Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
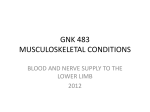
Chapter 29 Descending Branch of Lateral Circumflex Femoral Artery Grafting T.O. Tatsumi, S. Minohara, K. Kondoh 29.1 Introduction The lateral circumflex femoral artery (LFCA) is one of the branches of the deep femoral artery. The LFCA has three major branches: the ascending, transverse and descending branches. The ascending branches of the LFCA have a large diameter and do not taper like those of the radial arteries [1]. The descending branch of the LFCA has an attractive caliber and length. The LFCA has been used to supply composite tissue of skin and/or muscle in the field of plastic and reconstructive surgery [1 – 4]. Now, with the trend toward complete myocardial revascularization using the autologous arterial conduits, the descending branch of the LCFA can be used as an alternative arterial graft. 29.2 Anatomy The LCFA typically arises from the lateral side of the upper end of the deep femoral artery, but in some 15 % or so of instances it begins by the femoral artery above the deep femoral artery [5]. The LCFA runs laterally across the front of the iliopsoas muscle, between the branches of the femoral nerve, to pass behind the sartorius and rectus femorus muscle. Here, the LCFA divides into the three major branches: the ascending, transverse and descending branches (Fig. 29.1). The ascending branch ascends along the intertrochanteric line, under the tensor fasciae latae, lateral to the hip joint; it anastomoses with the superior gluteal and deep circumflex iliac arteries, supplying the greater trochanter, and forms an anastomotic ring round the femoral neck and head. The transverse branch, the smallest, passes laterally anterior to the vastus intermedius, pierces the vastus lateralis to wind round the femur, just distal to the greatest trochanter, anastomosing with the medial circumflex, inferior gluteal and first perforating arteries, which is the cruciate anastomosis in the buttock. Fig. 29.1. The right lateral circumflex femoral artery and its three major branches The descending branch, which sometimes runs from the deep femoral artery or the femoral artery, descends posterior to the rectus femoris, along the anterior border of the vastus lateralis, which it supplies; a long ramus descends in the vastus lateralis to the knee, anastomosing with the lateral superior genicular branch of the popliteal, accompanied by the nerve to the vastus lateralis. 29 234 X Rarely or Possibly Used Arterial Grafting Fig. 29.2. The descending branch of the left LFCA between the rectus femoris and the vastus lateralis muscle 29.3 Surgical Procedure The harvest of the descending branch of the LCFA can be performed simultaneously while the internal thoracic artery is isolated. It can be done before or after the harvest of the same side of the greater saphenous vein on the same position of the lower extremities. The incision to harvest the descending branch of the LFCA is made in the middle third of the thigh along the lateral margin of the rectus femoris muscle. The subcutaneous tissue and the fascia late are opened longitudinally along the length of the incision, so you can see the space between the rectus femoris muscle and the vastus lateralis muscle. The descending branch of the LCFA courses between the rectus femoris and the vastus lateralis muscle and is easily visualized when the rectus femoris muscle is retracted medially and the intermuscular space is explored. In general, you will find the descending branch of the LCFA is simply running straight to distal with little surrounding tissue (Fig. 29.2). The pulsation of the descending branch of the LCFA should be ensured by palpation to avoid applying the poor graft conduit to coronary artery bypass grafting (CABG). Poorer pulsation of the artery would be considered to indicate its obstruction or stenosis caused by some organic disorder of the artery. After the descending branch of the LCFA is isolated carefully from the surrounding tissue, the muscle branches are the descending branch of the LCFA tied and cut individually with hemoclips. Once mobilized, it is wrapped in a papaverine-soaked sponge and kept until the anastomosis. The descending branch of the LFCA is ligated and cut near its origin with silk proximally, and cut off distally at the appropriate length for bypass grafting; that is usually 10 – 15 cm. The descending branch of the LFCA is absolutely free from the patient and is soaked in the preservative solution after the injection of diluted papaverine hydrochloride (40 mg in 10 ml saline) into the free graft through the proximal site of the free graft. CABG is performed per protocol with or without cardiopulmonary bypass (CPB). The descending branch of the LFCA is grafted to the coronary branch except for the left descending branch. The proximal anastomosis is constructed onto the ascending aorta, saphenous vein graft (SVG) and internal thoracic artery (ITA). 29.4 Results Twenty of 21 descending branches of the LFCA harvested were satisfactory for use as arterial grafts after the first patient undergoing CABG used the descending branch of the LFCA [6]. The lengths of these grafts were 10 ~ 17 cm and the inner diameter measured 1.5 ~ 2.0 mm, similar to the ITA of the same patient. CABG with CPB was performed on 11 patients, and the other 9 patients underwent CABG without CPB. The perioperative and postoperative course of all patients was not eventful. The descending branch of the LFCA was grafted to the diagonal branch, posterolateral branch of circumflex, right coronary artery or the posterior descending branch of the right coronary artery. The proximal anastomosis of these grafts was on the ascending aorta, sa- 29 Descending Branch of Lateral Circumflex Femoral Artery Grafting phenous vein graft, left ITA or right ITA. The LFCA grafts anastomosed to the right ITA were used as an extension graft (I grafting technique). The LFCA grafts were anastomosed to the left ITA by the end-to-side method (Y grafting technique) (Table 29.1). Figure 29.3 Table 29.1. Sites of proximal and distal anastomoses of LFCA Proximal Distal Aorta 4 (1) RITA 7 (1) LITA 8 (1) SVG 1 RCA 7 (1) 4PD 2 4AV 1 (1) Diagonal 6 (1) PL 3 OM 2 No. of occluded anastomoses are in parentheses Fig. 29.3. The descending branch of the LFCA anastomosed right ITA is grafting to the 4PD shows the patent LFCA graft anastomosed right ITA grafting to the 4PD (Fig. 29.3). And Fig. 29.4 shows the patent LFCA graft anastomosed left ITA grafting to the diagonal branch (Fig. 29.4). The patency rate of the LFCA graft was 85 % at the early postoperative period (Table 29.1). In these cases, we have seen none of the complications of lower limb postulated as a consequence of harvesting the descending branch of the LFCA. 29.5 Comment Several points regarding the use of the descending branch of the LFCA as a bypass graft can be addressed. With regard to the quality of the vessel, the descending 235 236 X Rarely or Possibly Used Arterial Grafting Fig. 29.4. The descending branch of the LFCA anastomosed left ITA by the Ygrafting technique is grafting to the diagonal branch branch of the LCFA was similar in size to the ITA. Moreover, the descending branch of the LCFA is readily accessible and easier to isolate than the internal thoracic artery, gastroepiploic artery and inferior epigastric artery. Lastly, inasmuch as the muscles of the thigh supplied by the descending branch of the LCFA have a rich collateral supply, functional deficits associated with the operation are potentially reduced. Histologically, the LFCA is of the muscular type and contains many smooth muscle cells in the media, similar to the radial artery, inferior epigastric artery and gastroepiploic artery, whereas the ITA has elastic fibers 29 Descending Branch of Lateral Circumflex Femoral Artery Grafting in the media. There is very little difference in the incidence of arteriosclerosis between the LFCA and these arteries. But the LFCA has one disadvantage. The descending branch of the LFCA cannot be used in patients having arteriosclerosis obliterans, because the LFCA may make the important collateral. Therefore the angiogram of lower limb is necessary preoperatively. All patients undergoing CABG using the descending branch of the LFCA had no perioperative or postoperative complications such as myocardial infarction, heart failure or operative death. This showed no increase in perioperative risk with the use of the LFCA graft. The descending branch of LFCA bypass graft offers an acceptable early patency rate. Due to the technical demands involved with descending branch of LFCA harvesting, a learning period may be necessary. Anastomosis of the LFCA graft on the aorta may increase the risk of graft failure, because the wall of the aorta is thicker than the wall of the descending branch of the LCFA. The difference in thickness of their walls made the surgical technique difficult. It is anticipated that use of the descending branch of the LCFA should be extended by using the I or Y grafting technique. In summary, we believe that the descending branch of the LFCA can be used as an autologous graft for myocardial revascularization. References 1. Koshima I, Kawada S, Etoh H, et al. (1995) Flow-through anterior thigh flaps for one-stage reconstruction of soft-tissue defects and revascularization of ischemic extremities. Plast Reconstr Surg 95:252 – 260 2. Song YG, Chen GZ, Song YL (1984) The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Plast Surg 37:149 – 159 3. Koshima I, Fukuda H, Tmamoto H, et al. (1993) Free anterolateral thigh flaps for reconstruction of head and neck defects. Plast Reconstr Surg 92:421 – 428 4. Tanaka Y, Tajima S, Byen M, et al. (1995) Replantation on a large amputated segment of the face: a new technique. Microsurgery 16:594 – 597 5. Rosse C, Rosse PG (1997) Hollinshead’s textbook of anatomy, 5th edn. Lippincott-Raven, Philadelphia, pp 360 – 361 6. Tatsumi TO, Tanaka Y, Kondoh K, et al. (1996) Descending branch of the lateral femoral circumflex artery as a free graft for myocardial revascularization: a case report. J Thorac Cardiovasc Surg 112:546 – 547 237