Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
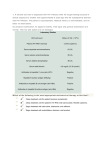
Management of the Newly Diagnosed HIV-infected Patient Sarah Lewis MHS, PA-C Case Presentation • A 32 yo woman presents for care at your clinic, referred from a public health clinic after testing positive for HIV • She presented for testing after discovering a past boyfriend of hers is HIV+ • What questions do you have for her? What does she know about HIV? • Human Immunodeficiency Virus • HIV is no longer a ‘death sentence’ – Diabetes mellitus can be a useful analogy • • • • Chronic, incurable disease Not immediately fatal Eventually requires medications in most cases Can usually be controlled with careful adherence, management, and follow-up • As with the care of persons with diabetes, working in a team and providing continuing education is essential throughout the course of the disease • Patients educated about HIV and the potential for resistance have better adherence to therapy1,2 1. Malow RW, et al. Alcohol Drug Abuse 1998;49:1021-4. 2. Tuldra A, et al. 39th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1999; Abstract 595. HIV 101 for Patients History of HIV • retroviruses discovered in 1900 in animals only • HIV related to primate retroviruses, that may have crossed species into humans and undergone mutations that became HIV as early as 1675?? • established in Africa as an epidemiologic disease after 1930 • 1980 1st retroviruses found to affect T cells • Gallo, Essex, & Montagnier pioneers of the cause of AIDS History of HIV • 1981 1st descriptions of immunodeficiency disease in previously healthy person in medical literature • specific retrovirus, HIV-1 was not isolated until 1983 • HIV-2 (West Africa) is distinct from HIV-1 (Central Africa) by a longer clinical latency period • although syndrome of AIDS was not reported until 1981, isolated cases were clearly reported in 1950s & 1960s History of HIV • HIV antibodies found in blood sample from 1950s in Central Africa suggesting emergence in 1930s; • remained localized there until spreading to Africa and then Haiti in late 1970s • to US & Europe from Haiti & Africa • first suspect US case 1968 15 y/o BM St. Louis w/ Kaposi’s & disseminated Chlamydial; blood samples + for HIV • HIV blood transmission documented 1982 • HIV testing 1985 • HIV drug Rx approved 1987 Primary HIV Infection (PHI) a/k/a Acute HIV Infection • • • • • • • Pathogenesis Clinical Presentation Diagnosis Epidemiology PHI and the Natural History of HIV Disease Treatment Options Conclusions & Recommendations Etiology: HIV Structure • RNA retrovirus • RNA into DNA an absolute must to multiply • core, nucleocapsid • double stranded RNA-genome at least nine genes • protein & enzymes – reverse transcriptase (RNA-to-DNA) – polymerase (DNA-to DNA) – ribonuclease (destroys old RNA) – integrase (splices viral DNA into host DNA, now permanent) – protease (molecular scissor) • spherical lipid bilayer viral envelope Life Cycle of HIV Sites of Action of antiretroviral Medications Day 0 Exposure to HIV at mucosal surface (sex) Day 0-2 Virus collected by dendritic cells, carried to lymph node Day 4-11 HIV replicates in CD4 cells, released into blood Day 11 on Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. Virus spreads to other organs Primary HIV Infection: Pathogenesis Plasma HIV RNA (copies/mL) Symptoms 1,000,000 100,000 Plasma RNA Viral Load 10,000 1,000 CD4 Cell Count (cells/mm³) 10,000,000 1,000 100 CD4 Cell Count 10 500 1 4-8 Weeks Up to 12 Years 2-3 Years How often do people with PHI seek health care? Swiss cohort • 87% of seroconverters (20/23) in cohort study had symptoms • 95% of these patients had medical evaluation • PHI considered in only 5 of 19 patients PHI often leads to medical evaluation, but is under-diagnosed! Schacker T et al. Ann Int Med 1996;125:257-64. How does HIV cause AIDS? • HIV infects and destroys an important type of cell in the body’s immune system known as the T-helper (TH) cell, also known as the CD4 cell How does HIV cause AIDS? • CD4 cells direct and coordinate other cells in the immune system to battle infections • When CD4 cells are destroyed, the body loses its ability to fight off infections HIV Infection is characterized by a steady decline in the number of CD4 cells Acute Infection Asymptomatic HIV Infection AIDS CD4 Cell Count 1,000 CD4 Cells 500 200 4-8 Weeks Up to 12 Years Time 2-3 Years HIV Infection is characterized by a steady decline in the number of CD4 cells CD4 Cell Count (cells/mm³) Acute Infection Asymptomatic HIV Infection AIDS 1,000 CD4 cell count 500 200 high risk of opportunistic infections 4-8 Weeks Up to 12 Years Time 2-3 Years How does HIV cause AIDS? • Infections that develop as a result of HIV-inflicted damage to the immune system are called “opportunistic infections” or “OIs” • When someone with HIV develops an opportunistic infection, they are diagnosed with AIDS How does HIV cause AIDS? • In the past, virtually all patients diagnosed with AIDS died within a few years • Now, with treatment, many patients diagnosed with AIDS are surviving many years with the disease What is the “Viral Load”? • The HIV viral load is simply a measure of the quantity of HIV in a drop (mL) of a patient’s blood, and it is usually measured in copies/mL • In general, the higher the viral load, the faster CD4 cells are destroyed Clinical Approach to the Diagnosis of Primary HIV Infection • Exposure • Signs & Symptoms • Laboratory Testing Exposure Risks (average, per episode, involving HIV-infected source patient) Percutaneous (blood)1 Mucocutaneous (blood)2 Receptive anal intercourse3 Insertive anal intercourse4 Receptive vaginal intercourse5 Insertive vaginal intercourse6 Receptive oral (male)7 Female-female orogenital8 IDU needle sharing9 Vertical (no prophylaxis)10 0.3% 0.09% 0.3 - 3% 0.06% 0.1 – 0.2% 0.03 – 0.14% 0.06% 4 case reports 0.67% 24% Primary HIV Infection: Signs & Symptoms • 40-90% of patients will be symptomatic • A mononucleosis-like illness of non-specific signs and symptoms • Signs and symptoms typically begin 1-4 weeks post-exposure • High index of suspicion is critical Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. Schacker T, et al. Ann Intern Med. 1996;125:257-264. Primary HIV Infection: Common Signs & Symptoms fever 86 lethargy 74 myalgias 59 rash 57 headache 55 pharyngitis N = 160 patients with PHI in Geneva, Seattle, and Sydney 52 adenopathy 44 0 10 20 30 40 50 60 70 % of patients Vanhems P et al. AIDS 2000; 14:0375-0381. 80 90 100 Primary HIV Infection: Other Signs & Symptoms aseptic meningitis 24 oral ulcers 15 genital ulcers 10 thrombocytopenia 45 leukopenia 40 transaminitis 21 0 20 40 60 % of patients Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. 80 100 Primary HIV Infection Rash Mucosal Lesions Trunk and face > limbs Small pink macules Oral ulcers, thrush (Kahn, NEJM, 1998) Oral Ulcers in Acute HIV Infection From: Walker, B. 40th IDSA, Chicago 2002. Genital Ulcer in Acute HIV Infection From: Walker, B. 40th IDSA, Chicago 2002. 1 mil HIV RNA 100,000 + _ 10,000 Ab P24 + 1,000 100 Exposure Symptoms 10 0 20 30 Days 40 50 HIV-1 Antibodies HIV RNA Diagnostic Testing for PHI Diagnostic Testing: Viral Load • More sensitive than HIV antibody or p24 Ag test3 • Positive one to three weeks before antibody test1 • Typically high level, e.g. greater than 50,000-100,000 copies/mL2,3 • False positives can occur – Most false positives are low level (<10,000 copies/mL) – HIV VL <10,000 copies/mL should probably be considered “indeterminate” 1. Busch MP, Satten GA. Am J Med 1997;102:Suppl 5B:117-24. 2. Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. 3. Daar ES et al. Ann Intern Med. 2001;134:25-29. Diagnostic Testing: HIV Antibody • The gold standard for diagnosis of HIV infection when used with confirmatory Western Blot • Antibody conversion typically 22-27 days following infection1 1. Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. Why do we Care about Diagnosing PHI? • Public Health: – Patients with PHI are likely to be highly infectious – Diagnosis of HIV infection may lead to safer sex • Personal Health – 40% of patients with HIV not diagnosed until they have AIDS – Antiretroviral therapy (ART) during PHI may alter the natural course of HIV disease HIV Rapid Tests Public Health Need for Rapid HIV Tests • High rates of non-return for test results – In 2000, 31% did not return for results of HIVpositive conventional tests at publicly funded sites • Need for immediate information or referral for treatment choices – Perinatal settings – Post-exposure treatment settings • Screening in high-volume, high-prevalence settings Multispot HIV-1/HIV-2 Uni-Gold Recombigen Reveal G2 OraQuick Advance Multispot HIV-1/HIV-2 Uni-Gold Recombigen Reveal G2 OraQuick Advance Four FDA-approved Rapid HIV Tests Sensitivity (95% C.I.) Specificity (95% C.I.) OraQuick Advance - whole blood - oral fluid - plasma 99.6 (98.5 - 99.9) 99.3 (98.4 - 99.7) 99.6 (98.5 - 99.9) 100 (99.7-100) 99.8 (99.6 – 99.9) 99.9 (99.6 – 99.9) Uni-Gold Recombigen - whole blood - serum/plasma 100 (99.5 – 100) 100 (99.5 – 100) 99.7 (99.0 – 100) 99.8 (99.3 – 100) Four FDA-approved Rapid HIV Tests Sensitivity (95% C.I.) Specificity (95% C.I.) Reveal G2 serum plasma 99.8(99.2 – 100) 99.8(99.0 – 100) 99.1 (98.8 – 99.4) 98.6 (98.4 – 98.8) Multispot serum/plasma HIV-2 100 (99.9 – 100) 100 (99.7 – 100) 99.9 (99.8 – 100) Additional Rapid Tests • FDA approved – May 2006 Sure Check Stat Pak Confirmatory Testing • Confirmatory test is essential (not just EIA) • For Western blot: – Venipuncture for whole blood – Oral fluid specimen • Follow-up testing of persons with negative or indeterminate Western blot results after 4 weeks The Berlin Patient • Treated soon after acute HIV infection with didanosine, indinavir, and hydroxyurea • Baseline VL 80,000-89,000 pre-treatment • Treatment briefly interrupted twice in first 4 months of treatment • Viral rebound during first interruption but not the second • VL remained undetectable after treatment was stopped a third time Lisziewicz J et al. NEJM 1999; 340: 1683-1684. Unplanned Treatment Interruptions of ART following Primary HIV Infection: “the Berlin Patient” ARV Rx Started Prior to HIV Seroconversion ddI + HU + IDV No ARV Rx Lisziewicz J et al. N Engl J Med 1999;340:1683. Primary HIV Infection: Pathogenesis Anti-HIV T-cell response Sero-conversion Antibody response Plasma HIV RNA (copies/mL) 1,000,000 100,000 Plasma RNA Viral Load 10,000 Viral set point 1,000 100 CD4 Cell Count 10 Up to 12 Years 1,000 500 1 4-8 Weeks CD4 count (cells/mm³) 10,000,000 2-3 Years A lot of important stuff happens here From Antigen-Presenting Cell (APC) to CD4 Cell Destruction APC HIV CD4 Cell Activated CD4 Cell HIV Picture Adapted from: Cohen DE, Walker BD. Clin Infect Dis 2001;32:1756-68 Loss of HIV-specific Cytotoxic T-Lymphocyte Response (CTL) CD4 Cell Activated CD4 Cell Antigen-Presenting Cells Lymphokines HIV HIV CD8 Cell HIV-Infected CD4 Picture Mature CD8 CTL Activated CD8 Pre CTL Adapted from: Cohen DE, Walker BD. Cellular Immune Response to Acute HIV Infection Acute HIV 100 Weak CTL Rapid Progression HIV RNA 80 60 Moderate CTL 40 20 Moderate Progression Strong CTL Slow Progression 0 0 1 2 3 4 5Time6 7 8 6 months Slide courtesy David Spach, Hypothesis Initiation of effective ART in the setting of Primary HIV Infection may preserve critical HIV-specific CD4 cells, allowing for a potentially more robust CTL response to HIV Early ART with Structured Treatment Interruptions: Theory • ART administered during primary HIV infection preserves HIV-specific CD4 cells • Allows potential for robust HIV-directed CTL response • ART interrupted periodically to ‘prime’ the immune system to recognize HIV, build CTL response • ART is re-initiated before HIV inflicts too much damage • With subsequent treatment interruptions, improved CTL response results in progressively lower viral set point • Ultimately, immune system may be able to exert adequate control over HIV without ART Structured Treatment Interruptions Structured Treatment Interruptions (STIs) What’s the Evidence? STIs During PHI: Evidence From an Animal Model • ART with STIs (3 weeks on/3 weeks off) compared to standard ART in macaques acutely infected with SIV and with chronic infection • In acutely-infected macaques, viral rebound rate decreased significantly during subsequent treatment interruptions • Virologic control in these animals was associated with vigorous SIV-specific CD8-mediated immunity Lori F et al. 40th ICAAC, September 2000, abstract L-17. STIs During PHI: Evidence of Improved Virologic Control • Trial involving 14 patients diagnosed with PHI • All patients initiated combination ART during PHI, prior to seroconversion, and had full viral suppression for at least 8 months before STIs implemented • All ARVs were discontinued simultaneously • Therapy re-instituted if VL persistently (>3 weeks) over 5,000 copies/mL or if VL at any time over 50,000 copies/mL Walker B. State of the Art Lecture and Summary. 8th CROI, Session STIs During PHI: Evidence of Improved Virologic Control • Initial success: 8/14 patients were able to discontinue ART following one or more STIs, maintaining a VL less than 500 copies/mL • However, all but 3 of these patients subsequently lost virologic control Walker B. State of the Art Lecture and Summary. 8th CROI, Session STIs during Chronic Infection • Results variable but less encouraging • No consistent improvement in virologic control • Significant proportion fail to regain CD4 count prior to treatment interruptions • May nonetheless prove useful for other reasons Potential Benefits of Treatment during PHI • • • • Suppress initial burst of viremia ? alter viral set-point Decrease viral evolution Preserve CD4 lymphocytes (both absolute number and HIV-specific) • Potentially decrease risk of transmission • Possibly allow for therapy to be stopped Potential Risks of Treatment during PHI • Drug toxicity • Costs of possible lifelong therapy • Starting therapy in patients who may never had needed it • Early development of resistance • Limited evidence to date of clinical benefit Treatment of PHI: Recommendations • Patients should be informed of the risks, benefits, and uncertainties • For treatment, consider two nucleoside analogues plus a protease inhibitor or an NNRTI (consider US treatment guidelines) • STI strategies remain experimental • Consider referrals to studies when possible Primary HIV Infection: Conclusions • PHI is under-diagnosed • May represent a critical opportunity to intervene • A high index of suspicion, recognition of key signs & symptoms, and lab testing are required for the diagnosis • ART may provide opportunity for improved longterm virologic control of HIV • Ongoing studies should clarify the potential role of treatment during PHI, including Structured Treatment Interruptions Case Presentation continued • How is she coping with the diagnosis? Common responses: - “I’ve tried not to think about it, ever since I found out” - “I’ve watched so many friends die, and now I’m next” - “My friends tell me it’s not that big a deal” - “I’ve been researching this on the internet and I have a 10-page list of questions for you” Case Presentation continued • Ask about sources of social support – Friends, family – Community organizations • Offer counseling How and when did she contract HIV? • What are her risk factors for acquiring HIV? – She has been an injection drug user for the past 10 years – She also admits to unprotected sex with drug use – She does not know when she might have contracted HIV, but her last HIV test was negative about one year ago • Risk factor identification can guide counseling and prevention Why do we care about when she contracted her HIV? • Resistance – Increasing transmission of drug-resistant HIV strains – Resistance testing generally indicated for patients infected within the past 2-3 years, even if antiretroviral therapy is not being considered in the near future (ability of currently available resistance assays to detect resistance wanes with time) • Primary HIV Infection (PHI) – Loss of HIV-specific CD4 cells occurs immediately after PHI – Some evidence that early treatment of PHI may favorably influence subsequent course of disease1,2 1. Lisziewicz J et al. N Engl J Med 1999;340:1683. 2. Walker BD. Nature 2000;407:313-4. Time Trends in Primary HIV-1 Genotypic Drug Resistance Among Recently Infected Persons % of resistant isolates 25 NRTI any NNRTI any PI any primary two classes three classes 20 15 10 5 0 1996-97 1998-99 JAMA. 2002 Jul 10;288(2):181-8. 2000-01 Past Medical History • Injection drug use (crystal methamphetamine) for past 5 years; no history of treatment • No other recreational drug use, no EtOH • Smoker: 2 PPD for past 10 years • Depression • Allergic rhinitis • No established primary care provider for past 5 years Medications • Diphenhydramine (Benadryl) • Ibuprofen (Motrin) prn • St. John’s Wort Social History • Single, no children • Born & raised in Idaho but has lived in Eastern Washington for past 8 years; no other travel • Estranged from family but many friends • Works as a waitress Review of systems • Intermittent vaginal labial pain for two weeks • Otherwise negative ROS Physical exam • Afebrile, vital signs normal, weight 110 lbs • PE unremarkable except for shallow vulvar ulcers Photo courtesy Beth Schenck, MD What tests would you order? • • • • • • • CD4, viral load CBC w/ differential Comprehensive metabolic panel Toxoplasmosis, CMV IgG, RPR Hepatitis panel (hepatitis A, B, C) HSV culture from labial region (or HSV serology?) Screening for other sexually transmitted infections (STIs): oral, rectal, urethral GC and urethral CT Any interventions? • 10 day course of acyclovir (400mg po tid) • Counseling re: safer sex, needle sharing • Follow up – Social work/case management – Substance abuse treatment, if interested • She isn’t! – Consider psychiatry/counseling – Nutritionist – Return approximately 2 weeks for counseling and follow-up lab results Lab results • • • • • • • • CBC, electrolyte panel unremarkable AST=45, ALT=92, other LFTs normal Absolute CD4=220 cells/mm³ (16%) HIV viral load=108,000 copies/mL HAV Ab+ HBsAb-, HBcAb-, HBsAgHCV AbToxo Ab+, CMV Ab+, RPR- Follow-up appointment • She returns in two weeks for follow-up • Receiving counseling but still “pretty down” about the diagnosis • Still using crystal methamphetamine, though less • How do you explain the CD4 and VL results to her? HIV Infection is characterized by a steady decline in the number of CD4 cells Acute Infection Asymptomatic HIV Infection AIDS CD4 Cell Count 1,000 CD4 Cells 500 200 4-8 Weeks Up to 12 Years Time 2-3 Years HIV Infection is characterized by a steady decline in the number of CD4 cells CD4 Cell Count (cells/mm³) Acute Infection Asymptomatic HIV Infection AIDS 1,000 CD4 cell count 500 200 high risk of opportunistic infections 4-8 Weeks Up to 12 Years Time 2-3 Years CD4 Count, Viral Load, and Clinical Course Primary Infection Seroconversion 10,000,000 AIDS Plasma HIV RNA 1,000,000 100,000 10,000 Viral Load 1,000 1,000 CD4 Cells 100 CD4 Cell Count Intermediate Stage 500 10 1 4-8 Weeks Up to 12 Years 2-3 Years What about HIV treatment? • She would like to start “the cocktail” she’s heard about for HIV • Should she initiate treatment? – Considerable variation in day-to-day CD4 and VL counts – Co-incident infections often result in lower CD4 and higher VL – Repeat measurements indicated to establish true baseline How do you explain her elevated transaminases? • Up to 19% of HIV+ individuals with chronic hepatitis C have negative HCV Ab titers1 • HCV RNA PCR (viral load) testing is indicated if chronic hepatitis C suspected 1. George, et al. JAIDS 2002;31:154-162 Case Presentation continued • You order repeat CD4 count and viral load as well as hepatitis C viral load and an HIV resistance assay • Results – – – – HCV VL=1,688,340 copies/mL CD4 count=280 cells/mm3 HIV VL=88,000 copies/mL Resistance assay does not reveal any resistance Case Presentation continued • She returns to clinic two weeks later • You review the results with her • She is anxious to start HIV medications • Should you start her on antiretroviral therapy? When Should Patients with HIV be Treated with Antiretroviral Therapy (ART)? • Benefits – reduced morbidity & mortality – immune system recovery • Drawbacks – toxicities – lifestyle changes – potential for developing resistance Initiation of ART: Key Considerations • Symptoms & opportunistic infections • CD4 count • HIV viral load • Anticipated adherence - patient ‘readiness’ (cells/mm³) Mellors et al. Ann Intern Med 1997;126:946. When Should ART be Initiated? An analysis of prospective studies • 13 cohort studies from Europe & North America • 12,574 patients initiating ART – – – – – Median age 38; mostly men Median baseline CD4 count 250; VL 74,000 Median month of ART initiation: 12/1997 Mostly protease inhibitor (PI)-based regimens 24,310 person-years of follow-up Egger et al. Lancet 2002; 360:119-30. Findings: effect of baseline CD4 count and VL on response to ART Years from starting HAART Egger et al. Lancet 2002; 360:119-30. Findings: Effect of risk factor for HIV acquisition and age on clinical progression Egger et al. Lancet 2002; 360:119-30. Conclusions • CD4 count at initiation of ART carried strongest prognostic significance, corroborating findings from other studies1-4 • Age, infection via IDU, history of AIDSrelated illness also appeared to affect durability of clinical response to ART 1. Chen RY et al. 8th CROI, Chicago 2001 2. Hogg RS et al. JAMA. 2001;286:2568-2577 3. Sterling et al, 9th CROI, Seattle 2002 4. Palella et al, 9th CROI, Seattle 2002 Caveats • High VL (>100,000 copies/mL) also carried prognostic significance, but – few patients initiated on efavirenz or ritonavir-boosted regimens – other recent studies have not demonstrated a clear correlation between baseline viral load and efficacy of ART1,2 • Observational study: other potential confounding factors could have affected results – However, randomized controlled trial very unlikely 1. Philips AN et al. JAMA 2001;286:2560-2567. 2. Hogg RS et al. JAMA 2001;286:2568-2577. Implications for Clinical Practice • Ideally, initiate ART before CD4 count drops below 200 cells/mm³ and before clinical symptoms develop • A benefit for treatment before CD4 count falls below 350 may exist, but the small risk of clinical progression if therapy is deferred must be balanced against drawbacks of ART • If CD4 already less than 200 or clinical progression has occurred, ART is clearly indicated as soon as patient is ready to start Implications for Clinical Practice: Significance of Baseline Viral Load • Initiation of ART before VL >100,000 may allow for more therapeutic options and greater clinical success • However, highly potent efavirenz (Sustiva)- or lopinavirritonavir (Kaletra)- based regimens may be equally effective in patients with high baseline viral loads1-3 • VL a marker for rate of CD4 decline: consider more frequent monitoring in patients with high VL? 1. XIV International AIDS Conference, July 2002. Abstract TuOrB1189 2. Arribas JR et al. AIDS 2002;16(11):1554-6. 3. Walmsley S et al. NEJM 2002 346(26):2039-46. When Should ART be Initiated? DHHS Guidelines Clinical Category CD4 count Viral Load Recommendation Symptomatic (AIDS, severe Sx) Any value Any value Treat Asymptomatic, AIDS < 200/mm3 Any value Treat Asymptomatic > 200/mm3 Any value but < 350 Treatment should generally be offered Asymptomatic > 350/mm3 > 55,000 copies/mL Asymptomatic > 350/mm3 < 55,000 copies/mL Some experts would recommend initiating treatment Many experts would defer therapy and observe DHHS Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents, October 6, 2005. Impact of CD4 and Viral Load on Initiation of ART: Summary • The optimal time to initiate therapy is: – – – – unclear before CD4 drops below 200 cells/mm3 perhaps when CD4 drops below 350 cells/mm3 determined more by CD4 count than by viral load • Viral load – predicts the slope of CD4 decline – may help determine whether to start closer to CD4 count of 200 cells/mm3 or 350 cells/mm3 Back to the Case • 31 yo woman with asymptomatic HIV infection • CD4=280 cells/mm3 • Viral load=88,000 copies/mL • Should she initiate antiretroviral therapy? When Should ART be Initiated? DHHS Guidelines Clinical Category CD4 count Viral Load Recommendation Symptomatic (AIDS, severe Sx) Any value Any value Treat Asymptomatic, AIDS < 200/mm3 Any value Treat Asymptomatic > 200/mm3 Any value but < 350 Treatment should generally be offered Asymptomatic > 350/mm3 > 55,000 copies/mL Asymptomatic > 350/mm3 < 55,000 copies/mL Some experts would recommend initiating treatment Many experts would defer therapy and observe DHHS Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents, March 23, 2004. Initiation of Antiretroviral Therapy: Key Considerations • Symptoms & opportunistic infections • CD4 count • HIV viral load • Anticipated Adherence - patient ‘readiness’ Adherence “Drugs don’t work if people don’t take them.” - C. Everett Koop Virologic Control falls sharply with diminished adherence Patients with HIV RNA <400 copies/mL, % 100 80 60 40 20 0 >95 90-95 80–90 70-80 <70 PI adherence, % (electronic bottle caps) Paterson, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago, IL. Abstract 92. Predictors of Poor Adherence • • • • • • • Active alcohol or substance abuse1,2,6 Work outside the home for pay1 Depressed mood1 Lack of perceived efficacy of ART3 Lack of advanced disease4 Concern over side effects4 Regimen complexity5 1. Chesney MA. 37th ICAAC, 1997; Toronto. Abstract 281. 2. Cheever LW, Curr Infect Dis Rep 1999 Oct;1(4):401-407. 3. Horne R, et al. 39th ICAAC, 1999; San Francisco. Abstract 588. 4. Wenger N, et al. 6th CROI, 1999, Abstract 98. 5. Stone VE, et al. JAIDS 2001; 28:124-131 6. Howard AA et al. AIDS 2002;16:2175-82. Factors Associated with Higher Levels of Adherence • • • • • Twice-daily or once-daily regimens1,4 Belief in own ability to adhere to regimen1 Not living alone2 Dependent on a significant other for support2 History of opportunistic infection or advanced HIV disease3 1. Eldred L, et al, J Acquir Immune Defic Syndr Hum Retrovirol 1998;18:117-125. 2. Morse EV et al, Soc Sci Med 1991;32:1161-1167. 3. Singh N, et al, AIDS Care 1996;8:261-269. 4. Stone VE, et al. JAIDS 2001; 28:124-131 Factors Associated with Higher Levels of Adherence • Belief in efficacy of antiretroviral therapy • Belief that non-adherence will lead to viral resistance Wenger N, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago. Abstract 98. Mental Health Issues • She refuses to see a psychiatrist, but is open to depression treatment by you – Should she continue her St. John’s Wort? • St. John’s Wort has significant interactions with many antiretroviral agents • Efficacy in major depression questionable Case Presentation continued • You substitute paroxetine (Paxil) for St. John’s Wort • She returns in a month; her depression is improving • She is still using crystal methamphetamine • Would you start her on antiretroviral therapy? • What is your estimate of her ability to adhere to treatment? Clinicians’ Estimates of Adherence Not Much Better Than Random Bangsberg Paterson Haubrich Steiner Bosely Charney Caron Gilbert Blowey Mushlin 2001 2000 1999 1995 1995 1967 1978 1980 1997 1977 JAIDS Annals Int Med AIDS Arch Int Med Eur Resp J Pediatrics Clin Pharmacol Can Med Assoc J Ped Nephrology Arch Int Med Slide courtesy David Bangsberg, MD ART ART ART AZT Inhaled terbutaline Penicillin Antacids Digoxin Cyclosporin Hypertensive What about her hepatitis C? • HIV accelerates the course of hepatitis C, but variable rates of progression still seen • Avoiding alcohol, other insults to the liver is critical • Co-infection with HIV also reduces the response rate to treatment for hepatitis C – but treatment can be helpful, even curative, and deserves consideration • For her, probably best to focus on HIV first, but discussing the possibility of future treatment and a Hepatology consultation is a good idea Case Presentation continued • You start her on a regimen of AZT (zidovudine; Retrovir) + 3TC (lamivudine; Epivir) + efavirenz (Sustiva)* * Note: efavirenz is a potential teratogen and should not be used in pregnant women or women with high potential to become pregnant “Preferred” regimens for treatment-naïve patients • efavirenz/tenofovir/emtricitabine • ritonavir-boosted atazanavir + tenofovir/emtricitabine • ritonavir-boosted darunavir + tenofovir/emtricitabine • raltegravir + tenofovir/emtricitabine. Antiretroviral Therapy: Optimal Response ART Initiated CD4 count (cells/mm3) Viral Load (copies/mL) 1000000 Viral Load 100000 10000 1000 100 50 50 10 0 1 2 3 Time (months) 4 5 6 7 8 Antiretroviral Therapy: Optimal Response ART Initiated 200 Viral Load 100000 CD4 Count 150 10000 100 1000 50 100 50 50 10 0 0 1 2 3 4 Time (months) 5 6 7 8 CD4 count (cells/mm3) Viral Load (copies/mL) 1000000 Health Care Maintenance • Vaccines – – – – Hepatitis A, hepatitis B (if not immune) Pneumococcal Influenza Tetanus • Pap smears – Every 6 months initially, then yearly if negative – If ASCUS or more significant abnormality colposcopy per latest guidelines (do not triage by HPV status) Health Care Maintenance • Breast, prostate, colorectal cancer screening – Same as for HIV-negative patients • Cholesterol screening – Protease inhibitors, efavirenz, some NRTIs associated with dyslipidemia – Check baseline lipids before treatment and periodically after initiation of treatment – Higher rates of CAD among HIV-infected patients starting to be seen Health Care Maintenance • PPD – Treatment of LTBI warranted for: • ≥5mm of induration on PPD, or • Recent contact with someone with active TB – LTBI treatment: • INH + pyridoxine x 9 months • Rifampin + pyrazinamide x 2 months is NO LONGER RECOMMENDED • STI screening – Annual anal/pharyngeal/urethral screening for GC, urethral chlamydia recommended for MSM – Annual RPR – More frequent STI screening may be appropriate for some patients Where is she now? • She achieves an undetectable viral load in four months; CD4 count rises to 410 cells/mm3 • Pap smear negative, vaccinations initiated • What would you focus on next? • Main health issues besides HIV: – Hepatitis C – Crystal methamphetamine use – Smoking Pulmonary Manifestations • Pneumocystis carinii (actually a fungus) – prophylaxis w/ Bactrim-DS if CD4+ < 200 • • • • • CMV M. tuberculosis (4% of HIV) Histoplasma Staphylococcus various tumors Pneumocystis Carinii (PCP) Mucocutaneous Manifestations • may present early • viral exanthem of seroconversion: erythematous, fine maculopapular rash • face trunk & arms • pruritis, fever, malaise, night sweats, fatigue, pharyngitis wt. loss, N/V/D/HA, lymphadenopathy • allergic, infectious, neoplastic • viral: HSV, VZ, EBV, HPV (genital warts) Oral Hairy Leukoplakia • white-grey, thickened, raised lesions, vertical folds or “hairs” that form on tongue & buccal mucosa • sides of tongue typical; cannot be scraped off like candida 18 y/o WM c/o of rectal bleeding; high school jock, popular; dx genital warts; HIV + 33 y/o WM w/ AIDS X 2 yrs. c/o “hemorrhoids acting up” dx rectal carcinoma Extensive vulvar condylomata acuminata Cervical intraepithelial neoplasia Herpes Simplex Virus • painful vesicles on red base; rupture & crust • become large, ulcerative, necrotic • genitalia, digits, perianal or perioral Lesions of Genital Herpes Herpes Zoster (Shingles) involving the face & eye Herpes Zoster (Shingles) Staphylococcus aureus • folliculitis, furuncles or bullous impetigo Fungal Skin Infections • Candida, Cryptococcus, or Histoplasma Kaposi’s Sarcoma others: squamous cell carcinoma, basal cell carcinoma, cutaneous lymphomas Neurologic Manifestations • • • • • • • • • • viral encephalitis (numerous agents) meninigitis (numerous agents) parasitic cerebral toxoplasmosis lymphoma neurosyphilis AIDS dementia spinal myelopathy or myelitis zoster radiculopathy polyneuropathy Ocular Manifestations • AIDS retinopathy: immune or CMV • CMV retinitis AIDS and Cytomegalovirus (CMV) Retinitis T4 Cell Count <50/cu.mm National HIV/AIDS Clinician’s Consultation Center • Warmline: Offers treating clinicians upto-the-minute HIV clinical and drug information and individualized, expert case consultation • Monday – Friday 6am to 5 pm PST • 1-800-933-3413 • Warmline is a free service to health care providers Useful references • NIH AIDS info (incredible site) http://www.aidsinfo.nih.gov/Default.aspx • John Hopkins AIDS Service http://www.hopkins-aids.edu • National Clinicians’ Postexposure Prophylaxis Hotline (PEPline) 1-888-448-4911 www.ucsf.edu/hivcntr • National HIV Telephone Consultation Service 1-800-933-3413 • Hepatitis Hotline 1-888-443-7232