Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
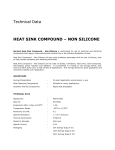
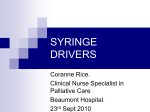
Standard Operating Procedure (SOP) Administration of Drugs via the CME Medical T34 Syringe Driver DOCUMENT CONTROL: Version: Ratified by: Date ratified: Name of originator/author: Name of responsible committee/individual: Date issued: Review date: Target Audience 2 Clinical Effectiveness Committee 5 November 2013 Community Practice Educator Medicines Management Committee 25 February 2014 November 2016 Community Nursing Staff 1. Aim This Standard Operating Procedure (SOP) represents current recommended good practice and will ensure the proper action to take regarding the setting up and management of the CME Medical T34 Syringe driver by clinical staff in the Community setting. 2. Scope All registered nurses using the CME T34 Syringe Driver must be personally competent and accountable in the use and operation of the device by attending bespoke training. Evidence of training will be recorded on each staff member’s training record. Mandatory annual updates will be provided. 3. Link to overarching policy and/or procedure This SOP is to be used in conjunction with the RDaSH Policy Safe and Secure Handling of Medicines. 4. Procedure 4.1 General Information The McKinley T34 Syringe Driver is being introduced across Rotherham Doncaster and South Humber NHS Foundation Trust (RDaSH) in line with the requirements of the National Patient Safety Alert entitled ‘Safer Ambulatory Syringe Drivers’ (NPSA/2010/RRR019) (2010) and will replace the previously used Micrel MP101 pumps throughout the Trust. 4.2 Safety The McKinley T34 is a small battery operated machine, designed to give a continuous subcutaneous infusion in millilitres (ml) per hour over a given period. This method of symptom control, used predominantly in palliative and terminal care provides relief of multiple symptoms e.g. pain, nausea and agitation via a single route. The safe use of the syringe driver requires comprehensive knowledge in order to maintain patient safety. Caution: If a patient is discharged home with a different make of syringe driver, this should be changed to a McKinley T34 device as soon as possible. Lock boxes will fit syringes up to 30ml and should always be used with the CME Medical T34. Lock boxes reduce the risk of accidental or intentional interference with the syringe driver and protect from damage caused by normal daily use or drops within the range of one metre. Page 2 of 27 4.3 Cleansing, Decontamination and Maintenance All staff must follow standard infection prevention and control precautions including hand hygiene, aseptic technique, use of personal protective equipment, decontamination of reusable medical devices, sharps management and disposal of healthcare waste. The device must be decontaminated between patients, daily when in use and as and when it becomes dirty or contaminated. Always turn the syringe driver off before cleaning. After patient use decontaminate the unit using lint free cloth such as Tuffi 5. Also clean actuator screw thread and guiding rods to remove debris or other particles. Do not clean the syringe pump with chemicals such as xylene, acetone, or similar solvents. These chemicals can cause damage to components and labels. Do not soak or immerse any part of the syringe driver in any solution. Immersing the pump in liquid will cause damage to components and this will void the guarantee. It is recommended that Tuffi 5 wipes are also used to decontaminate the lock box. All Syringe Drivers will require routine annual maintenance and service as a minimum or when syringe driver warning is indicated on individual syringe drivers. Key Health Solutions will provide maintenance work. Devices due for maintenance can be returned to the Community Support Manager who will then forward the devices onto Key Health Solutions. A declaration of decontamination status for will need completing and attaching to the device prior to sending it for repair or service. 4.4 Storage. It is essential that all syringe drivers are accounted for at all times. All District Nursing Teams are required to keep an up to date list of the exact location of the Syringe Drivers. (See appendix 1) Syringe Drivers will be stored at District Nursing Team bases. They will be stored in lockable cases and each device will have its’ own case. It will be the responsibility of the nurse who last used the device to clean the syringe driver and lock box adhering to the Standard Infection Prevention and Control Precautions Policy. The case will be refilled ready for further use and stored in a safe place within the base point. There will be 1 case for each device and these cases will be stored at each base point in the Community. Page 3 of 27 4.5 Equipment Required 1. Syringe driver McKinley T34 and Lock Box. Ensure within maintenance date. Obtain a new syringe driver if out of date. 2. 9-volt alkaline battery Duracell Procell. The average battery life is 3-5 days depending on usage e.g. key presses or backlight use. 3. Winged infusion set Saf-T-Intima24Gx0.75 FSP318Yellow. 4. Administration set CME McKinley Micro set 100-172S (Anti-siphon valve and female luer lock. Length approx. 100cm, priming volume approx. 0.5ml). 5. BD Plastipak luer lock syringe 20ml or 30ml. N.B. luer lock syringes must always be used to ensure secure connection of the infusion set. The pump is calibrated to luer lock and failure to use may result in under or over infusion due to variation in syringe dimensions. 6. Combi-stopper to cap the syringe or administration set 7. Transparent adhesive dressing 8. Drugs and diluent prescribed 9. Needle (to draw up drug) 10. Drug additive label 11. Patient’s Syringe Driver Prescription and Observation Chart or Care of the Dying IPOC document. 12. Sharps receptacle 13. Disposable carrying pouch (only if patient is mobile) 14. Instruction procedure manual and equipment, as documented on syringe driver check list. 15. Signing in and out sheet completed with the syringe driver serial number date, time, patient name and address (see appendix 2) 16. Battery will be removed when device not in use. Syringe driver to be stored in cases provided by Trust. A reciprocal agreement is in place between RDaSH and Doncaster and Bassetlaw Hospital NHS Foundation Trust (DBHFT) for the safe return of syringe drivers to their respective bases. Page 4 of 27 The syringe driver must be returned to base after use. If the patient is admitted to hospital, then it is the responsibility of the nurse who is allocated to the visit to ensure that they retrieve the syringe driver. The responsible nurse will contact the Community Support Manager via e-mail using the relevant form. (See appendix 2) An agreement is in place with Doncaster Royal Infirmary (DRI) for devices that turn up with patients that have been admitted to hospital. These devices will be returned to the medical devices unit at DRI. The medical devices unit will then return the device to the Community Support Manager. If devices from DRI are sent home with patients in the community, these will be returned by the Community Support Manager to the medical devices unit at DRI. Transferred out of RDaSH The registered nurse must: • • • • Record the details and serial number of the syringe driver on the district nurse referral form or on the transfer letter if the patient is discharged to a care home, other hospital or hospice Place a copy of the form in the patient’s notes Request that care home, hospital or hospice return the syringe driver to Medical Technical Services Inform Medical Technical Services of the transfer Caution: If a patient is discharged home from a neighbouring hospital (other than Doncaster Royal Infirmary) with a different make of syringe driver, this should be changed over to the McKinley T34 and the other syringe driver returned to the hospital in question as soon as possible. 4.6 Administration Procedure It is good practice for two staff members, one of which must be qualified, to undertake the procedure; however, in community settings where there may not be another health professional available, the patient’s relative may act as a second signatory to check relevant aspects of the procedure. E.g. Stock levels. Indications for the use of a syringe driver The inability of the patient to swallow or absorb oral drugs because of: Intestinal Obstruction Persistent Vomiting Dysphagia Mouth Throat or Oesophageal Tumour Altered Level of Consciousness Malabsorption Profound Weakness Page 5 of 27 Advantages Plasma drug levels are maintained preventing peaks and troughs Effective symptom control without repeated injections Control of multiple symptoms with a combination of drugs Mobility and independence maintained for some patients Disadvantages/Risks Medication errors relating to drug or dose Inflammation or infection may occur at skin site Drug/patient and drug/diluent incompatibility Standard Operating Procedure for the Administration of Drugs via a 4.6 Involving the patient and family Communication and consultation with the patient and family is essential. Before starting a subcutaneous infusion, the reasons for using this method of administration should be explained to the patient and family. Informed consent for administration should be obtained, in accordance with the Mental Capacity Act 2005 Policy. The discussion is then to be recorded in the nursing care plan. Attention should be paid to both the physical and psychological aspects involved in accepting a new way of receiving medication. Some patients feel that this method of drug delivery is a last resort that their activities will be restricted and that death may be imminent. It is necessary to listen to and answer the patient’s questions, acknowledge their concerns and then give explanations and reassurance as appropriate. The patient and family will be informed that the syringe driver device is on loan to them and must be returned as delivered after use. A signature will be required from the patient or family after discussion. (See appendix 5) The explanation should include the following: The reasons for using a syringe driver How the syringe driver works The siting procedure and site care How the dose of medication can be adjusted to manage symptoms Encouragement to describe symptoms Page 6 of 27 4.7 McKinley T34 Feature Recognition Barrel clamp arm…. secures syringe and detects brand and size Collar sensor……… detects correct loading of syringe collar Plunger sensor…… detects correct loading of the syringe plunger Actuator…………… drives the syringe plunger to deliver the syringe contents Info key……………. (a) shows infusion summary, protocol parameters, battery level (b) when pump is paused, access the main menu (c) activates/deactivates keypad lock UP arrow key……... (a) scrolls between options (b) increases infusion parameters Down arrow key….. (a) scrolls between options (b) decreases infusion parameters during programming/titration Yes/Start…………... Confirms selection and starts infusion No/Stop……………. (a) stops infusion (b)takes the user back a step during programming FF (Forward) ….…. (a) moves actuator forward when no syringe in place and barrel clamp arm is down (b) accesses purge function (if enabled) Back (Reverse)…... moves actuator backward when no syringe is in place and barrel clamp arm is down On/Off key…………Switches the pump on and off Infusion LED light…A green indicator lights: (a) during system self-test (b) intermittently to indicate infusion delivery A red indicator light: (a) continuously to indicate an alarm state (b) when pump paused/on stand-by mode Page 7 of 27 4.8 Procedure for setting up the syringe driver A registered nurse must calculate the volume of drug that needs to be drawn up from the concentration of the preparation to be used and the prescribed dose. When preparing medicines and disposing of waste materials, the registered nurse must adhere to the following guidance:Safe and Secure Handling of Medicines Policy SOP for Controlled Drugs Standard Infection Prevention and Control Precautions Policy Sharps Policy – Safe Use and Disposal of Sharps and Management of Contamination Injuries Hand Hygiene policy NMC Standards of Medicines Management The Medicines Act (1986) Waste Policy A registered nurse must ensure:• • • The prescription has been completed correctly, perform the calculation and check the medication. Confirm the previous opioid dose, formulation and frequency. Ensure the medication prescribed and the doses are clinically appropriate based on the patient’s previous requirements (NPSA, 2008). The diluent will be prescribed on the patient’s Syringe Driver Prescription (Syringe Driver Pro-Forma). Sterile water for injection Advantages • Recommended because of its use in reconstituting lyophilized (freeze-dried) diamorphine (the parenteral strong opioid of choice in the UK) • More supporting compatibility data • Reduces the risk of precipitation with cyclizine lactate Disadvantages • Large volumes are hypotonic and can cause infusion site pain Sterile 0.9% Sodium chloride Advantages • Recommended with certain drugs e.g. octreotide • Less infusion site pain and fewer skin reactions Disadvantages • Incompatible with cyclizine • Increases likelihood of precipitation when more than one drug is used Page 8 of 27 There is a potential for interaction between drugs in a syringe driver. The compatibility of the drugs and the diluent to be drawn up must be checked prior to mixing. The Palliative Care Formulary (Twycross et al, 2011), The Syringe Driver, Continuous subcutaneous infusions in palliative care (Dickman A and Schneider J, 2011) suggest suitable combinations of drugs. If there are any concerns regarding compatibility please contact the Specialist Palliative Care Team or Pharmacy. Out of hours, please contact the on call Consultant in Palliative Medicine or on call Pharmacist. Please refer to Compatibility and stability tables for a subcutaneous infusion in a McKinley T34 Syringe Pump (Appendix 3). In Rotherham Doncaster and South Humber NHS Foundation Trust (RDaSH) a combination of no more than 3 dugs should be prescribed on the prescription form or drawn up into a syringe. If more than 3 drugs are required, 2 prescription forms and 2 syringe drivers will be needed. Please seek advice from the Specialist Palliative Care Team. N.B. Ampules containing a liquid solution may contain an amount in excess of the volume stated on the label. Therefore, measure the volume of liquid as it is drawn up to ensure accuracy of the dose. • • • • • • Select the appropriate syringe size 20ml or 30ml Draw up the prescribed medication Add the diluent up to the required volume Complete the label, including: - Patient name and NHS number - Medicine name and dose - Batch numbers - Diluent used - Route of infusion - Date and time prepared - Initials of the registered nurses preparing the syringe Attach the label to the syringe ensuring that it is flat and not folded. Leave the scale visible so that it can still be read. Skin Site Selection for Subcutaneous Infusions Following completion of the procedure record keeping principles will be used to record correctly the prescribed medication, dose, dilutant and site of the syringe driver alongside the amount of prescribed medication remaining. (See appendix 3). Note when using Appendix 3:This is not an exhaustive list of compatible combinations. When setting up a syringe driver you should consult the list, if the prescribed combination is not on the list you should risk assess the situation. Contact St Johns Hospice to determine the suitability for the combination, as they have access to a more extensive list. Consider the administration history for that patient – has the combination been administered without incident prior to this instance. Page 9 of 27 Contact the prescriber and consider their personal experience or advice they have taken, in prescribing the combination. Additionally – this list is up review in Sept 2013 – so will need to be updated accordingly. The CME Medical T34 ambulatory syringe pump is calibrated to operate with BD Plastipak Luer lock syringe brands and sizes. It is programmed to recognise both the brand and the size of syringe being used (commonly 20ml. and 30ml).It will be defaulted using a Prime and Load (Lock – on) Programme of a 24 hour delivery system. Fill volume Medication and diluents should always be drawn up to the following volumes 20ml syringe draw up to 17ml 30ml syringe draw up to 22ml N.B The 50ml BD Plastipak luer lock syringe is the largest syringe that will fit the McKinley T34. It allows drugs to be drawn up to approximately 34ml volume for BD Plastipak syringes. This may reduce the need for a second syringe driver when giving larger volumes of drugs. 50ml syringes will not fit into the lock box and are not recommended for routine use. If a 50ml syringe is thought to be required, please contact the Advanced users within your team. Where possible involve the patient in the choice of a suitable site. Areas suitable for subcutaneous infusion include those with a good depth of subcutaneous fat, towards the trunk of the body, particularly if the patient’s peripheral circulation is compromised. Page 10 of 27 Acceptable sites Sites to avoid Oedematous areas, including areas affected by lymphoedema or ascites. (poor absorption, increased risk of infection) Sites over bony prominences (discomfort and poor absorption) Joints or skin folds (discomfort and movement may displace cannula) Previously irradiated skin (may have poor perfusion - affects drug absorption) Upper abdomen in a patient with an enlarged liver (risk of puncturing the liver capsule) Upper chest wall in a very cachectic patient (risk of pneumothorax) Infected, broken, inflamed or bruised skin Sites of tumour Inserting BD Saf-T- Intima Venflon Please note PPE and hand hygiene principles should be adhered to for all procedures. • Clean the site with soap and water if the skin is dirty otherwise there is no need to swab the skin • Apply the clamp to the line • Grasp the “pebbled” side of the wings of the cannula, pinching the wings firmly together. This “locks” the needle and prevents it from retracting during insertion • Ensure that the needle is point down and bevel uppermost, to guide the cannula through the tissues. This prevents kinking of the cannula Page 11 of 27 • If the needle is not already orientated with the point down open the wings and gently twist the white shield until the needle is correctly positioned • Insert the cannula subcutaneously at an angle of less than 45 degrees, lowering the initial angle of the cannula to a level more parallel to the skin (caution on the chest wall) and advance to the hilt of the cannula • Open the wings (pebbled side down) flat against the skin • Apply transparent adhesive dressing over the insertion site and the cannula wings • Apply firm finger- tip pressure over the wings of the cannula (avoiding the centre where the needle retracts) simultaneously grasp the pebbled end of the coloured/white cylinder shield and pull in a straight continuous motion until the needle has fully with drawn into the cylinder and pops off • Gently remove cylinder from the cannula port, if it has not released spontaneously, exposing the adapter with the rubber bung • Place the needle shield in the sharps bin • Change the site every 7 days or as necessary depending on the condition of the skin N.B.The Saf-T-Intima cannot be primed when using the McKinley T34. When setting up the syringe driver the primed extension line is connected directly to the un-primed Saf-T-Intima The registered nurse must prepare the syringe and confirm the patient’s identity as on prescription • • • • • • • • • • • Check the battery life by pressing the INFO Key twice *** Prepare syringe and contents and cap the syringe. Press STOP Press and hold INFO key to deactivate keypad lock If the infusion complete alarm has activated, press YES to confirm end of infusion Switch syringe driver OFF Clamp Saf-T-Intima Raise the barrel clamp arm Remove old syringe Follow instructions on page 18 Power on and pre-loading When “Start infusion?” screen displays, connect the infusion line to the syringe, release the clamp on the Saf-t- Intima and press YES *** For community use the battery will need changing when the device registers at 40% battery life left. Page 12 of 27 Bolus dose of medication If the patient has uncontrolled symptoms prior to setting up the McKinley T34, it may be necessary to give a bolus dose of medication. A separate Saf-T- Intima 24Gx0.75 FSP318 Yellow should be inserted for the purpose of giving bolus doses. A Swan Lock needle free device should be attached to the Saf-TIntima port. Temporary interruption to the infusion This is not normal practice in a community setting and should only be used in exceptional circumstances e.g. showering or bathing. N.B. Stopping the infusion will delay the end time of the infusion Stopping the Infusion • Press STOP – unlock the keypad and turn the syringe driver OFF. • Clamp the Saf-T- Intima • Disconnect the syringe driver. DO NOT REMOVE THE SYRINGE FROM THE PUMP • Cap the Saf-T-Intima and infusion line to minimize cross infection. • Record time and reason why infusion stopped on Syringe Driver Observation Chart Resuming the Infusion • Check that the prescription, syringe label and patient details are correct • Reconnect the line to the syringe on the pump maintaining asepsis • Press and hold ON button • The screen will request confirmation of size and brand of syringe • Press YES to confirm • The screen will display “Press YES to Resume” “NO for New Syringe” • Press YES to resume • The screen will display remaining volume/ duration/ rate of infusion • Ensure information is correct as prescribed • Press YES to confirm • Unclamp Saf-T-Intima • Screen will display “Start Infusion?” • Press YES to start infusion • Press and hold INFO key to lock the keypad • Replace the Lock Box • Record on the Syringe Driver Observation chart the time the infusion was recommenced N.B. If “NO for New Syringe” is pressed the remaining infusion will be reset to deliver over the next 24hrs at a different rate, and the infusion will be incorrect. If “NO for New Syringe” has been pressed in error. Discard the remainder of the syringe contents, prepare, and set up a new syringe. Page 13 of 27 N.B. In a community setting the following procedure should not be applicable as staff will check the battery status before commencing each 24 hour regime. Changing the battery during an infusion • • • • • • • • • When near the end of the battery alert sounds, it indicates that the battery should be changed within the next half hour Press STOP and apply clamp to Saf-T-Intima Insert new battery Restart the syringe driver Reconfirm syringe size and brand Press YES to resume Reconfirm volume and duration and rate of infusion Press YES to recommence the infusion Lock the keypad Following completion of the procedure all patient records will be updated and signed by the registered nurse. (For paper documentation see appendix 2). Records will also include those accessed on System One. What to do if there is an occlusion in the extension line • • • • • • Check that the Saf-t-Intima is not clamped Check the extension line and Saf-t-Intima for any kinking – straighten if kinked Check the syringe, extension line and Saf-t-Intima for any signs of crystallization of the solution. If crystallization detected – prepare and fit new syringe, extension line and change Saf-t-Intima site If no physical reason for the occlusion is detected – resite the Saf-t-Intima If occlusion is still present – change the site, extension line and syringe N.B. During an occlusion the pump’s Post Occlusion Reduction System will reverse the operation of the motor and drive the actuator backwards, otherwise the pressure build up could cause a surge of fluid into the patient on release of the occlusion. When the pump is resumed/restarted following the backward movement of the actuator, time will be added to the time remaining to protect the original calculated rate. Page 14 of 27 Procedure for releasing a trapped foreign object from the actuator (See appendix 4) WARNING: IF A FOREIGN OBJECT IS TRAPPED IN FRONT OF OR BEHIND THE ACTUATOR DURING PRE-LOADING (AUTOMATIC ACTUATOR MOVEMENT) OR WHEN MANUALLY ADJUSTING THE ACTUATOR, THE USER SHOULD: • • • • • • Ignore screen prompts as the prompt that may display will be in relation to alarm activation and NOT the trapped object Turn the syringe driver OFF Raise the barrel clamp arm and turn it to the left or right to keep it in the raised position Turn the syringe driver ON Turn and lower the barrel clamp arm Use the FF key (or BACK key) to move the actuator in order to release the object 4.9 Contacting the Palliative care team for advice Out of hours advice – Monday – Friday after 18:00hrs, weekends and bank holidays contact the on call Consultant in Palliative Medicine via DRI switchboard. 4.10 Incident Reporting Systems are in place within Rotherham Doncaster and South Humber NHS Foundation Trust to report and manage incidents, near misses and serious untoward incidents involving syringe pumps. Staff should be familiar with the reporting process and the Incident Reporting Policy. Page 15 of 27 Acknowledgements McKinley T34 Ambulatory Syringe Pump Operations Manual (2011) Illustrations courtesy of CME McKinley Medical CME McKinley UK Ltd Kincraig Business Park Kincraig Road Blackpool FY2 0PJ Tel: 01253 894646 www.cme-mckinley.co.uk 5. Links to Associated Documents Aseptic technique and Aseptic Non Touch Technique Policy Lifecycle of Clinical & Corporate Records Policy Medical Devices Policy The Medicines Act (1986) Mental Capacity Act 2005 Policy Incident Reporting Policy Policy for Consent to Examination and Treatment. SOP for Controlled Drugs Standard Infection Prevention and Control Precautions Policy Sharps Policy – Safe Use and Disposal of Sharps and Management of Contamination Injuries Hand Hygiene Policy NMC Standards of Medicines Management Waste Policy Page 16 of 27 6. References and Literature review British Medical Association and the Royal Pharmacological Society of Great Britain. (2013) British National Formulary No 64 London. BMA and RPSGB. Dickman A and Schneider J (2011) The Syringe Driver. Continuous subcutaneous infusions in palliative care 3rd edition, Oxford University Press, Oxford Perdue, C. (2004) The syringe driver – an aid to delivering symptom control. Nursing Times, 100, 13. pp32-35. Medicines Act 1986. HMSO: London Mental Capacity Act (2005) DOH: London Mitten, T. (2001) Subcutaneous drug infusions: a review of problems and solutions. International Journal of Palliative Nursing, 7,2. pp.75-85. National Patient Safety Agency (2008) Reducing dosing errors with Opioid Medicines Rapid Response Report 05 National Patient Safety Agency (2010) Safer ambulatory syringe drivers Rapid Response Report 019 NMC (2008) The Code: Standards of conduct, performance and ethics for nurses and midwives, Nursing and Midwifery council, London NMC (2008) Standards for medicines management, Nursing and Midwifery Council, London Twycross, R and Wilcock A (2011) (eds) Palliative Care Formulary4th edition, Nottingham, palliativedrugs.com Ltd. Wilson J. (2001) Infection Control in Clinical Practice. BailliereTindall. London pp138 7. Appendices Appendix 1. Syringe Driver base information Appendix 2. Subcutaneous syringe driver instruction and observation chart for McKinley T34 and continuation sheet Appendix 3. McKinley Syringe pump compatability tables Appendix 4. Procedure for releasing a trapped object from the actuator Appendix 5. Form for the patient regarding loan of syringe driver Page 17 of 27 Appendix 1 SYRINGE DRIVE BASE INFORMATION SYRINGE DRIVER IDENTIFICATION CODE CLUSTER AREA IN USE/NOT IN USE nb. IF IN USE PLEASE REFER TO THE RECORD SHEET STAFF SIGNATURE Appendix 2 SUBCUTANEOUS SYRINGE DRIVER INSTRUCTION AND OBSERVATION CHART FOR MCKINLEY T34 PRESCRIPTION DETAILS [for completion by the prescriber] – a separate form must be completed for each syringe driver a DRUG DOSE DILUENT PHARMACY ALLERGY STATUS Please circle Date 1. Route Duration of flow SC 2. Please circle 12 hours 24 hours 3. Water for injection or Normal Saline 4. The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. If, as the prescriber, you wish to review the patient on a particular date, please stipulate below - Review date: ……………………….. Prescriber name: ………………………………………… Signature: ………………………………………………… Practice: …………………………………………….. PATIENT DETAILS [Affix label if available] NHS Number: ……………………………………………….. Surname: ……………………………………………………… Forename(s): ………………………………………………… Address: ……………………………………………………….. ………………………………………………………. DOB: …………………….. a. Pharmacy: Only complete if this form is used on a ward. NOT required for community use. DAILY SET UP MONITORING PROGRESS ADMINISTRATION & OBSERVATION DETAILS [for completion by administering clinician] WARD OR BASEPOINT NAME The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. ADMINISTRATION1 Day and Date OBSERVATIONS2 Time [HH:MM] 6 Start time of infusion: Site appearance : 17ml infusion in 20ml syringe Syringe size used Syringe/line contents clear3 - OK to continue? [Y/N] 22ml infusion in 30ml syringe 20ml or 30ml Infusion rate setting – as at set up? [Y/N] Syringe Driver serial No.: Battery Status [%]: Infusion time remaining [HH:MM] Infusion rate [ml/hr]: Volume still to be infused (vtbi) [ml] Site used5: Site Appearance6: Is the VTBI correct for time remaining [Y/N] Drawn up by: Checked by: Volume infused [ml] Details of any problems & actions taken: Battery status [%]4 Is the key pad locked? [Y/N] Observer’s initials If syringe contents discarded: Volume discarded: Date & time: Discharged by: Checked: 1. 2. 3. To be completed each time syringe driver is loaded WARD - Completed 30 minutes after loading and then every 4 hours COMMUNITY – Complete at set up, at each subsequent visit and at syringe change If contents of syringe look cloudy, precipitation has occurred. STOP infusing and contact prescriber. Refer to policy for guidance on checking compatibility 4. Change battery when less than 10% (ward ) or 40% (community) 5. Document insertion site of winged infusion 6. Appearance: Use code below NP (no problem) P (pain) I (inflammation) SW (swelling) B (bleeding) H (hardening) Page 1 SUBCUTANEOUS SYRINGE DRIVER CONTINUATION SHEET DAILY SET UP MONITORING PROGRESS ADMINISTRATION & OBSERVATION DETAILS WARD OR BASEPOINT NAME The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. ADMINISTRATION1 Day and Date OBSERVATIONS2 Time [HH:MM] Start time of infusion: Site appearance6 : 17ml infusion in 20ml syringe Syringe size used Syringe/line contents clear3- OK to continue? [Y/N] 22ml infusion in 30ml syringe 20ml or 30ml Infusion rate setting – as at set up? [Y/N] Syringe Driver serial No.: Battery Status [%]: Infusion time remaining [HH:MM] Infusion rate [ml/hr]: Volume still to be infused (vtbi) [ml] 5 6 Site used : Site Appearance : Is the VTBI correct for time remaining [Y/N] Drawn up by: Checked by: Volume infused [ml] Details of any problems & actions taken: Battery status [%]4 Is the key pad locked? [Y/N] If syringe contents discarded: Volume discarded: Observer’s initials Date & time: Discharged by: Checked: DAILY SET UP MONITORING PROGRESS ADMINISTRATION & OBSERVATION DETAILS WARD OR BASEPOINT NAME The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. ADMINISTRATION1 Day and Date OBSERVATIONS2 Time [HH:MM] 6 Start time of infusion: Site appearance : 17ml infusion in 20ml syringe Syringe size used Syringe/line contents clear3 - OK to continue? [Y/N] 22ml infusion in 30ml syringe 20ml or 30ml Infusion rate setting – as at set up? [Y/N] Syringe Driver serial No.: Battery Status [%]: Infusion time remaining [HH:MM] Infusion rate [ml/hr]: Volume still to be infused (vtbi) [ml] Site used5: Site Appearance6: Is the VTBI correct for time remaining [Y/N] Drawn up by: Checked by: Volume infused [ml] Details of any problems & actions taken: Battery status [%]5 Is the key pad locked? [Y/N] If syringe contents discarded: Volume discarded: Observer’s initials Date & time: Discharged by: Checked: 1. 2. 3. To be completed each time syringe driver is loaded WARD - Completed 30 minutes after loading and then every 4 hours COMMUNITY – Complete at set up, at each subsequent visit and at syringe change If contents of syringe look cloudy, precipitation has occurred. STOP infusing and contact prescriber. Refer to policy for guidance on checking compatibility 4. Change batter when less than 10% (ward ) or 40% (community) 5. Document insertion site of winged infusion 6. Appearance: use code below NP (no problem) P (pain) I (inflammation) SW (swelling) B (bleeding) H (hardening) Page …….. SUBCUTANEOUS SYRINGE DRIVER CONTINUATION SHEET DAILY SET UP MONITORING PROGRESS ADMINISTRATION & OBSERVATION DETAILS WARD OR BASEPOINT NAME The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. ADMINISTRATION1 Day and Date OBSERVATIONS2 Time [HH:MM] Start time of infusion: Site appearance6 : 17ml infusion in 20ml syringe Syringe size used Syringe/line contents clear3- OK to continue? [Y/N] 22ml infusion in 30ml syringe 20ml or 30ml Infusion rate setting – as at set up? [Y/N] Syringe Driver serial No.: Battery Status [%]: Infusion time remaining [HH:MM] Infusion rate [ml/hr]: Volume still to be infused (vtbi) [ml] 5 6 Site used : Site Appearance : Is the VTBI correct for time remaining [Y/N] Drawn up by: Checked by: Volume infused [ml] Details of any problems & actions taken: Battery status [%]4 Is the key pad locked? [Y/N] If syringe contents discarded: Volume discarded: Observer’s initials Date & time: Discharged by: Checked: DAILY SET UP MONITORING PROGRESS ADMINISTRATION & OBSERVATION DETAILS WARD OR BASEPOINT NAME The patient will be reviewed by the attending clinician at each attendance and, where there has been a change of circumstances, will refer to the prescriber for any necessary treatment changes or need for review. ADMINISTRATION1 Day and Date OBSERVATIONS2 Time [HH:MM] 6 Start time of infusion: Site appearance : 17ml infusion in 20ml syringe Syringe size used Syringe/line contents clear3 - OK to continue? [Y/N] 22ml infusion in 30ml syringe 20ml or 30ml Infusion rate setting – as at set up? [Y/N] Syringe Driver serial No.: Battery Status [%]: Infusion time remaining [HH:MM] Infusion rate [ml/hr]: Volume still to be infused (vtbi) [ml] Site used5: Site Appearance6: Is the VTBI correct for time remaining [Y/N] Drawn up by: Checked by: Volume infused [ml] Details of any problems & actions taken: Battery status [%]5 Is the key pad locked? [Y/N] If syringe contents discarded: Volume discarded: Observer’s initials Date & time: Discharged by: Checked: 4. 5. 6. To be completed each time syringe driver is loaded WARD - Completed 30 minutes after loading and then every 4 hours COMMUNITY – Complete at set up, at each subsequent visit and at syringe change If contents of syringe look cloudy, precipitation has occurred. STOP infusing and contact prescriber. Refer to policy for guidance on checking compatibility 4. Change batter when less than 10% (ward ) or 40% (community) 5. Document insertion site of winged infusion 6. Appearance: use code below NP (no problem) P (pain) I (inflammation) SW (swelling) B (bleeding) H (hardening) Page …….. Appendix 3 Compatibility and stability tables for a subcutaneous infusion in a McKinley T34 Syringe Pump Table 1: Subcutaneous Morphine Infusion Diluent: Water for injections • The figures in these tables are not clinical doses to prescribe. Most patients do not need such large amounts of medication. • • Refer to the relevant guidelines to obtain the usual dose range for each of the medications. Use the minimum effective dose and titrate according to response. Use the table to check for concentrations that are stable for 24 hours; their use is unlicensed. • Drug Combination Concentrations of two drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Morphine Sulphate Cyclizine 300mg 150mg 380mg 150mg Morphine Sulphate Glycopyrronium bromide 300mg 1200 micrograms 380mg 1200 micrograms Morphine Sulphate Haloperidol 400mg 10mg 500mg 10mg Morphine Sulphate Hyoscine butylbromide 300mg 120mg 380mg 120mg Morphine Sulphate Hyoscine hydrobromide 450mg 1200 micrograms 580mg 1200 micrograms Morphine Sulphate Levomepromazine 300mg 100mg 380mg 100mg Morphine Sulphate Metoclopramide 120mg 60mg 150mg 70mg Morphine Sulphate Midazolam 300mg 30mg 380mg 35mg Morphine Sulphate Octreotide 400mg 400 micrograms 500mg 500 micrograms Drug Combination Concentrations of three drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Morphine Sulphate Cyclizine Haloperidol 40mg 100mg 2mg 50mg 100mg 3mg Morphine Sulphate Haloperidol Midazolam 100mg 5mg 20mg 130mg 6mg 25mg Morphine Sulphate Hyoscine butylbromide Midazolam 50mg 40mg 60mg 60mg 50mg 75mg Morphine Sulphate Metoclopramide Midazolam 50mg 30mg 7mg 60mg 40mg 10mg Morphine Sulphate Midazolam Levomepromazine 180mg 10mg 5mg 230mg 12mg 5mg 73 Table 2: Subcutaneous Diamorphine infusion in a McKinley T34 Syringe Pump Diluent: Water for injections • The figures in these tables are not clinical doses to prescribe. Most patients do not need such large amounts of medication. • • Refer to the relevant guidelines to obtain the usual dose range for each of the medications. Use the minimum effective dose and titrate according to response. Use the table to check for concentrations that are stable for 24 hours; their use is unlicensed. • Drug Combination Concentrations of two drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Diamorphine Cyclizine 340mg 150mg 440mg 150mg Diamorphine Glycopyrronium bromide 425mg 1200 micrograms 550mg 1200 micrograms Diamorphine Haloperidol 800mg 10mg 1000mg 10mg Diamorphine Hyoscine butylbromide 1000mg 120mg 1000mg 120mg Diamorphine Hyoscine hydrobromide 1000mg 1200 micrograms 1000mg 1200 micrograms Diamorphine Levomepromazine 850mg 100mg 1000mg 100mg Diamorphine Metoclopramide 1000mg 85mg 1000mg 110mg Diamorphine Midazolam 560mg 80mg 720mg 80mg Diamorphine Octreotide 425mg 900 micrograms 550mg 900 micrograms Drug Combination Concentrations of three drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Diamorphine Cyclizine Haloperidol 340mg 150mg 10mg 440mg 150mg 10mg Diamorphine Haloperidol Midazolam 800mg 7mg 65mg 1000mg 10mg 80mg Diamorphine Hyoscine butylbromide Midazolam 120mg 80mg 20mg 150mg 100mg 25mg Diamorphine Levomepromazine Metoclopramide 850mg 100mg 50mg 1000mg 100mg 60mg Diamorphine Levomepromazine Midazolam 850mg 50mg 30mg 1000mg 60mg 40mg 74 Table 3: Subcutaneous Oxycodone infusion in a McKinley T34 Syringe Pump Diluent: Water for injections • The figures in these tables are not clinical doses to prescribe. Most patients do not need such large amounts of medication. • • Refer to the relevant guidelines to obtain the usual dose range for each of the medications. Use the minimum effective dose and titrate according to response. Use the table to check for concentrations that are stable for 24 hours; their use is unlicensed. • • If the 10mg/ml preparation of oxycodone injection is used, and the 24 hour dose of oxycodone exceeds 60mg, an alternative opioid may be needed for breakthough pain. Drug Combination Concentrations of two drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Oxycodone Cyclizine Do not mix - Incompatible Do not mix - Incompatible Oxycodone Haloperidol 140mg 10mg 180mg 10mg Oxycodone Hyoscine butylbromide 140mg 40mg 180mg 50mg Oxycodone Hyoscine hydrobromide 130mg 1200 micrograms 160mg 1200 micrograms Oxycodone Levomepromazine 120mg 100mg 150mg 100mg Oxycodone Metoclopramide 80mg 40mg 100mg 50mg Oxycodone Midazolam 80mg 40mg 100mg 50mg Oxycodone Octreotide 80mg 400 micrograms 100mg 500 micrograms Drug Combination Concentrations of three drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Oxycodone Haloperidol Hyoscine butylbromide 80mg 2mg 100mg 100mg 5mg 120mg Oxycodone Haloperidol Hyoscine hydrobromide 80mg 2mg 1000 micrograms 100mg 5mg 1200 micrograms Oxycodone Haloperidol Midazolam 80mg 2mg 15mg 100mg 5mg 20mg Oxycodone Levomepromazine Hyoscine butylbromide 80mg 20mg 100mg 100mg 25mg 120mg 75 Table 4: Subcutaneous Alfentanil infusion in a McKinley T34 Syringe Pump Diluent: Water for injections • The figures in these tables are not clinical doses to prescribe. Most patients do not need such large amounts of medication. • • Refer to the relevant guidelines to obtain the usual dose range for each of the medications. Use the minimum effective dose and titrate according to response. Use the table to check for concentrations that are stable for 24 hours; their use is unlicensed. • Drug Combination Concentrations of two drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Alfentanil Cyclizine 4mg 150mg 5mg 150mg Alfentanil Glycopyrronium bromide 5mg 1200 micrograms 8mg 1200 micrograms Alfentanil Haloperidol 7mg 10mg 10mg 10mg Alfentanil Hyoscine butylbromide 5mg 120mg 8mg 120mg Alfentanil Hyoscine hydrobromide 7mg 1200 micrograms 10mg 1200 micrograms Alfentanil Levomepromazine 7mg 40mg 10mg 50mg Alfentanil Metoclopramide 2mg 60mg 3mg 80mg Alfentanil Midazolam 3mg 50mg 5mg 60mg Alfentanil Octreotide 6mg 800 micrograms 8mg 900 micrograms Drug Combination Concentrations of three drug combinations that are physically stable for 24 hours 17ml in 20ml syringe 22ml in 30ml syringe Alfentanil Haloperidol Midazolam 4mg 5mg 35mg 6mg 5mg 45mg Alfentanil Hyoscine butylbromide Levomepromazine 5mg 120mg 25mg 7mg 120mg 25mg Alfentanil Metoclopramide Midazolam 3mg 35mg 20mg 3mg 45mg 30mg Alfentanil Levomepromazine Midazolam 3mg 80mg 30mg 5mg 100mg 40mg 1. Dickman A: The syringe driver: continuous subcutaneous infusions in palliative care. 2nd Edition, 2005. OUP. 2. Palliative care drug information online http://www.palliativedrugs.com/ Appendix 4 77 Appendix 5 You have been loaned a syringe driver by Rotherham Doncaster and South Humber NHS Foundation Trust. Make and Model........................................................................................................... Serial Number............................................................................................................... This syringe driver will be cleaned, maintained and tested to ensure it is, and remains fit for purpose by the Nursing team. We have included an instruction manual for the unit that you have been given. Please ensure that; • • The driver is kept dry It is handled with care Delivered by (Print name)................................................................RDaSH Employee Instruction given - Date.............................Signature..................................................... Syringe driver accepted by (print name)...................................................Patient/carer Date accepted.................................................................. By accepting this machine I agree to the above. Signature...................................................................................................Patient/carer Advice available from............................................................ Please contact .............................................................................. for any issues or to return the unit. The equipment specified remains the property of Rotherham Doncaster and South Humber NHS Foundation Trust and must be returned to the contact above in the condition it was received in when no longer required. 78