Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
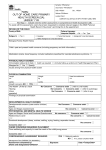
REQUEST FOR CONSULTATION GOLD COAST HOSPITAL AND HEALTH SERVICE HEART HEALTH SCREENING CLINIC Chronic Disease Wellness Program Specialising in Community based multidisciplinary care for Patients with complex care needs Supporting Team Care Arrangements (does not utilise Medicare items) Aboriginal and Torres Strait Islander Early Intervention and Chronic Disease Management Services Prof Rohan Jayasinghe SEND TO: Central Intake Unit Fax: 1300 668 536 OR Phone: 1300 668 936 OR Secure Transmission Via Medical Objects to: QHEALTH, GOLD COAST HEALTH Adult Community Health Central Intake Unit FROM: <<Doctor:Name>> <<Practice:Name>> Address: <<Practice:Address>> Phone:<<Practice:Phone>> Fax: <<Practice:Fax>> Email: <<Doctor:E-mail>> Provider Number: <<Doctor:Provider Number>> Signature Does the Patient identify as being of Aboriginal and/or Torres Strait Islander descent? <<Does the pt identify as A and/or TSI>> (If no, this Patient is ineligible for this service) This service is for Patients 18 years and older. I wish to send this Patient to The Aboriginal and Torres Strait Islander Heart Health Screening Clinic An early intervention Cardiac Screening Clinic that includes a Cardiology consultation targeting Aboriginal and/or Torres Strait Islander community members with high cardiovascular risk factors including: Risk Factors: Smoker (current)? Smoking quitting stage? Consumes alcohol? Physical inactivity? Work environment mostly sitting? Social isolation? Diabetes? High blood cholesterol? Hypertension? Depression? <<Clinical Details:Smoking>> <<Clinical Details:Smoking Quitting Stage>> <<Clinical Details:Alcohol>> <<Is the Patient physically inactive?>> <<Is the Patient's work environment mostly sitting?>> <<Is the Patient socially isolated?>> <<Does the patient have diabetes?>> <<Does the Patient have high blood cholesterol?>> <<Does the Patient have hypertension?>> <<Does the Patient have depression?>> Date: <<Miscellaneous:Date>> Dear Prof Rohan Jayasinghe RE: <<Patient Demographics:Full Name>> Date of Birth: <<Patient Demographics:DOB>> Gender: <<Patient Demographics:Sex>> Medicare Number*: <<Patient Demographics:Medicare Number>> *[Medicare ineligible patients will incur an appointment fee] Address:<<Patient Demographics:Full Address>> Home Ph: <<Patient Demographics:Phone (Home)>> <<Patient Demographics:Full Name>> <<Patient Demographics:DOB>> Developed in partnership by General Practice Gold Coast, Gold Coast Primary Health Network and Gold Coast Health January 2016 Mobile Ph: <<Patient Demographics:Phone (Mobile)>> Alternative Contact Name: <<Alternative Contact Name:>> Alternative Contact's Phone: <<Alternative Contact's phone number>> [Alternative contact may be used to contact the Patient if they cannot be reached via the contact details given] Interpreter Required:<<Interpreter required>> Please specify Language: <<Please specify Language>> Is the Patient known to private Consultant/s? <<Is Patient known to private Consultant/s?>> If yes, provide Consultant's name: <<If yes, provide Consultant's name>> Has a Team Care Arrangement been completed? <<Has a Team Care Arrangement been completed?>> [Please ensure any current GPMP/TCA is attached] Has the Patient been referred for Close the Gap medication assistance? <<Has Pt been referred for CTG medication?>> Is this Patient newly diagnosed?<<Is this patient newly diagnosed?>> If no, when were they diagnosed? <<If no, when were they diagnosed?>> Do you consider this Patient's care needs are: <<Do you consider this Patient’s care needs are:>> Is this Patient able to participate in: General community physical activity progams <<Can Pt participate in general physical activity?>> A graded exercise program under the guidance of a Physiotherapist or Exercise Physiologist: <<Can Pt participate in graded Phys/Ex Phys program>> Please advise any restrictions that need to be considered during exercise: <<Advise restrictions to consider during exercise>> Include as much relevant information as possible about your Patient's condition to optimise their chances of being triaged correctly, e.g. diagnosis, duration, severity and impact. Reason for Referral Key examination findings: Management provided to date: Allergies: <<Clinical Details:Allergies>> <<Patient Demographics:Full Name>> <<Patient Demographics:DOB>> Developed in partnership by General Practice Gold Coast, Gold Coast Primary Health Network and Gold Coast Health January 2016 Current Medications: <<Clinical Details:Medication List>> PLEASE forward with the referral any of the following TESTS if relevant to your Patient: Spirometry Electrocardiogram (ECG) within last 3 months Bloods within last 3 months Relevant Medical History <<Clinical Details:History List>> <<Clinical Details:Family History>> SResults: <<Summary:Investigation Results (Selected)>> PLEASE make sure ALL relevant results from above are attached <<Patient Demographics:Full Name>> <<Patient Demographics:DOB>> Developed in partnership by General Practice Gold Coast, Gold Coast Primary Health Network and Gold Coast Health January 2016