Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
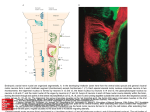
Motor Speech Disorders Samantha Shune, PhD, CCC-SLP [email protected] Preview Brief introduction to motor speech disorders Brief neuroanatomy primer Video samples INTRODUCTION Neurogenic Communication Disorders Neurogenic communication disorders can be defined as impairments in speaking, listening, reading, and writing skills that result from damage in different parts of the nervous system. These impairments include: Aphasia Cognitive-Communication Disorders Motor Speech Disorders Dysarthria Apraxia of Speech Cognitive-Communication Disorder Aphasia Apraxia of Speech Dysarthria Motor Speech Disorders Motor speech disorders can be defined as disorders of speech resulting from neurologic impairments affecting the: Motor planning, Motor programming, or Neuromuscular execution of speech Dysarthria and apraxia of speech Motor speech disorders are a significant proportion of acquired communication disorders Motor speech disorders 8% 8% 41% 8% 4% Other cognitive-language disorders Psychogenic 11% 19% Other neurologic speech disorders Aphasia 1% Etiologies of Motor Speech Disorders VITAMIN D (Dworkin, 1991) V I T A M I N D vascular accidents infectious processes traumatic insults allergic or anoxic metabolic disorders idiopathic neoplasms degenerative demyelinating Major types of MSDs Type Localization Neuromotor basis Flaccid Dysarthria Lower motor neuron Weakness Spastic Dysarthria Bilateral upper motor neuron Spasticity Ataxic Dysarthria Cerebellum Incoordination Hypokinetic Dysarthria Basal ganglia control circuit Rigidity/reduced range of movement Hyperkinetic Dysarthria Basal ganglia control circuit Involuntary movements Unilateral Upper Motor Neurons (UUMN) Dysarthria Unilateral upper motor neurons Weakness, incoordination, or spasticity Mixed More than one More than one Apraxia of Speech Left (dominant) hemisphere Motor planning Distribution of MSDs Type Percentage Flaccid Dysarthria 8% Spastic Dysarthria 7% Ataxic Dysarthria 9% Hypokinetic Dysarthria 9% Hyperkinetic Dysarthria 19% Unilateral Upper Motor Neurons Dysarthria 8% Mixed 28% Apraxia of Speech 7% Dysarthria, type undetermined 4% From Duffy, 2012 Methods for Studying & Categorizing MSDs Perceptual Eyes, ears, and hands Examples Prolonged /a/ Diodokinetic task /pataka/ Read grandfather passage Oral motor examination Methods for Studying & Categorizing MSDs Instrumental Acoustic methods Same data as perceptual = speech signal Provides quantification, description, and confirmation of human (clinical) perception Methods for Studying & Categorizing MSDs Instrumental Physiologic methods Study of movements of speech structures, air flow and air pressure, muscle contraction, nervous system, CNS and PNS activities in relationship to biomechanical activity and and CNS activity during speech planning and execution. Ex. Electromyography and aerodynamic measures Methods for Studying & Categorizing MSDs Instrumental Visual imaging methods Allows visualization of upper aerodigestive tract during speech Ex. Videofluoroscopy Nasoendoscopy Videostroboscopy (RE)VISITING NEUROANATOMY Speech Motor System The final common pathway Lower motor neurons The direct activation pathway Upper motor neurons (pyramidal system) Corticobulbar and corticospinal tracts The indirect activation pathway Cranial and spinal nerves Upper motor neurons (extrapyramidal system) The control circuits Basal ganglia and cerebellar Final Common Pathway Lower motor neuron system Brainstem and spinal cord muscles Includes: cranial nerves supplying muscles for phonation, resonance, articulation, and prosody; spinal nerves for respiration and prosody CN V (trigeminal), VII (facial), IX (glossopharyngeal), X (vagus), XI (accessory), XII (hypoglossal) Damage to lower motor neuron system Weakness Paralysis Diminished reflexes Decreased muscle tone Atrophy Fasciculations Flaccid dysarthria Direct Activation Pathway Upper motor neurons with direct, fast connection and influence on lower motor neurons Includes: corticobulbar tract (cortex to brainstem/cranial nerves); corticospinal tract (cortex to spine/spinal nerves) Damage to direct activation pathway Loss or reduction of skilled movement Unilateral upper motor neuron lesion = contralateral weakness Particularly of tongue, lower face Bilateral upper motor neuron lesion = bilateral weakness and alterations in muscle tone (spasticity) Normal reflexes UUMN, spastic dysarthria Indirect Activation Pathway Upper motor neurons with indirect influence on lower motor neurons Effects of damage: Increased muscle tone (spasticity) Hyperreflexia UUMN, spastic dysarthria Control Circuits Basal ganglia and cerebellum Coordinate, integrate, control movement activites Effects of damage Cerebellar control Ataxia, incoordination Intention tremor Dysdiodokinesia Ataxic dysarthria Basal ganglia control Hypokinesia (too little movement) Hyperkinesia (too much movement) Hypokinetic, hyperkinetic dysarthria What does this damage look like in speech? Flaccid (‘weakness’) Articulation: imprecise consonant production Phonation: breathy/hoarse voice quality, diplophonia, short phrases, weak cough or glottal coup, vocal flutter, audible inhalations (stridor) Prosody: monopitch, monoloudness Resonance: hypernasality, nasal emissions, weak pressure consonants Respiration: reduced loudness, short phrases, strained vocal quality Spastic (‘spasticity’) Articulation: imprecise consonant production, labored and slow production Phonation: harsh and/or strained-strangled vocal quality, low pitch, short phrases, pitch breaks Prosody: monopitch, monoloudness, slow rate Resonance: hypernasality Respiration: [shallow, slow inhalation] Ataxic (‘incoordination’) Articulation: imprecise consonant production, distorted vowels (slurred), irregular breakdowns Phonation: harsh vocal quality, voice tremor Prosody: equal and excess stress, prolonged phonemes and intervals between phonemes, monopitch, monoloudness, slow rate Resonance: [intermittent hyponasality] Respiration: exaggerated and/or paradoximal mvmt Hypokinetic (‘diminished movement’) Articulation: imprecise consonants, repeated phonemes, palilalia Phonation: harsh or breathy voice, low pitch Prosody: monopitch, monoloudness (low), reduced stress, inappropriate pauses, short rushes of speech Resonance: [mild hypernasality] Respiration: faster breathing rates, incoordination of muscles, shallow breath support, poor control of exhalation for speech Hyperkinetic (‘extraneous movement’) Articulation: imprecise consonants, distorted vowels, prolonged phonemes Phonation: harsh, strain-strangled, or breathy voice, excess loudness variation, voice stoppage Prosody: prolonged intervals between syllables/ words, variable rate of speech, monopitch, inappropriate silences, monoloudness Resonance: hypernasality and hyponasality Respiration: unexpected inhalations and exhalations Motor System Actions Motor Planning Motor Programming Motor Execution • • • • • • • • • • • • • Higher level Goal-oriented What to do Plans are inflexible Sets the plan for place & manner of articulation • Premotor cortex • Insular cortex Apraxia of Speech Lower level Procedure-oriented How to do it Modifiable via sensory feedback • Detailed program of motor acts across 5 speech systems • Basal ganglia • Cerebellum Lowest level Muscle oriented Do it Modifiable via sensory feedback • Executes muscle movements • Upper motor neurons • Lower motor neurons Dysarthrias VIDEO/AUDIO SAMPLES Questions/comments?