Survey
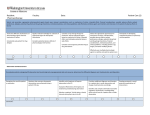
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Rajiv Gandhi University of Health Sciences Bangalore, Karnataka. ANNEXURE-II PROFORMA FOR REGISTRATION OF SUBJECTS FOR DISSERTATION 01 Name of candidate and address (in block letters) OINAM JIMMY DEVI, GHOUSIA WOMEN HOSTEL, BANGALORE DAIRY CIRCLE, BANGALORE-560 029 02 Name of institution AL-AMEEN COLLEGE OF PHARMACY, OPP. LAL BAGH MAIN GATE HOSUR ROAD, BANGALORE- 560 027 03 Course of study and subject M. Pharm Pharmacy Practice 04 Date of admission to course 26th JULY 2010 05 Title of the Topic: “STUDY OF DRUG-DRUG INTERACTIONS IN THE MEDICATION CHARTS IN MEDICINE WARDS AT ST. MARTHA’ S HOSPITAL, BANGALORE”. 6.0 6.1 BRIEF RESUME OF THE INTENDED WORK Need for the study Drug interactions are said to occur when pharmacologic activity of a drug is altered by the concomitant use of another drug or by the presence of another drug or by the presence of food, drinks or environmental chemicals. A large number of drugs are introduced every year, and new interactions between medications are increasingly reported. The interaction may increase (or) decrease the effectiveness of the drug, it also may result in a new side effect. Drug interactions may lead to adverse drug reactions that can be severe enough to necessitate hospitalization. Approximately 37-60% of patients admitted to the hospital may have one or more potentially interacting drug combinations at admission. Drugs can be tools in the prevention and treatment of diseases, but if not used properly, they may be harmful and cause new symptoms (or) produce suboptimal effects. Most drugs have multiple pharmacologic effects in patients, specially the newer, more complex drugs being marketed. Clinically significant drug interactions can occur when two or more drugs are taken in combination.1 Drug-drug interactions (DDI) in patients receiving multi-drug therapy are of wide concern. They may lead to risk of hospitalization and higher health care costs. At least 15% of the patients admitted to hospitals have one DDI at admission. The risk of DDI can increase in the hospital because new drugs are often added to an existing drug therapy. Drug-drug interactions are often predictable and, therefore, avoidable or manageable, but the reactions caused by them are mostly unknown.2 About 5% of all the adverse drug reactions in the hospitals are caused by DDI, the majority of which are advoidable.3 Medicines are often used concomitantly with other drugs, and some degree of drug-drug interactions occurs with concomitant use. Although only a small proportion of this interaction is clinically significant. Therefore, in the evaluation and clinical application of drugs, appropriate efforts should be made to predict the nature and degree of drug interactions so that patients will not be adversely affected.4 The quality use of medicines is a key factor in achieving positive health outcomes. Evidence indicates that there is significant scope for improvement in the use of drugs for hospitalized patients as medication related problems have been identified as contributing to negative clinical and economic outcomes including hospitalization and increased length of stay. The contribution of various members of the healthcare team in improving the medication-related outcomes is less well explored. In developed countries, pharmacists in hospitals frequently initiate changes to patient’s therapy and management. For the purpose of the study an intervention is defined as “any action by the pharmacist that directly results in a change to patient management or therapy”.5 Drug therapy has become so difficult that no single professional is expected to optimize the drug therapy and control drug related problems alone. However, optimization of drug therapy may, by preventing drug related problems, influence health expenses, potentially save lives and enhance patient’s quality of life.6 Hence, this project is proposed to identify drug-drug interactions in the drug therapy by the clinical pharmacist and report the same to the physician so that adverse drug reactions can be prevented and patient outcome can be improved. 6.2 Review of literature A study has been carried out to the physicians expectations to prevent drug interactions in clinical practice. A standard Questionnaire containing 12 Questions regarding prescription writing, importance, experience, training program attended, training needs, source of information, software need and software design for drug-drug interactions were prepared and circulated to 100 doctors of various specialties. The filled Questionnaire were collected and analyzed. 98% of doctors consider drug-drug interaction is an important aspect while writing prescription. 61% of doctors had serious drug-drug interaction experience in their practice.1 A retrospective case-control study (1:1) was performed in 4 months using data of the prescriptions held at the pharmacy of a 300 bed Brazilian teaching hospital. Approximately 11,250 adult inpatients received handwritten prescriptions with two or more drugs prescribed at wards. In randomly selected 887 prescriptions, at least 653 (73.6%) prescriptions presented more than one DDI with different adverse drug reactions, while 234 (26.4%) presented one.2 A study was conducted in the medical wards of the Ospedale Regionale di Lugano, sede Civico, Switzerland. Prescribed drugs from 200 patients at discharge were analyzed for interactions using commercially available software (Pharmavista). Clinical pharmacists and a physician assessed the clinical relevant of detected interactions, eliminated those which were not considered clinically relevant and formulated recommendations for those considered clinically relevant. Among all patients, 62.5% (n=125) had at least one potential DDI, whereas 37.5% (n=75) had no potential drug-drug interaction. In total, 373 potential drug-drug interactions were identified: 223 (60%) of minor severity, 143 (38%) of moderate severity and 7 (2%) of major severity.3 A pharmacoepidemiologic study of drug interactions in a Brazilian teaching hospital has been reported. From 1785 prescriptions studied, at least 1 drug drug interaction was found in 887 prescriptions, which were classified as minor, moderate, major and undetermined. The median number of drugs in each prescription was 7. Drug-drug interactions were identified by using Micromedex, DrugReax System. From the 30 patients with major interactions, 17 presented adverse drug reactions induced by exposure to a major drug-drug interaction. 7 In a study reported at Bou-Ali teaching hospital, Iran, a total number of 3130 prescriptions from in-patients of ICU, CCU, internal and infectious wards were examined during the first 6 months of 2000 and all the potential drug interactions present were extracted and classified in terms of significance, onset, severity and documentation. Among the prescriptions examined 3960 cases and 156 types of interaction were observed.8 A study was conducted with 3 separate population-based, nested case-control studies by linking multiple health care databases over 7 years ( January 1, 1994, to December 31, 2000) in Ontario, Canada to determine whether elderly patients admitted to hospital with specific drug toxicities were likely to have been prescribed an interacting drug in the week prior to admission. 179986 elderly patients treated with glyburide continuously for a total of 431662 patient-years of therapy were admitted to hospital with almost responsible diagnosis of hypoglycemia.9 Pharmacist-initiated changes in drug therapy not only have the potential to save lives, enhance patient’s quality of life and reduce length of stay, but can also be significantly cost-effective. Reduced length of hospital stay and fewer drug-related (re)-admissions are two factors that can be used as indicators of the justification of interventions.10 6.3 Objectives of the study : To attend the ward rounds everyday in Medicine Intensive Care Unit (MICU) and female medical ward of medicine unit I and to collect complete patient history, diagnosis and note down all the medicines prescribed for the patients. To classify all drugs prescribed according to the Anatomical-Therapeutical-Chemical classification (ATC code, WHO 2004). To analyze using various drug information resources for any anticipated or reported drug interaction for the drugs prescribed. In case, any patient is experiencing an adverse drug reaction, to check the prescription for drug interaction and if that is the cause of ADRs. 7.0 Materials and methods 7.1 Source of data : Data will be collected from prospective series of patients' medication charts, who are admitted to the MICU and female general ward of medicine unit I in St.Martha’s hospital, Bangalore during the nine month period of study. Inclusion criteria : Patients who were prescribed with two or more drugs in emergency ward as well as female general ward. To include patients who are on both oral or parenteral medications. Exclusion criteria: All pediatric patients. 7.2 Method of collection of data: The clinical pharmacist will participate in the ward rounds conducted in MICU and female general ward of medicine unit I. The pharmacist will make note of complete patient details, diagnosis, co-morbid conditions, laboratory values and drugs prescribed with their doses and frequency of administration. Then it will be analyzed for any reported drug interactions between the drugs prescribed. If any patient is experiencing an adverse drug reaction, the clinical pharmacist will check whether it is due to drug-drug interactions. The pharmacist will report to the physician incharge the findings of the data analysis. 7.3 Duration of study The study will be conducted for a period of 9 months. 7.4 Does the study require any investigation or intervention to be conducted on patients or other humans? No. 7.5 Has ethical clearance been obtained from your institution in case of 7.3? The project will be submitted to the Institutional Review Board of St. Martha’s hospital for ethical clearance and the same will be submitted to the university. 8.0 References: 1. Satish A, Bhaskar H. Physician expectation to prevent the drug interactions in clinical practice. Int Jour Pharm and Pharmaceut Sci; 2(3):172-73. 2. Joice MCS, Carlos JT. Prevalence of potential drug-drug interactions and its associated factors in a Brazilian teaching hospital. J Pharm Pharmaceut Sci 2006; 9(3):427-33. 3. Bertoli R, Bissigb M, Caronzoloc D, Odoricod M, Pons M, Bernasconi E. Assessment of potential drug-drug interactions at hospital discharge. Swiss Medical Weekly 2010 March. Available from URL: http://smw.ch/docs/PdfContent/smw-12979.pdf. 4. Flockhart DA. Methods of Drug Interaction Studies.2009 Jan. Available from URL: http://nihs.go.jp/phar/material3/DiGIEngFinal011209. 5. Alagiriswami B, Ramesh M, Parthasarathi G, Basavanagowdappa H. A study of clinical pharmacist initiated changes in drug therapy in a teaching hospital. ijopp 2009 Jan; 1(2):36-45. 6. Dooley MJ, Allen KM, Doecke CJ, Galbarth KJ, George TR, Jennifer B et.al. A prospective multicentre study of pharmacist initiated changes to drug therapy and patient management in acute care government funded hospitals. Br J Clin Pharmacol 2003 Oct; 57(4): 513-21. 7. Cruciol-Souza JM, Thomson JC. A pharmacoepidemiologic study of drug interactions in a brazilian teaching hospital Clinics 2006; 61(6):515-20. 8. Giti H, Alireza SM. An Investigation of Drug Interaction in Hospital Pharmacy Prescription. IJPR 2002 July; 1:15-19. 9. David NJ, Mamdani M, Alexander K, Andreas L, Donald AR. Drug-drug interactions among elderly patients hospitalized for drug toxicity. JAMA 2003 Apr; 289(13):165258. 10. Struck P, Kristine PH, Moodley P, Rasmussen M. A pilot study of pharmacist-initiated interventions in drug therapy in an Australian paediatric hospital. EJHP Science 2007; 13(4):105-12. 9.0 Signature of the candidate 10.0 Remarks of the Guide Recommended for research and submission of dissertation 11.0 Name & Guide Dr. Shobha Rani R Hiremath Professor and Head Department of Pharmacy Practice Al-Ameen College of Pharmacy Bangalore-560 027 Signature 12.0 Co – Guide Dr. Indira Ramaiah Senior Consultant and Unit Head (UNIT I) Department of Medicine St.Martha’s Hospital No.5 , Nrupathunga Road Bangalore-560 001 Signature 13.0 Head of the Department Dr. Shobha Rani R Hiremath Professor and Head Department of Pharmacy Practice Al-Ameen College of Pharmacy Bangalore-560 027 Signature 14.0 Remarks of the Principal Forwarded for approval 15.0 Principal Prof. B.G. Shivananda Principal Al-Ameen College of Pharmacy Bangalore-560 027 Signature