigation of coupled motion is often reported as an essential concept to low back evaluation (26–30). The two principle components of lumbar coupling are quantity of motion, used in detection of hypo and hypermobility, and direction of coupling behavior. The most controversial of the two assessment methods is the theory of directional lumbar coupling, a theory based on the invalidated premise that a “normal” lumbar coupling pattern exists in nonpathological individuals (31–33). It has been suggested that the link between pathology of the lumbar spine may be best represented by addressing the pattern or direction of coupling behavior (30,34–39). Coupled motion is the rotation or translation of a vertebral body about or along one axis that is consistently associated with the main rotation or translation about another axis (39). During movement, translation occurs when movement is such that all particles in the body at a given time have the same direction of motion relative to a fixed coordinate system (39). With movement, rotation occurs as a spinning or angular displacement of the vertebral body around some axis. Historic, foundational works on coupling mechanics used observation or controversial twodimensional (2-D) radiographic imagery (30). Past 2-D studies involved cadaveric tissue, X-rays of live subjects, or single X-rays of segments, and used a small sample of subjects (30,40). Prior to 1969, only 2-D studies were executed for spinal coupling, signifying that any study performed prior to 1969 encompassed these errant methods (30). 2-D imagery leads to magnification errors, projection of translations as rotations, and misleading results (30,40). Theories such as Fryette’s Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ laws I and II of the lumbar spine have not held up well to modern science and are generally recognized by researchers as incorrect (25,30). Contemporary studies use three-dimensional (3-D) assessment, which more accurately measures the six degrees of freedom associated with coupling motion (25). All of the studies reported no coupling present in at least some of the specimens or subjects at L1-2, with two reported opposite results (25). Inconsistency is also present at L2-3 and L3-4 where results are split between no report of coupling, opposite rotational coupling with side bending, and both (25). The spinal levels of L4-5 and L5-S1 exhibited the greatest degree of variability. Two studies reported that no coupling was present at L4-L5, three others recognized opposite rotational coupling with side bending, and one indicated same-side rotational coupling with side bending (25). The same two studies which found no coupling at previous segments found no coupling at L5-S1, three others found opposite rotational coupling to side bending, and one found both opposite and no coupling (25). Recent in vivo and in vitro studies find coupling pattern disparities specifically when dealing with symptomatic patients with low back pain (27,34,47–50). According to Panjabi et al. (51), “diseases and degeneration affect the physical properties of the spinal components (ligaments, discs, facet joints, and vertebral bodies), which, in turn, alter the overall spinal behavior.” Current research addresses the contribution of coupling motion from the disc and the facets (25). An in vivo study (52) found that a narrowed intervertebral disc led to increased lateral bending, increased disc shear at the level of abnormality, and asymmetric coupling patterns throughout adjacent functional spine units. Lower lumbar levels (L3-4, L4-5) increased their coupling behavior and range while decreasing at higher levels (L1-2, L2-3). Surgical fusion created increased mobility immediately above the fused site (53). The coupling movement was abnormal and relied heavily on increased motion in the posterior facet joints and shear of the intervertebral discs. Posterior-lateral disc removal in vitro does significantly affect normal spinal kinematics. The alteration is not only present in the single functional spinal unit but also the neighboring joints (38). Chronic back pain diagnoses such as postlaminectomy, postdiscectomy, and disc degeneration leads to variability in in vivo coupling at lower levels of the lumbar spine (37). Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ There seems to be little evidence to support that knowledge of lumbar spine coupling characteristics are important in understanding and treating patients with low back pain (29). Many manual therapy techniques use coupling-based mobilizations and the validity of this approach is questionable. Several authors have suggested that the use of symptom reproduction to identify the level of pathology is the only accurate assessment method (54–60). Because no pathological coupling pattern has shown to be consistent, an assessment method in absence of symptom reproduction may yield inaccurate results. Therefore, biomechanical coupling theory may only be useful if assessed with symptom reproduction within a clinical examination (61). There is little evidence to support a limited focus on biomechanical coupling patterns; therefore, techniques that are based on this “theory” are excluded from this textbook. Table 10.6: Serious, Specific Low Back Diseases (70). Category Specific Disorders Examples of Disorders 1) Nonmechanical spine disorders (+ 1%) Neoplasia Metastases, lymphoid tumor, spinal cord tumor Infective spondylitis, epidural abscess, endocarditis, herpes zoster, Lyme disease Ankylosing spondylitis, psoriatic arthritis, reactive arthritis, Reiter’s syndrome, inflammatory bowel disease) Prostatitis, endometriosis, pelvic inflammatory disease Nephrolithiasis, pyelonephritis, renal papillary necrosis Aortic aneurysm Infection Seronegative spondyloarthritides 2) Visceral disease (1–2%) Pelvic Renal Aortic aneurysm Gastrointestinal 3) Miscellaneous Paget’s disease Pancreatitis, cholecystitis, peptic ulcer disease Paget’s disease Parathyroid disease Parathyroid disease Hemoglobinopathies Hemoglobinopathies Range of Motion Troke et al. (62) report global flexion and extension range-of-motion values of 72 degrees to 40 degrees of flexion and 29 degrees to 6 degrees of extension. Their findings suggest that range of motion declines with age changes from 16 to 90 years. These findings are in accordance Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ with others who have reported similar numbers and similar declines with advancing age (63,64). Rotation and side flexion have also been studied extensively. Summary • • • Little to no evidence exists to support the use of directional lumbar coupling biomechanics for manual therapy techniques. The use of coupling assessment as a basis for treatment is neither scientific nor evidence based, and therefore may be inappropriate for certain patients. The majority of segmental range of the motion in the lumbar spine occurs within a sagittal plane, followed by coronal, and lastly, transverse. ONLINE REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. rd Bogduk N. Clinical anatomy of the lumbar spine and sacrum. 3 ed. New York; Churchill Livingstone: 1997. Little JS, Khalsa PS. Material properties of the human lumbar facet joint capsule. J Biomech Eng. 2005;127(1):15–24. Pope MH, Panjabi M. Biomechanical definitions of spinal instability. Spine. 1985;10(3):255–256. Peng B, Wu W, Hou S, Li P, Zhang C, Yang Y. The pathogenesis of discogenic low back pain. J Bone Joint Surg Br. 2005;87(1):62–67. Eyre DR. Biochemistry of the intervertebral disc. Int Rev Connect Tissue Res. 1979;8:227–291. Humzah MD, Soames RW. Human intervertebral disc: structure and function. Anat Rec. 1988;220(4):337–356. Tencer A, Ahmed A, Burke D. Some static mechanical properties of the lumbar intervertebral joint, intact and injured. J Biomech Eng. 1982;104:193–201. Gracovetsky S, Farfan H, Helleur C. The abdominal mechanism. Spine. 1985;10(4):317– 324. O’Sullivan P. Lumbar segmental instability: clinical presentation and specific stabilizing exercise management. Man Ther. 2000;5(1):2–12. Bogduk N. The Innervation of the Lumbar Spine. Spine. 1983;6:286–293. Cavanaugh JM, el-Bohy A, Hardy WN, Getchell TV, Getchell ML, King AI. Sensory innervation of soft tissues of the lumbar spine in the rat. J Orthop Res. 1989;7(3):378– 388. Bogduk N, Twomey L. Clinical anatomy of the lumbar spine. Melbourne; Churchill Livingstone: 1987. Luk K, Ho H, Leong J. The iliolumbar ligament: a study of its anatomy, development and clinical significance. J Bone Jnt Surg. 1986;68:197–200. Pool-Goudzwaard A, van Dijke G, Mulder P, Spoor C, Snijders C, Stoeckart R. The iliolumbar ligament: its influence on stability of the sacroiliac joint. Clin Biomech. 2003;18:99–105. Panjabi M. The stabilizing system of the spine: Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5:383–389. Hides J, Richardson C, Jull G. Multifidus recovery is not automatic after resolution of acute, first-episode low back pain. Spine. 1996;21(23):2763–2769. Cresswell A, Thortensson A. Changes in intra-articular pressure, trunk muscle activation and force during isokinetic lifting and lowering. Eur J Appl Physiol. 1994;68:315–321. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci Sports Exerc. 1998;30:301–310. Cresswell A. Responses of intra-abdominal pressure and abdominal muscle activity during dynamic loading in man. Eur J Appl Physiol. 1993;66:315–320. Hodges P, Richardson C. Inefficient muscular stabilization of the lumbar spine associated with low back pain: A motor control evaluation of transverse abdominis. Spine. 1996;21(22):2640–2650. Taylor J, O’Sullivan P. Lumbar segmental instability: Pathology, diagnosis, and conservative management. In: Twomey L, Taylor J, eds. Physical Therapy of the low rd back. 3 ed. Philadelphia; Churchill Livingstone: 2000. Farfan H. Mechanical disorders of the low back. Philadelphia; Lea & Febiger: 1973. Bogduk N, Macintosh JE, Pearcy MJ. A universal model of the lumbar back muscles in the upright position. Spine. 1992;17(8):897–913. van Dieen JH, Selen LP, Cholewicki J. Trunk muscle activation in low-back pain patients, an analysis of the literature. J Electromyogr Kinesiol. 2003;13(4):333–351. Cook C. Lumbar Coupling biomechanics—A literature review. J Man Manip Ther. 2003;11(3):137–145. Pearcy M, Portek I, Shepherd J. The effect of low back pain on lumbar spine movements measured by three-dimensional x-ray analysis. Spine. 1985;10:150–153. Mellin G, Harkapaa K, Hurri H. Asymmetry of lumbar lateral flexion and treatment outcome in chronic low back pain patients. J Spinal Disorders. 1995;8:15–19. Winkel D, Aufdemkampe G, Matthijs O, Phelps V. Diagnosis and treatment of the spine. Gaithersburg, Maryland; Aspen Publication: 1996. Panjabi M, Oxland T, Yamamoto I, Crisco J. Mechanical behavior of the human lumbar and lumbosacral spine as shown by three-dimensional load-displacement curves. Am J Bone Jnt Surgery. 1994;76:413–424. Harrison D, Harrison D, Troyanovich S. Three-dimensional spinal coupling mechanics: Part one. J Manipulative Physiol Ther. 1998;21(2):101–113. Gibbons P, Tehan P. Spinal manipulation: indications, risks and benefits. J Bodywork Movement Therapies 2001;5(2):110–119. Fryette H. The Principles of Osteopathic Technique. Carmel CA; Academy of Applied Osteopathy: 1954. Faye LJ. Motion palpation of the spine. Huntington Beach; Motion Palpation Institute: 1984. Gertzbein S, Seligman J, Holtby R. Centrode patterns and segmental instability in degenerative disc disease. Spine. 1986;14:594–601. Plaugher G. Textbook of clinical chiropractic: A specific biomechanical approach. Baltimore, MD; Williams & Wilkins: 1993. Gracovetsky S, Newman N, Pawlowsky M, Lanzo V, Davey B, Robinson L. A database for estimating normal spinal motion derived from noninvasive measurements. Spine. 1995;20(9):1036–1046. Lund T, Nydegger T, Schlenzka D, Oxland T. Three-dimensional motion patterns during active bending in patients with chronic low back pain. Spine. 2002;27(17):1865–1874. Panjabi M, Hult J, Crisco J, White A. Biomechanical studies in cadaveric spines. In: th Jayson M., ed. The Lumbar Spine and Back Pain. 4 ed. London; Churchill Livingstone: 1992. Evans F, Lissner H. Biomechanical studies on the lumbar spine and pelvis. J Bone Joint Surg Am. 1959;41:278–290. Harrison D, Harrison D, Troyanovich S, Hansen D. The anterior-posterior full-spine view: The worst radiographic view for determination of mechanics of the spine. Chiropractic Technique. 1996;8:163–170. Rab G, Chao E. Verification of roentgenographic landmarks in the lumbar spine. Spine. 1977;2:287–293. Grice A. Radiographic, biomechanical and clinical factors in lumbar lateral flexion. Part 1. J Manipulative Physiol Ther. 1979;2:26–34. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. Gomez T. Symmetry of lumbar rotation and lateral flexion range of motion and isometric strength in subjects with and without back pain. J Orthop Sports Phys Ther. 1994;19:42– 48. Gertzbein S, Seligman J, Holtby R. Centrode patterns and segmental instability in degenerative disc disease. Spine. 1986;14:594–601. Kaigle A, Holm S, Hansson T. Experimental instability in the lumbar spine. Spine. 1995;20:421–430. Kaigle A, Wessberg P, Hansson T. Muscular and kinematic behavior of the lumbar spine during flexion-extension. J Spinal Disord. 1998;11:163–174. Panjabi M, Krag M, Chung T. Effects of disc injury on mechanical behavior of the human spine. Spine. 1984;9(7):707–713. Seligman J, Gertzbein S, Tile M, Kapasouri A. Computer analysis of spinal segment motion in degenerative disc disease with and without axial loading. Spine. 1984;9:566– 573. Weitz E. The lateral bending sign. Spine. 1981;6:388–397. Parnianpour M, Nordin M, Frankel V, Kahanovitz N. Trunk triaxial coupling of torque generation of trunk muscles during isometric exertions and the effect of fatiguing isoinertial movements on the motor output and movement patterns. Spine. 1988;13:982– 992. Panjabi M, Hult E, Crisco J, White A. Biomechanical studies in cadaveric spines. In: White A, Panjabi M. Clinical Biomechanics of the Spine. Philadelphia; Lippincott: 1978. Lai PL, Chen LH, Niu C, Fu T, Chen WJ. Relation between laminectomy and development of adjacent segment instability after lumbar fusion with pedicle fixation. Spine. 2004;29(22):2527–2532 Panjabi M, Krag M, Chung T. Effects of disc injury on mechanical behavior of the human spine. Spine. 1984;9(7):707–713. Keating J, Bergman T, Jacobs G, Finer B, Larson K. The objectivity of a multidimensional index of lumbar segmental abnormality. J Manipulative Physiol Ther. 1990;13:463–471. Hardy G, Napier J. Inter- and intra-therapist reliability of passive accessory movement technique. New Zealand J Physio. 1991;22–24. Vilkari-Juntura E. Inter-examiner reliability of observations in physical examinations of the neck. Phys Ther. 1987;67(10):1526–1532. Lee M, Latimer J, Maher C. Manipulation: Investigation of a proposed mechanism. Clin Biomech. 1993;8:302–306. Maher C, Adams R. Reliability of pain and stiffness assessments in clinical manual lumbar spine examinations. Phys Ther. 1994;74(9):801–811. Maher C, Latimer J. Pain or resistance: The manual therapists’ dilemma. Aust J Physiother. 1992;38(4):257–260. Boline P, Haas M, Meyer J, Kassak K, Nelson C, Keating J. Interexaminer reliability of eight evaluative dimensions of lumbar segmental abnormality. Part II. J Manipulative Physiol Ther. 1992;16(6):363–373. Li Y, He X. Finite element analysis of spine biomechanics. J Biomech Engineering. 2001;18(2)288–289,319. Troke M, Moore AP, Maillardet FJ, Hough A, Cheek E. A new, comprehensive normative database of lumbar spine ranges of motion. Clin Rehabil. 2001;15:371–379. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ