Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
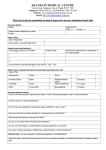
Suttons Medical Group Travel Questionnaire Travel health consultations are provided free to our patients on the NHS as an additional service. However if you book an appointment and then DO NOT ATTEND YOU WILL BE INVOICED A CHARGE FOR THE APPOINTMENT TIME WASTED. Please cancel any appointments that you can not attend giving plenty of notice and reschedule at a convenient time. Adapted from Travel Risk Assessment Form, © Travel Health Training Ltd. 2005 Page 1 of 5 03/06/11 Michele Bradley updated 07/08/14 WL Suttons Medical Group Travel Questionnaire Appointment Booked: Office use: Appt Time Needed: Date: Personal Details Name: Date Of Birth: Male [ ] Female [ ] Easiest contact telephone number: Address: Travel Details Departure Date: Email: Reason For travel Tick Boxes Holiday 1-28 days Holiday 28 days or more Return Date: Method of Tick travel Box Long haul flight Short haul flight Ferry/Boat Train Car Cruise: Cruise company Cruise Number Please attach itinerary Other (describe) Other Destinations Country Time: Business Trip Visiting friends or relatives Gap Year Voluntary work What type? Other (Describe) Do you travel abroad? Once a year Twice a Year More Frequently Hardly Ever Region Final destination Country Resort or port Region Urban or Rural High Altitude Going anywhere else during your journey? E.G. to change flights, join cruise, island hop, visit tourist attractions, game parks, waterfalls etc YES/NO If Yes please give details below Resort/port Length of Stay Please attach destinations on separate sheet if too many to list here Please tick as appropriate to best describe your trip Accommodation Planned Activities Travelling Hotel Self catering apartment/villa Safari Alone Walking in woodland With family/friends Private Home Climbing/Trekking at high altitude Snorkelling Camping Scuba/Sub aqua diving Sleeping Rough/ Adventure Hostel In a group Other information More than 24 hours from medical care? Mixing closely with Adapted from Travel Risk Assessment Form, © Travel Health Training Ltd. 2005 Page 2 of 5 03/06/11 Michele Bradley updated 07/08/14 WL Suttons Medical Group Travel Questionnaire Backpacking local population? Personal Medical History Do you have any recent or past medical history of note? (Including diabetes, heart or lung conditions, thymus disorder) List any current or repeat medications Do you have any allergies for example to eggs, antibiotics, nuts? Have you ever had a serious reaction to a vaccine given to you before? Does having an injection make you feel faint? Have you ever had a Pulmonary Embolus (PE) or Deep Vein Thrombosis (DVT)? Do you have any history or mental illness including depression or anxiety? Have you recently undergone radiotherapy, chemotherapy or steroid treatment? Have you taken out travel insurance and if you have a medical condition, informed the insurance company about this? Women only: Are you pregnant or planning pregnancy or breast feeding? Please write below any further information which may be relevant Vaccination History Have you ever had any of the following vaccinations / malaria tablets and if so when? Tetanus Polio Diphtheria Typhoid Hepatitis A Hepatitis B Meningitis Yellow Fever Influenza Jap B Tick Borne Encephalitis Encephalitis Rabies Other Malaria tablets For discussion when risk assessment is performed within your appointment: I have no reason to think that I might be pregnant. I have received information on the risks and benefits of the vaccines recommended and have had the opportunity to ask questions. I consent to the vaccines being given. Signed __________________________________________ Date ________ Adapted from Travel Risk Assessment Form, © Travel Health Training Ltd. 2005 Page 3 of 5 03/06/11 Michele Bradley updated 07/08/14 WL Suttons Medical Group Travel Questionnaire NB. All travel consultations are carried out at SUTTON BRIDGE SURGERY For official use Patient Name: Sign Date Form received Travax Printed Processed by nurse Travel risk assessment performed Yes [ ] No [ ] TRAVEL VACCINES RECOMMENDED FOR THIS TRIP Vaccines advised Yes Date had Further information Diphtheria Hepatitis A Polio Tetanus Typhoid Yellow Fever Vaccines to consider Cholera Hepatitis B Japanese B Encephalitis Measles (MMR) Meningitis ACWY Rabies Tick Borne Encephalitis Other MALARIA PREVENTION ADVICE and MALARIA CHEMOPROPHYLAXIS Is there a risk of malaria? Y/N Length of trip _________ NIGHTS Aware/understanding e.g. how contracted? Bite avoidance discussed? Y/N Drug Y/N Chloroquine Signs/symptoms/diagnosis Y/N Proguanil Malaria advice leaflet given Y/N Doxycycline FURTHER INFORMATION No. tablets Prescriber’s Signature Malarone e.g. weight of child Mefloquine Planned vaccine schedule for current trip Vaccine Day 0 Day Day Day Adapted from Travel Risk Assessment Form, © Travel Health Training Ltd. 2005 Page 4 of 5 03/06/11 Michele Bradley updated 07/08/14 WL Prescriber’s Signature Suttons Medical Group Travel Questionnaire Signed by: Position: Date: Adapted from Travel Risk Assessment Form, © Travel Health Training Ltd. 2005 Page 5 of 5 03/06/11 Michele Bradley updated 07/08/14 WL