Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
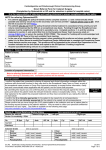
Cambridgeshire and Peterborough Clinical Commissioning Group Direct Referral Form for Cataract Surgery Patient’s Name: GP’s Name: Optometrist’s Name: Address: Address: Address: Postcode: Tel No: NHS No: Postcode: Tel No: Postcode: Tel No: DOB: Reason for referral / symptoms/ likely functional benefit of surgery: Ocular Co-morbidity / POH: Rx Current Previous R Sph. Cyl. Axis BC VA L Sph. Cyl Axis BC VA Add CCG Referral Threshold met?1 BCVA ≤6/12 or worse in worst eye; YES/NO OR bilateral cataracts, binocular vision does not meet DVLA standards; OR significant optical imbalance (anisometropia or anisekonia) YES/NO affecting activities of daily living only corrected with cataract surgery; AND patient willing to undergo surgery. YES/NO Cataract Grade Clear R L Clear Nuclear Nuclear mild / mod / severe mild / mod / severe Cortical Cortical mild / mod / severe mild / mod / severe PSC PSC mild / mod / severe mild / mod / severe Pseudophakia Pseudophakia List for cataract surgery in right or left eye? Blepharitis: Yes /No. A/C depth: Deep / Shallow. Pupil dilates well: Yes / No. Difficult fundoscopy: Yes / No. RAPD present: Yes / No. Cornea: L: R: Indicate if opacity IOP: mmHg R: mmHg L: Disc: L: R: Indicate cup-disc ratio Fundus: L: R: Indicate macular status Medical History (to be completed by the Optometrist). Circle Yes/No below appropriate. Diabetes: Yes / No. Hypertension: Yes / No. Heart attack: Yes / No. Stroke: Yes / No. Short of breath: Yes / No. Poor mobility: Yes / No. Is able to lie down flat: Yes / No. Current Drugs: Choice of care provider Social History: (eg driver, working, carer) Other: Transport needed? Yes / No Written information provided? Yes / No Patient Consent Is the patient aware of this referral and the content of this form, and any supporting documents? I confirm the patient has consented to the sharing of personal and clinical information contained within this form with clinical staff involved with their care to enable full consideration of this referral. By submitting this referral you are confirming that you have fully explained to the patient the proposed treatment and they have consented to you raising this referral on their behalf. Optometrist’s signature: ___________________________________ Circle as appropriate Yes / No Yes / No Date: _____________ Date: ____________________________________ Copes to be printed: (Please circle once printed): Care Provider Copy / Patient Copy / GP Copy / Optometrist Copy 1 For patients who do not meet the policy threshold, treatment is considered of low priority and will only be commissioned by the NHS on an exceptional case basis. Optometrists or GPs need to apply to the Exceptional and Individual Funding Request Panel for approval of funding. Click the links to access the CCG Cataract Policy and Exceptional/Individual Funding Request Form: Policy; Funding Rqst Frm Doc Ref R:/CPF Pols & working Area/Surg Threshold Pols - Draft and Agreed/referral pfrma/cataract/ CATARACT REFERRAL PROFORMA MAY 14 V5 May 2014