Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
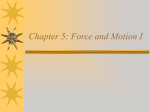
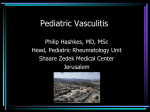
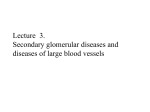
Cryoglobulinemia Andrew J Avery A.M. Report 08/19/09 Introduction • Precipitation of blood proteins at temperatures lower than 37ºC is referred to as cryoprecipitation • Cryoglobulins are either immunoglobulins or a mixture of immunoglobulins and complement components that precipitate from both serum and plasma (if just plasma, then called cryofibrinogen) Introduction • Wintrobe and Buell are credited with the first description of the cryoprecipitation phenomenon. In 1933, they described a patient with signs and symptoms of hyperviscosity associated with multiple myeloma Cryoglobulins Prevalence • The prevalence of clinically-significant cryoglobulinemia has been estimated at approximately 1:100,000 • Detectable levels of circulating CGs have been seen in a significant proportion of patients with chronic infections and/or inflammation: • HIV-15-20% • Connective Tissue Dz-15-25% • HEP C-40-50% Brouet Classification • Uses the immunological analysis of the CG to delineate the clonality of the responsible CG • Type I: Criterion is presence of isolated monoclonal Ig; ≈5-25% of cases; most commonly ass. w/ LPD • Type II: A mixture of polyclonal Ig in association with a monoclonal Ig; ≈40-60% of cases; most commly ass. w/ chronic viral inf • Type III: Mixed cryoglobulins consisting of polyclonal Ig; ≈40-50% of cases; most commonly ass. w/ CTD Etiology and Pathogenesis • CGs are often detectable in the serum of healthy pts, thus speculated that CGs reflect the ongoing physiological clearance of endogenous immune complexes by Igs with RF activity • Pathogenic CG responses may result from several factors: next slide Etiology and Pathogenesis • Chronic immune stimulation and/or lymphoproliferation, resulting in the production of higher concentrations of mono-, oligo-, or polyclonal CG. • Immune complex formation among CG and/or their target antigens • Defective and/or insufficient clearance of the resulting immune complexes, which accumulate and mediate disease Clinical Manifestations Signs & Sx Type I Type II Type III Purpura + +++ +++ Gangrene/Acrocyano +++ +/++ +/- Arthralgias>Arthritis + ++ +++ Renal + ++ + Neurologic + ++ ++ Liver +/- ++ +++ Clinical Manifestations • Cutaneous: Nearly all pts with CG syndromes develop erythematous macules to purpuric papules of the lower extremities (90-95%). • More commonly in Type I CG are infarction, hemorrhagic crusts and ulcers (10-25%); raynaud phenomenon, livedo reticularis, acrocyanosis; and post-inflammatory hyperpigmentation (30-50%). Palpable Purpura Clinical Manifestations • Musculoskeletal: Arthralgias and myalgias are common • • in type Type II and III CGs (>70%). Most commonly affect metacarpophalangeals, proximal phalangeals, knees, and ankles Neuropathy: Affects 70-80% of pts with mixed CG (Type II & III). Thought to be 2/2 vasculitis Pulmonary: Generally affects Types II & III (40-50%). PFTs often reveal evidence of small airways disease and impairment of gas exchange; sx generally range from dyspnea to cough and pleurisy Clinical Manifestations • Renal: Renal disease in mixed CG often results from immune complex disease; less frequently 2/2 thrombotic dz (more common in Type I) • Membranoproliferative glomerulonephritis seems to be more common in mixed CG • Isolated proteinuria or hematuria occur much more frequently than nephrotic or nephritic syndromes or acute renal failure. Clinical Manifestations • Other: Sjogrens syndrome (4-20%); Raynaud phenomenon (≈50%); hepatomegaly, abnormal liver function tests or abnormal liver biopsy (≈90%); lymphadenopathy (≈20%); splenomegaly (≈30%); abdominal pain (≈20%). All of the above are more common in Types II & III • CNS, heart, and retinal vessels are rarely affected unless in association with hyperviscosity due to type I CG Cutaneous Pathological Findings • Mixed CG most often reveal leukocytoclastic vasculitis (50%), less commonly inflammatory or noninflammatory purpura (10-20%), noninflammatory hyaline thrombosis (10%), or post-inflammatory sequelae (10%) • Type I CGs more often induce noninflammatory thrombotic lesions, sometimes with evidence of cutaneous infarction or hemorrhage Skin lesion in mixed cryoglobulinemia (PAS Stain) Renal Pathological Findings • Light and immunofluorescence microscopy: In Mixed CG, most common is membranoproliferative glomerulonephritis (60-80%), with endocapillary proliferation and subendothelial and/or intraluminal deposits of CGs, immunoglobulin, and/or complement proteins • Type I CG generally produce noninflammatory glomerulopathies, including thrombotic and hypocellular lesions, without evidence of vasculitis. Renal involvement in type II cryoglobulinemia Laboratory Findings • Measureable Cryoglobulins: Types II & III (1 to 5 mg/dL); Type I (5 to 10 mg/dl) • Complement: Normal in Type I; Decreased CH50, C1q, C2 and C4 and normal C3 in Types II & III • Elevated ESR and CRP • Autoantibodies: Types II & III often have elevated RF, ANA (many others as well) • Evidence of Viral Inf: HCV, HBV, HIV, EBV Treatment • Mild Dz: Mild symptoms, such as fatigue, arthralgias and myalgias, in the absence of clear evidence for end-organ damage. Initial trx is cold avoidance and nsaids. Low dose prednisone for inflam sx not responsive to nsaids • Mod-Severe Dz: pathologically-proven, CGrelated, end-organ-threatening vasculitis or thrombosis -Type I (malignancy related): chemo and/or radiation for bone lesions Treatment • Type I (non-malignancy)-Prednisone and Cycylophosphamide • Types II & III-generally involves immunosuppression and may also require plasmapheresis; May be combined with antiviral therapy when indicated • Severe Dz: hyperviscosity syndrome or vasculitis in Type I CG, or life or organ threatening vasculitis in mixed CG (Types II or III) warrants the addition of plasmapheresis to quickly reduce the CG burden Prognosis • The presence of CG does not seem to confer a significant morbidity or mortality risk over and above the underlying conditions • Survival: Mean survival is approximately 70% at 10 years after the onset of symptoms, 50% at 10 years after diagnosis, with death typically resulting from infection and cardiovascular disease