Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
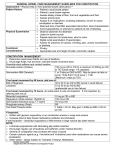
GIT Fall Semester Nur 221 Anatomy overview of the GIT Function of the GIT: - Breakdown of food for digestion - Absorption of nutrients produced by digestion into the bloodstream - Elimination of undigested foodstuffs and other waste products Assessment of the GIT Health Hx and clinical manifestation: - Pain (Abdominal) - Dyspepsia (indigestion) - Intestinal gas (belching , flatulence) - N&V - Changing in bowel habit and stool ch.ch (diarrhea, constipation - jaundice, history of GI surgery or problems, appetite and eating patterns, teeth, and nutritional assessment including weight patterns PE & Diagnostic procedure Psychosocial, spiritual, and cultural factors Common Sites of Referred Abdominal Pain Diagnostic test: - CBC, PT,PTT, LFT, S.amylase, billirubin, stool analysis Breath test (hydrogen breath test, urea breath test) Abd U\S Imaging studies: CT, MRI Upper Gastrointestinal Tract Study (barium meal) Lower Gastrointestinal Tract Study (Barium enema) Endoscopic procedures (gastroscopy) Colonoscopy Quadrants of the Abdomen Gastritis Inflammation of gastric and stomach mucosa Acute: rapid onset of symptoms - usually caused by dietary indiscretion. FOOD irritating … highly seasoned or contaminated by microorganism. - Other causes include overuse of medications (aspirin & NSAID), alcohol, bile reflux, and radiation therapy. - Ingestion of strong acid or alkali. Chronic- prolonged inflammation: due to benign or malignant ulcers, or by helicobacter pylori (H. pylori), Can be due to autoimmune disease as pernicious anemia, dietary factors (caffeine), medications NSAID, alcohol, smoking, chronic reflux of pancreatic secretions or bile Pathophysiology: gastric mucus membrane is edematous and hyperemic (congested with fluid &blood) & may perforated. Very little acid and a much mucus is secreted. superficial ulceration may occur & cause hemorrhage Symptoms: - For acute gastritis: Abd discomfort, headache, lassitude, nausea, vomiting, anorexia, hiccupping, feeling of fullness. - In chronic gastritis: Anorexia, heartburn after eating, belching, sour taste in the mouth, nausea and vomiting, intolerance of some foods, May have vit. B12 deficiency due to malabsorption Assessment & Dx finding: - hypochlorhydria (↓HCl) or hyperchloridria (↑HCl), or achlorhydria - diagnosis made by: UGI x-ray series, endoscopy & biopsy, histological examination of tissue specimen, CBC, stool for occult blood Medical management: - In acute gastritis: may heal by it self in 1 day, with anaroxia for 2-3 days, it also treated by refrain pt from alcohol & food until symptoms subside nonirritating diet is recommended Supportive therapy (NGI; IV fluid; antiacid; Sedative If hemorrhage present (blood transfusion with fluid replacement) Neutralize and dilute the agent if the cause is acid or alkali ingestion, avoid emetics and lavage due to danger of perforation and damage to esophagus *In sever cases surgery is performed (gastrojejunostomy) - For chronic gastritis: modifying the patient's diet promoting rest, reducing stress, recommending avoidance of alcohol and NSAIDs & smoking initiating pharmacotherapy (drug combinations) (e.g. antibiotics; H2 blocker, proton pump inhibitors) Nursing process for pt with gastritis Assessment: - History including presenting signs and symptoms + symptoms occur at any specific time of the day + & factor+ association. Dietary history and dietary associations with symptoms (72 hour diet) - Identifies duration of symptoms, any methods used by pt to treat it, & if the methods are effective - Physical examination include abdominal tenderness, dehydration, and evidence of any systemic disorder that might be responsible for the symptoms of gastritis - Result of diagnostic procedure Diagnosis: - Anxiety related to treatment - Imbalanced nutrition, less than body requirements, related to inadequate intake of nutrients - Risk for imbalanced fluid volume related to insufficient fluid intake and excessive fluid loss subsequent to vomiting - Deficient knowledge about dietary management and disease process - Acute pain related to irritated stomach mucosa Planning: - Reduced anxiety - Avoidance of irritating foods - Adequate intake of nutrients - Maintenance of fluid balance, - Increased awareness of dietary management - Relief of pain. Implementation: - Reducing Anxiety : offers supportive therapy to the patient and family during treatment and after the ingested acid or alkali has been neutralized or diluted uses a calm approach to assess the patient and to answer all questions as completely as possible explain all procedures and treatments based on the patient's level of understanding. - Promoting Optimal Nutrition: N.P.O possibly for a few days—until the acute symptoms subside monitors fluid intake and output along with serum electrolyte values After the symptoms subside, offer ice chips followed by clear liquids Introducing solid food as soon as possible discourages the intake of caffeinated beverages, because caffeine is a central nervous system stimulant that increases gastric activity and pepsin secretion Discouraging cigarette smoking (nicotine reduce the secretion of pancreatic bicarbonate which inhibit neutralization of gastric acid) - Promoting Fluid Balance : Daily fluid intake and output are monitored be alert for any indicators of hemorrhagic gastritis, which include (hematemesis : vomiting of blood), tachycardia, and hypotension IVF administration and monitoring - Patients Teaching: inform about stress management, diet, and medications Dietary instructions take into account the patient's daily caloric needs, food preferences, and pattern of eating review foods and other substances to be avoided (e.g., spicy, irritating, or highly seasoned foods; caffeine; nicotine; alcohol). Describe medication regimen. Peptic Ulcer Disease A peptic ulcer may be referred to as a gastric, duodenal, or esophageal ulcer, depending on its location Excavation (hollowed-out area) that forms in the mucosal wall of the stomach, in the pylorus (the opening between the stomach and duodenum), in the duodenum (the first part of small intestine), or in the esophagus more likely to be in the duodenum than in the stomach Peptic ulcer disease occurs with the greatest frequency in people between 40 and 60 years of age uncommon in women of childbearing age, After menopause, the incidence of peptic ulcers in women is almost equal to that in men result from infection with the gram-negative bacteria , which may be acquired through ingestion of food and water Other causes for peptic ulcer are: stress, caffeinated beverages, smoking, and alcohol, eating spicy foods may make peptic ulcers worse. Familial tendency also may be a significant predisposing factor. People with blood type O are more susceptible to peptic ulcers than are those with blood type A, B, or AB Other predisposing factor chronic use of NSAID’s, alcohol ingestion and smoking severe peptic ulcers, extreme gastric hyperacidity, and gastrin-secreting benign or malignant tumors of the pancreas known as Zollinger-Ellison syndrome (ZES) Deep peptic ulcer ZES (Zollinger-Ellison syndrome): - suspected when a patient has several peptic ulcers or an ulcer that is resistant to standard medical therapy - identified by the following: hypersecretion of gastric juice, duodenal ulcers, and gastrinomas (islet cell tumors) in the pancreas (↑release the hormone gastrin) - The most common symptom is epigastric pain - H.Pylori is not a risk factor for ZES Stress ulcer: - acute mucosal ulceration of the duodenal or gastric area that occurs after physiologically stressful events, such as burns, shock, severe sepsis, and multiple organ traumas - endoscopy within 24 hours of trauma or surgery reveals shallow erosions of the stomach wall; by 72 hours, multiple gastric erosions are observed. - Mechanism: in shock gastric mucosal blood flow decrease and the duodenal content reflux to stomach increase, and amount of pepsin secretion increase ( ischemia + increase acid and pepsin creates an ideal climate for ulceration) Pathophysiology peptic ulcers mainly occur in gastroduodenal mucosa. Damaged mucosa cannot secrete enough mucus to act as a barrier in addition increase acid and pepsin will cause further damage to the mucosa and decrease resistance to bacteria C\M dull pain or a burning sensation (gnawing) in the midepigastrium or in the back Pain is usually relieved by eating in duodenal ulcer, while increase in pt with gastric ulcer localized tenderness in the epigastric area pyrosis (heartburn), vomiting, constipation or diarrhea, and bleeding Melena, hematomesis Assessment and Diagnostic Findings physical examination may reveal pain, epigastric tenderness, or abdominal distention barium study of the upper GI tract may show an ulcer endoscopy is the preferred diagnostic procedure because it allows direct visualization of inflammatory changes, ulcers, and lesions Stools analysis Gastric secretory studies to evaluate a chlorhydria Pathogenic/histological examination (for H.pylori) serologic testing for antibodies against the antigen urea breath test Management Medications (combination of antibiotics, proton pump inhibitors, and bismuth salts that suppress or eradicate, for 10 to 14 days lifestyle changes surgical intervention (vagotomy, Pyloroplasty, Gastrojejunostomy) Smoking cessation, stress reduction Diet modification Management surgical intervention: 1. Pyloroplasty: a surgical procedure in which the pylorus valve at the lower portion of the stomach is cut and resutured, relaxing and widening its muscular opening (pyloric sphincter) into the duodenum 2. vagotomy: disconnecting the nerves that stimulate acid secretion and opening the pylorus), The purpose of the procedure is to disable the acid-producing capacity of the stomach. 3. Gastrojejunostomy 30 Surgical Procedures for Peptic Ulcers Question Is the following statement True or False? The most common site for peptic ulcer formation is the pylorus. Answer False The most common site for peptic ulcer formation is not the pylorus. The most common site for peptic ulcer formation is the duodenum. Nursing process Assessment: - Assess pain & method to relive it - Assess vomiting - Assess pt usual food intake - Assess pt intake of medication - V\S - Review result of the diagnostic test - P\E for abdominal tenderness Nursing Diagnoses: - Acute pain related to the effect of gastric acid secretion on damaged tissue - Anxiety related to an acute illness - Imbalanced nutrition related to changes in diet amb decreased weight, decreased required caloric intake/24hs - Deficient knowledge about prevention of symptoms and management of the condition Collaborative Problems/Potential Complications: - Hemorrhage Perforation Penetration Pyloric obstruction (gastric outlet obstruction) Intervention: - Medication to relive pain - Instruct pt to avoid aspirin, caffeinated beverage, spicy food - Relaxation technique to manage pain and stress - Encourage pt to express fear - Explain any procedure to the pt - Manage complication ( blood transfusion, monitor V\S, IVF) - Instruct the pt about factors that decrease or increase the condition - Teach the pt about the diet Abnormalities of fecal elimination Abnormalities in fecal elimination are symptoms of functional disorders or disease of the GI tract. It include constipation, diarrhea and incontinence Constipation It is abnormal hardening of stools that makes their passage difficult and sometimes painful, a decrease stool volume, or retention of stool in the rectum for a prolonged period Causes: - Medication (anticholinargeic, antidepressant, iron preparation, antihypertensive, opioid analgesic) - Rectal or anal disorders (hemorrhoids) - Obstruction (bowel tumor) - Metabolic, neurologic and neuromuscular condition as ( DM, MS) - Endocrine disorder (hypothyroidism) - Lead poisoning and connective tissue disorders (SLE) Other causes: weakness, immobility, emphysema, dietary habit, lack of exercise, stress, chronic laxative use Irritable bowel syndrome & diverticular are common disease of the colon associated with constipation Pathophysiology Interference with one of the following: 1- mucosal transport ( mucosal secretion that facilitate the movement of colon content) 2- myoelectric activity( mixing of the rectal mass and propulsive action) 3- process of defecation Any causes of the constipation can interfere with these three processes If no any organic causes for constipation idiopathic constipation is diagnosed C\M: - Decrease bowel movement <3\wk Abdominal distension Pain & pressure Headache dec appetite Fatigue indigestion, strain at stool & elimination of small volume and hard-dry stool - Sense of incomplete evacuation Diagnosis Pt Hx Physical examination Barium enema or sigmiodscopy (to assess is it from spasm or narrowing of the bowel) Anorectal manometry: measure the changes in intraluminal pressure and coordination of muscle activity in GIT(to assess malfunction of the sphincter, rectosphincteric reflex.) Defography: instillation of very thick barium into the rectum then fluoroscopy done while the pt. is trying to expel the barium, evaluation for the function of the rectum and anal sphincter Complications: HTN, fecal impaction, hemorrhoids and fissure, megacolon (enlarged colon that is unable to move stool) Medical Managements: aim to correct the underlying cause by: - Education to increase fiber diet and fluids - Bowel training habits and discontinuing of laxative use. - Routine exercise that strengthen abdominal muscles - Biofeedback is a technique used to help patient learn to relax the sphincter mechanism to expel the stool. - 6-12 teaspoon of unprocessed bran. - If laxative to be used; use bulk forming agents, saline and osmotic agents, lubricants, stimulants, fecal softeners. - Enemas and rectal suppositories used for patient with fecal impaction Nursing management: - Pt education how to prevent constipation: Respond to urge to defecate Dietary information Increase ambulation and exercise Describe abdominal toning exercise ( contracting Abd muscle 4t\day and leg to chest left 10-20t\day) Instruct patient about semisquatting position during defecation Diarrhea increase frequency of bowel movement (> 3 per day), increase amount more than 200 g per day, altered consistency (looseness) of stool. Associated with urgency, perianal discomfort, incontinence. Any condition that causes ↑ intestinal secreration, ↓ mucosal absorption, or alteration in motility can cause diarrhea It may be acute or chronic Causes (IBS, IBD, lactose intolerance) the main underlying disease that cause diarrhea. It occurs also from Medications as ( thyroid hormone replacement, laxative, AB, chemotherapy) Tube feeding formula Metabolic and endocrine disorders (DM, thyrotoxicosis) Viral or bacterial infection (food poisoning, dysentery) Nutritional and malabsorpative disorders (celiac) Anal sphincter defect ZES, paralytic ileus, intestinal obstruction, AIDS Pathophysiology: - 3 types: 1- Secretory: (high-volume diarrhea, caused by production and secretion of water and electrolyte by intestinal mucosa 2- Osmotic: (due to water pulling into the intestine by the osmotic pressure from unabsorbed particles) 3- Infectious 4- Malabsorption 5- Exudative C\M: increase frequency and fluid content of stools, Abd cramp, distention, intestinal rumbling (borborygmus), anorexia, thirst. Painful spasmodic contraction of the anus and ineffective straining (tenesmus). Other symptoms are due to dehydration and electrolyte imbalance Greasy stool suggest intestinal malabsorption; presence of mucus and pus suggests inflammatory enteritis or colitis. Oily droplet are almost indicate pancreatic insufficiency, nocturnal diarrhea may suggest diabetic neuropathy Diagnosis: CBC, chemistry, urinalysis, routine stool examination, and stool exam for infectious or parasitic organism, Barium enema and endoscopy Complications: Dysrthymias, Muscle weakness, drowsiness, anorexia, loss of fluid cause urine output less than 30 ml/day. Dec K+ level less than 3 mmol/l should be reported Medical management: use of AB and antiinflammatory agent to reduce the severity & treat the underlying disease Nursing management: assessment, in acute episode encourage bed rest and food and fluid low in bulk, solid food followed, avoid caffeine beverages & very hot or cold foods, restrict milk products, fat, fresh fruit and vegetables for several days, administer antidiarrheal medication (diphenoxylate or loperamide), IVF, report evidence of dysrhythmias that may result from hypokalemia IBS Functional disorders of intestinal motility No known cause, usually hereditary factor, psychological stress, depression and anxiety, diet high in fat and stimulating or irritating food, alcohol consumption and smoking. More common in women than in men In IRS the peristaltic waves are affected at specific segments & the intensity of propel the fecal pattern, no evidence of inflammation or tissue changes in intestinal mucosa C\M: Alteration in bowel pattern (primary symptoms) constipation or diarrhea or mixing of both, abdominal pain ( ↑ with eating & ↓ with defecation) , bloating, abd distension Diagnosis: Stool studies, contrast X-ray, Barium enema, colonoscopy (spasm), proctoscopy, manometry, and electromyography study the intraluminal pressure changes generated by spasm Medical management: Restrict food and then reintroduction of foods is important to determine type of food that is irritating (beans, caffeinated products, fried food, alcohol, spicy food) Stress reduction techniques Manage diarrhea and constipation Tegaserod (zelnorm) for women with IBS and complain from constipation, but it was not recommended lately due to the risk of MI Probiotics can be given Dietary complement Nursing management: Nurse should educate family and patient about the importance of good dietary habits, chewing food slowly and eat regularly, not taking fluid with meal since it may cause abd destination, discouraged alcohol and smoking. Acute inflammatory intestinal disorders Appendicitis: (inflammation of the appendix) - Appendix is a small, finger-like structure within the abd, about 10 cm long and attached to the cecum just below the ileocecal valve - fills with food and empties into the cecum - It is prone to obstruction and to infection (appendicitis) - Common cause of acute abd, and emergency abdominal surgery - Occur in all ages but it common between age 10-30 years Pathophysiology: - It become inflamed and edematous either by being kinked or occluded by fecalith, tumor or Foreign body - Inflammatory process increases intraluminal pressure, initiating progressively sever and generalized or periumblical pain that becomes localized in the RLQ - When it flamed it filled with pus C\M: - vague epigastric pain or periumblical pain that progress to the RLQ - associated with low grade fever, N & V - loss of appetite - Localized tenderness at the Mc Burney’s point ( point between the umbilicus and the anterior superior iliac spine - +ve rebound tenderness ,+ve rovsing sign, +ve obtirator, & psoas sign, and cutaneous hypersthesia - If it rupture pain become more diffuse, with the development of abdominal distention - Constipation may occur, so pt not given laxative Diagnosis: - Complete P\E - Lab test (CBC, urine analysis) - Abd x-ray, U\S and CT scan (reveal RLQ density or localized distension of the bowel Complications: - Perforation (peritonitis): occur 24hr’s from pain onset - Abscess formation - Portal pylephlebitis Medical management: - Immediate surgery (Appendectomy) - AB pre op - If it perforated drainage is applied to the abscess, then appendectomy is performed Nursing management: - Pre surgery - Relive pain - Prevent FVD - Reduce anxiety - Prepare the pt for surgery - After surgery :place pt in high fowler position or supine with leg slightly flexed - Give pt opioid analgesic Give food as tolerated Teach pt wound care Instruct pt that he can resume normal physical activity within 24wk’ Nursing interventions for patient with complications after appendectomy: - Peritonitis: observe for abd tenderness, fever, vomiting, abd rigidity and tachycardia, employ constant NG tube, correct dehydration, administer antibiotic - Pelvic abscess: evaluate N & V, chills, fever, diaphoresis, diarrhea, prepare pt for rectal exam and surgical drainage, - Subphrenic abscess (under the diaphragm): evaluate for chills and fever, prepare x-ray exam, prepare pt for surgical drainage of abscess. - Paralytic ileus: assess for bowel sounds, employ NG tube and suction, replace F& E, prepare for surgery Peritonitis: - An inflammation of the peritoneum, the serous membrane lining the abd cavity and covering the viscera. - Results from bacteria (E.Coli, klebsiella, Proteus& pseudomonas) or MO from GI disease, in women it occur from disease of reproductive organ. It can result from trauma or injury (gunshot, stab wound) or kidney inflammation. - Other common causes are: appendicitis, perforated ulcer, diverticulitis and bowel perforation, peritoneal dialysis Pathophysiology Occurs when abd organ content leak into the abd cavity as a result of inflammation, infection, trauma, tumor & perforation. Result in edema & exudation of fluid. Fluid in the abd cavity becomes turbid and then increasing amount of protein and cellular debris, blood, WBC, intestinal tract responded immediately by hypermotility followed by paralytic ileus with fluid and gas accumulation in the bowel and. C\M: depends on the severity and location of inflammation - Diffuse pain (then becomes constant, localized, more intense near the site of inflammation, ↑with movement) - Then becomes sever tenderness and distention in the affected area - Rebound tenderness & paralytic ileus - N&V, increase temp (37.8- 38.3), increase pulse rate - Diminished peristaltic movement - Rigid abdominal muscle Pain diminished in pt with diabetes, liver cirrhosis and on analgesic or corticosteroids Diagnostic finding: - ↑ WBC’s - ↓ Hb & HCT if blood lost occurred - ↓ Na, K, Cl - Abd x-ray: air, fluid & distended bowel - CT scan show abscess formation - Peritoneal aspiration for culture and sensitivity. - Complications: Sepsis (major cause of death ) Shock due to hypovolemia or septicemia Intestinal obstruction (due to bowel adhesion) Medical management: Fluid and electrolyte replacement. Isotonic solution is administered (several liters) to correct hypovolemia Analgesic for pain Antiemetic as prescribed for N & V Intestinal intubations and suction decrease distension and promote intestinal function. O2 therapy is administered Massive antibiotic therapy: large doses of broad spectrum antibiotic through IV. Surgery is aimed to remove the infected material and correct the cause: excision (appendix), repair (perforation) & drainage (abscess) Nursing management: pt is in ICU - Monitor VS, GI function, F & E balance, urine output - Assessment of pain - Positioning (place pt on the side with knee flexed) - Record I&O - Administer and monitor IVF - Assess signs of ↓ peritonitis: ↓ temp, pulse rate, softening of the abdomen, return of peristaltic sounds, passing of flatus, and Bowel movement - Increase food and fluid intake gradually as needed - Observe and record the ch.ch of the drainage - Teach pt & family how to care for the drain and the wound if he will discharge with them Intestinal obstruction Presence of blockage that prevents the normal flow of intestinal contents through the intestinal tract 2 types: 1- Mechanical: it is an intraluminal or mural obstruction from pressure on the intestinal wall (as tumors & neoplasms, intussusceptions, hernias, stenosis, abscess, adhesion) 2- Functional: the intestinal musculature cannot propel the content along the bowel [as muscular dystrophy, endocrine (DM), neurological (Parkinson's disease)], can be temporary when the bowel is manipulated due to surgery Causes of Intestinal Obstructions Obstructions can be partial or complete Its severity depends on: - The region of obstruction - The degree of obstruction - The degree to which vascular supply disturbed Most bowel obstruction occur in the small intestine ( adhesion then hernias and neoplasms), other causes intussusceptions, volvulus, paralytic ileus. Most obstruction of the large bowel occur in sigmoid colon, common causes are carcinoma, diverticulitis, IBD, benign tumor. . Intussusception: invagination or shortening of the colon caused by movement of one segment of the bowel into another. Volvulus of the sigmoid colon: twisted and with edematous bowel Hernias: herniated intestinal content (inguinal hernia). 82 Small bowel obstruction Intestinal contents, fluids & gas accumulate above the intestinal obstruction →Abdominal destination & retention of fluid → ↓absorption of fluid → stimulate more gastric secretion. With ↑ing destination → ↑intestinal pressure → ↓venous & arteriolar pressure → Edema, congestion, necrosis, perforation or rupture of the intestinal wall; peritonitis may occur Metabolic alkalosis (reflux vomiting → loss of H+ & K ions (stomach)→ ↓ Cl& K (blood)→ MA) Dehydration and acidosis (Rt loss of H2O and Na). Hypovolemic shock may occur due to acute fluid losses Signs and symptoms: initially crampy pain & colicky. Pt may pass blood & mucus but not fecal matter or flatus. Vomiting. If obstruction complete, intestinal content propelled toward the mouth instead of the rectum (due to reverse direction of extremely vigorous peristaltic movement). Obstruction of the ileum: fecal vomiting: starting with vomiting of stomach content → bile-stained content of the duodenum & jejunum → darker fecal-like content of the ileum. Dehydration signs: intense thirst, drowsiness, malaise, aching, parched (dry) tongue & mucous membrane. The more lower the GI obstruction the more abdominal distention occurs. End result ….hypovolemic shock (RT dehydration & loss of plasma volume). Diagnosis: S&S, x-ray (abnormal quantities of fluid and gas), lab studies for (electrolyte &CBC: for signs of dehydration). Medical management: NG tube (NGT) for decompression of the bowel. Surgery (in complete obstruction) as: repairing the hernias, dividing the adhesion, or removal of affected part and making anastomosis. Nursing management: Maintain the NGT function; measure/assess its output, Assess: F&E, nutritional status, passage of stool or flatus, return of bowel sounds, improvement in the Abd pain. Report: ↑ in pain or abd distension, ↑NGT output and prepare pt for surgery Large bowel obstruction Accumulation of intestinal contents, fluid and gas proximal to the obstruction. Cause sever destination and perforation unless release of some fluid and gas through the ileal valve. In sever obstruction→ cut off blood → necrosis (life threatening). Dehydration occur more slowly because colon can distend beyond its normal capacity and absorb its fluid content. Slow progression of symptoms. C\M: - If sigmoid colon and rectum obstructed →only constipation can be seen for months. - Blood loss in stool → iron deficiency anemia - Distended abd → visible loops of large intestine through the abdomen - Crampy lower Abd pain develop - Fecal vomiting and shock may occur. Diagnosis: - S&S - Imaging studies (X-ray, Abd CT, MRI): distended colon **Barium study is Contra Indicated Medical management: - Correction of F&E, NGT for immediate aspiration & decompression Colonoscopy: to untwist & decompress the bowel Rectal tube to decompress the lower area of the bowel Surgery to resects and remove the obstructed lesion Cecostomy to release gas and small amount of drainage - Colostomy (temporary or permanent), - Ileoanal anastemosis (if the entire large bowel removed) Nursing management: - Monitor pt for worsening in obstruction - Administer IVF and electrolyte replacement - Prepare the pt for surgery if indicated Colostomy Is the surgical creation of an opening into the colon , allows the drainage of colon It could be content to the out side the body. temporary or permanent fecal diversion. The consistency of the drainage is related to the placement of the colostomy. Large bowel obstruction, Indications : Colorectal cancer. The colostomy begins to function 3- 6 days after surgery. Ileostomy Ileostomy: the surgical creation of an opening into the ileum or small intestine, is commonly performed after a total colectomy. It allows for drainage of fecal matter from ileum to the out side of the body The drainage is liquid to unformed and occurs at frequent intervals. Indication: chronic inflammatory bowel disease. Nursing Management - Stoma care ( see chart 38-5 changing an ostomy appliance) & ( See chart 38-11 the irrigation procedure) - Teaching patient self care - Supportive a positive body image - Continuing care. Diseases of the Anorectum Includes: Anorectal abscess, Anal fistula, Anal fissure, hemorrhoids, pilonidal sinus or cysts. Anal fissure: - Is a longitudinal tear or ulceration in the lining of the anal canal - Causes: trauma, persistent tightening of the anal canal from stress and anxiety (constipation), childbirth, overuse of laxative - C\M: painful defecation, burning and bleeding during defecation, bright red on the paper toilet - Rx: dietary modification ( fiber supplement), stool softener, increase water intake, sitz bath, suppositories with analgesic, surgery ( lateral internal shpinctretomy with fissure excision) - - Hemorrhoids Dilated veins in the anal canal 50 % of people above 50y of age develop hemorrhoids. Shearing effect on the anal mucosa during defecation leading to sliding of the anal structure ( hemorrhoidal and vascular tissue) Pregnancy may initiate it due to the pressure in the hemorrhoidal tissue Classifies as: internal or external S&S: pain, itching, bright red bleeding with defecation External: associated with sever pain from inflammation and edema caused by thrombosis lead to ischemia and necrosis. Internal is not painful until they bleed or prolapsed when they enlarge Management: avoid strain, hygiene, high-fiber diet, fruit, bran and fluid intake. Analgesic, bulk-forming agents such as (Metamucil),, warm compresses, sitz bath, bed rest allow the engorgement to subside. None surgical treatment: infrared photocoagulation, bipolar diathermy, laser therapy (to affix the mucosa to underling muscle) . Surgical treatment: rubber-band Ligation procedure after anoscope. Can be painful and may cause secondary hemorrhage or infection. Cryosurgical hemorrhoidectomy: freezing the hemorrhoid for sufficient time to cause necrosis, painless, foul smelling, prolonged healing, not very common. For hemorrhoids with thrombosed vein hemorrhoidectomy is performed, after surgery small tube inserted through the sphincter to permit flatus and blood drainage Nursing process Assessment: Nsg Dx: - Constipation R\T ignoring the urge to defecate secondary to pain - Anxiety R\T surgery or embarrassment - Acute pain R\T irritation, pressure - Knowledge deficit Potential complication: hemorrhage Planning: relive constipation, relive pain, anxiety, increase knowledge Implementation: - Encourage fluid intake - High fiber diet recommendation - Instruct pt how to use bulk agent - Give analgesic before bowel movement - Relaxation exercise - Inform pt not to ignore the urge to defecate Explain surgical procedure - - Maintain pt privacy during care of the pt - Sitz bath of warm water to relive pain 3-4t\day after each bowel movement for 1-2 wk post surgery - Use of topical analgesic agent (xylocaine) - Place pt in prone position ( reduce edema of the tissue) - Check area for rectal bleeding - Monitor urine output