Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
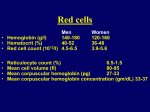
Rajiv Gandhi University of Health Sciences, Karnataka SYNOPSIS FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1. NAME OF THE CANDIDATE Mr. MANISH.SAXENA 2. NAME OF THE INSTITUTION Diana College of Nursing No 68,Chokkanahalli.Jakkur post Bangalore-64 3. COURSE OF STUDY AND SUBJECT Master Of Science in Nursing Community health Nursing 4. DATE OF ADMISSION TO COURSE 5. TITLE OF THE TOPIC 10-06-2010 Assess the effectiveness of structured teaching module on prevention of anaemia among adolescent girls in selected Govt. school, Rural Bangalore, Karnataka. 6. BRIEF RESUME OF THE INTENDED WORK INTRODUCTION Anaemia affects about 2 billion people worldwide. Inadequate iron intake is the primary cause of anemia, and contributes to 22 percent of maternal deathsand24percentofperinatal deaths. Anemia in childhood irreversibly compromises cognitive development, leading to lower school attainment and losses in productivity.. Thus, correcting anemia of any severity can have an impact on and child survival. Adolescents constitute about 25% of the population and form an important physiological group whose nutritional needs demand special attention. Adolescence is a period of rapid growth, weight gain and blood volume expansion. The overall iron requirement of the body increases during this period. During adolescent period, the risk of iron deficiency and anaemia among boys and girls appears to be more due to growth spurt, and in girls it remains as such during their reproductive life. Iron deficiency is the most widespread form of malnutrition among women and children. In India, anaemia affects an estimated 50% of the population. Numerous studies among adolescent girls have shown that the prevalence of anaemia is very high. Anemia is widely prevalent in India and affects both sexes and all age groups1. In India, pre-adolescent and adolescent girls, who constitute a sizable segment of its population, constitute a vulnerable group on account of the practice of early marriages and potential exposure to a greater risk of morbidity and mortality2. Adolescence is a crucial developmental period. In adolescent girls on a marginal diet, iron deficiency may be a routine consequence of growth and skeletal development. Further, low iron stores throughout childhood may contribute to a delayed menarche and impaired immune response3. India has one of the fastest growing youth populations in the world, with an estimated 190 million adolescents. Girls below 19 years of age comprise one quarter of India’s rapidly growing population. The majority is out of school and has limited choices available for the future. Girls are caught in the cycle of early marriage, repeated pregnancy and poverty. 6.1 NEED FOR THE STUDY Anemia afflicts an estimated two billion people worldwide, mostly due to iron deficiency. It primarily affects women.1 yet among adolescents, prevalence rates of anemia are closer for males and females in some parts of the world. The prevalence of anemia is disproportionately high in developing countries, due to poverty, inadequate diet, certain diseases, pregnancy and lactation, and poor access to health services. Young people are particularly susceptible because of their rapid growth and associated high iron requirements. Anemia is a critical health concern because it affects growth and energy levels. Adolescence is an opportune time for interventions to address anemia. In addition to growth needs, girls need to improve iron status before pregnancy.2,3 And both boys and girls are more accessible to information about anemia through schools, recreational activities, and via the mass media than they will be later in their lives. A significant percentage of adolescents in the developing world are anemic, causing considerable health consequences for this age group. About 27% of adolescents are estimated to be anemic in developing countries, compared to 6% in developed countries.4 Regional figures, although varying by country within the region, suggest the following prevalence rates for anemia: 5In Africa, 45% ,In Oceania, 45% ,In Latin America and the Caribbean, 12% for girls ,In Asia, 19% for girls In studies conducted by the International Center for Research on Women, country findings on adolescent anemia among both males and females include:6 High rates of anemia in Nepal (42%), India (55%), and Cameroon (32%) Moderate rates in Ecuador (17%) and Jamaica (16%) A 1997 survey of 12-18 year old girls in rural India found an anemia prevalence rate of 82.9% among girls in school and 92.7% among girls not in school.7 in a baseline survey conducted in Indonesia in October 1996, students showed a mean anemia prevalence of 29% for girls and 23% for boys.8 The health consequences of anemia in children and adolescents are well documented. In children, anemia affects physical growth and mental development. Other consequences— including reduced levels of energy and productivity and impaired immune system function—develop as children mature.9,10,11 Boys and girls both need iron for growth during adolescence, and girls have a continuing need to replace iron lost during menstruation.12,13 Anaemia is a serious public health problem that affects the ability to study and work as well as health and well being. It is one of the most prevalent nutritional deficiencies in the world, and more than half of the population in India is anaemic. The prevalence of anemia is as high as 70 – 80 per cent among children and 60 per cent among adolescents7. In the northern states of Uttar Pradesh and Jharkhand, anemia prevalence among preschool children is 74 per cent and 82 per cent respectively. Adolescence has been defined by the World HealthOrganization as the period of life spanning the ages between 10 to 19 years.4 this is the formative period of life when the maximum amount of physical, psychological, and behavioural changes take place. This is a vulnerable period in the human life cycle forthe development of nutritional anemia, which has been constantly neglected by public health programs. Girls are more likely to be a victim due to various reasons. Ina family with limited resources, the female child is morelikely to be neglected. She is deprived of good food and education, and is utilized as an extra working hand tocarry out the household chores. The added burden of menstrual blood loss, normal or abnormal, precipitates the crises too often. Girls often enter their active reproductive years in late adolescence with poor iron status. A great many girls in the world (at least 25%) will have had their first child by age 19, and great more shortly afterward.14 Because pregnancy requires more iron for increased blood production, an iron deficit can result in negative reproductive consequences.15 An estimated 47% of women of reproductive age in developing countries are anemic.16 During pregnancy, 59% are estimated to be anemic.17 Anemia during pregnancy isassociated with prematurity and low birth weight.18,19 Anemia is also related to perinatal and maternal mortality.20 The nutritional anemia in this group attributes to high MMR, high incidence of low-birth weight babies, high perinatal mortality and foetal wastage and consequent high fertility rates. This phase of life is also important due to the ever-increasing evidence that control of anemia in pregnant women may be more easily achieved if satisfactory iron status can be ensured during adolescence.2 it is very important to find effective interventions to prevent and control anemia in adolescents .Hence the researcher felt a need to conduct a study regarding the effectiveness of planned teaching programme on prevention of anemia among adolescent girls. 6.2 REVIEW OF LITERATURE A review of literature refers to activities involved in identifying and searching for information on a topic and developing and understanding the state of knowledge on the topic. Researchers never conduct a study in an intellectual vacuum their studies are usually undertaken within the context of an existing basic knowledge. The literature is reviewed and presented under the following headings 1. Literature related to general information on anemia 2. Literature related to incidence and prevalence of anaemia. 3. Literature related to causes and factors influencing anaemia 4. Literature related to prevention of anaemia. 5. Literature related to national health programmes on anaemia. 6. Literature related to role of nurse in prevention of anaemia 1. Literature related to general information on anemia Anaemia derived ;from Ancient Greek anaimia, meaning lack of blood is a decrease in number of red blood cells (RBCs) or less than the normal quantity of hemoglobin in the blood.[1][2] However, it can include decreased oxygen-binding ability of each hemoglobin molecule due to deformity or lack in numerical development as in some other types of hemoglobin deficiency. Because hemoglobin (found inside RBCs) normally carries oxygen from the lungs to the tissues, anemia leads to hypoxia (lack of oxygen) in organs. Because all human cells depend on oxygen for survival, varying degrees of anemia can have a wide range of clinical consequences. Anemia is the most common disorder of the blood. There are several kinds of anemia, produced by a variety of underlying causes. Anemia can be classified in a variety of ways, based on the morphology of RBCs, underlying etiologic mechanisms, and discernible clinical spectra, to mention a few. The three main classes of anemia include excessive blood loss (acutely such as a hemorrhage or chronically through low-volume loss), excessive blood cell destruction (hemolysis) or deficient red blood cell production (ineffective hematopoiesis). There are two major approaches: the "kinetic" approach which involves evaluating production, destruction and loss,[3] and the "morphologic" approach which groups anemia by red blood cell size. The morphologic approach uses a quickly available and low cost lab test as its starting point (the MCV). On the other hand, focusing early on the question of production may allow the clinician to more rapidly expose cases where multiple causes of anemia coexist. Anemia goes undetermined in many people, and symptoms can be minor or vague. The signs and symptoms can be related to the anemia itself, or the underlying cause. Most commonly, people with anemia report non-specific symptoms of a feeling of weakness, or fatigue, general malaise and sometimes poor concentration. They may also report dyspnea (shortness of breath) on exertion. In very severe anemia, the body may compensate for the lack of oxygen carrying capability of the blood by increasing cardiac output. The patient may have symptoms related to this, such as palpitations, angina (if preexisting heart disease is present), intermittent claudication of the legs, and symptoms of heart failure. On examination, the signs exhibited may include pallor (pale skin, mucosal linings and nail beds) but this is not a reliable sign. There may be signs of specific causes of anemia, e.g., koilonychia (in iron deficiency), jaundice (when anemia results from abnormal break down of red blood cells — in hemolytic anemia), bone deformities (found in thalassaemia major) or leg ulcers (seen in sickle cell disease). In severe anemia, there may be signs of a hyperdynamic circulation: a fast heart rate (tachycardia), flow murmurs, and cardiac enlargement. There may be signs of heart failure. Pica, the consumption of non-food based items such as dirt, paper, wax, grass, ice, and hair, may be a symptom of iron deficiency, although it occurs often in those who have normal levels of hemoglobin. Chronic anemia may result in behavioral disturbances in children as a direct result of impaired neurological development in infants, and reduced scholastic performance in children of school age. Restless legs syndrome is more common in those with iron deficiency anemia. Less common symptoms may include swelling of the legs or arms, chronic heartburn, vague bruises, vomiting, increased sweating, and blood in stool.Peripheral blood smear microscopy of a patient with iron-deficiency anemia. Anemia is typically diagnosed on a complete blood count. Apart from reporting the number of red blood cells and the hemoglobin level, the automatic counters also measure the size of the red blood cells by flow cytometry, which is an important tool in distinguishing between the causes of anemia. Examination of a stained blood smear using a microscope can also be helpful, and is sometimes a necessity in regions of the world where automated analysis is less accessible. In modern counters, four parameters (RBC count, hemoglobin concentration, MCV and RDW) are measured, allowing others (hematocrit, MCH and MCHC) to be calculated, and compared to values adjusted for age and sex. Some counters estimate hematocrit from direct measurements. WHO's Hemoglobin thresholds used to define anemia[5] (1 g/dL = 0.6206 mmol/L) Age or gender group Hb threshold (g/dl) Hb threshold (mmol/l) Children (0.5–5.0 yrs) 11.0 6.8 Children (5–12 yrs) 11.5 7.1 Teens (12–15 yrs) 12.0 7.4 Women, non-pregnant (>15yrs) 12.0 7.4 Women, pregnant 11.0 6.8 Men (>15yrs) 13.0 8.1 Reticulocyte counts, and the "kinetic" approach to anemia, have become more common than in the past in the large medical centers of the United States and some other wealthy nations, in part because some automatic counters now have the capacity to include reticulocyte counts. A reticulocyte count is a quantitative measure of the bone marrow's production of new red blood cells. The reticulocyte production index is a calculation of the ratio between the level of anemia and the extent to which the reticulocyte count has risen in response. If the degree of anemia is significant, even a "normal" reticulocyte count actually may reflect an inadequate response. If an automated count is not available, a reticulocyte count can be done manually following special staining of the blood film. In manual examination, activity of the bone marrow can also be gauged qualitatively by subtle changes in the numbers and the morphology of young RBCs by examination under a microscope. Newly formed RBCs are usually slightly larger than older RBCs and show polychromasia. Even where the source of blood loss is obvious, evaluation of erythropoiesis can help assess whether the bone marrow will be able to compensate for the loss, and at what rate. When the cause is not obvious, clinicians use other tests: ESR, ferritin, serum iron, transferrin, RBC folate level, serum vitamin B12, hemoglobin electrophoresis, renal function tests (e.g. serum creatinine). When the diagnosis remains difficult, a bone marrow examination allows direct examination of the precursors to red cells. Classification Production vs. destruction or loss is the most clinically relevant classification of anemia. This classification depends on evaluation of several hematological parameters, particularly the blood reticulocyte (precursor of mature RBCs) count. Red blood cell size In the morphological approach, anemia is classified by the size of red blood cells; this is either done automatically or on microscopic examination of a peripheral blood smear. Microcytic Microcytic anemia is primarily a result of hemoglobin synthesis failure/insufficiency, which could be caused by several etiologies: Macrocytic Megaloblastic anemia, the most common cause of macrocytic anemia, is due to a deficiency of either vitamin B12, folic acid (or both). Deficiency in folate and/or vitamin B12 can be due either to inadequate intake or insufficient absorption. Folate deficiency normally does not produce neurological symptoms, while B12 deficiency does. Normocytic Normocytic anemia occurs when the overall hemoglobin levels are always decreased, but the red blood cell size (Mean corpuscular volume) remains normal. Causes include: Dimorphic When two causes of anemia act simultaneously, e.g., macrocytic hypochromic, due to hookworm infestation leading to deficiency of both iron and vitamin B12 or folic acid [10] or following a blood transfusion more than one abnormality of red cell indices may be seen. Evidence for multiple causes appears with an elevated RBC distribution width (RDW), which suggests a wider-than-normal range of red cell sizes. Heinz body anemia Heinz bodies form in the cytoplasm of RBCs and appear like small dark dots under the microscope. There are many causes of Heinz body anemia, and some forms can be drug induced. It is triggered in cats by eating onions[11] or acetaminophen (paracetamol). It can be triggered in dogs by ingesting onions or zinc, and in horses by ingesting dry red maple leaves. Refractory anemia Refractory anemia is an anemia which does not respond to treatment. [12] It is often seen secondary to myelodysplastic syndromes. [13] Iron deficiency anemia may also be refractory as a clinical manifestation of gastrointestinal problems which disrupt iron metabolism. [14] Causes Broadly, causes of anemia may be classified as impaired red blood cell (RBC) production, increased RBC destruction (hemolytic anemias), blood loss and fluid overload (hypervolemia). Several of these may interplay to eventually cause anemia. Indeed, the most common cause of anemia is blood loss, but this usually doesn't cause any lasting symptoms unless a relatively impaired RBC production develops, in turn most commonly by iron deficiency.[15] (See Iron deficiency anemia) Impaired production Disturbance of proliferation and maturation of erythroblasts Increased destruction Further information: Hemolytic anemia Fluid overload Fluid overload (hypervolemia) causes decreased hemoglobin concentration and apparent anemia: Treatments Treatments for anemia depend on severity and cause. Iron deficiency from nutritional causes is rare in non-menstruating adults (men and postmenopausal women).. Mild to moderate iron deficiency anemia is treated by oral iron supplementation with ferrous sulfate, ferrous fumarate, or ferrous gluconate. When taking iron supplements, it is very common to experience stomach upset and/or darkening of the feces. The stomach upset can be alleviated by taking the iron with food; however, this decreases the amount of iron absorbed. Vitamin C aids in the body's ability to absorb iron, so taking oral iron supplements with orange juice is of benefit. Vitamin supplements given orally (folic acid) or subcutaneously (vitamin B-12) will replace specific deficiencies. In anemia of chronic disease, anemia associated with chemotherapy, or anemia associated with renal disease, some clinicians prescribe recombinant erythropoietin, epoetin alfa, to stimulate red cell production. In severe cases of anemia, or with ongoing blood loss, a blood transfusion may be necessary. Blood transfusions In severe, acute bleeding, transfusions of donated blood are often lifesaving. Improvements in battlefield casualty survival is attributable, at least in part, to the recent improvements in blood banking and transfusion techniques. Four randomized controlled clinical trials have been conducted to evaluate aggressive versus conservative transfusion strategies in critically-ill patients. All four of these studies failed to find a benefit with more aggressive transfusion strategies.[22][23][24][25] In addition, at least two retrospective studies have shown increases in adverse clinical outcomes in critically ill patients that underwent more aggressive transfusion strategies.[26][27] Hyperbaric oxygen Treatment of exceptional blood loss (anemia) is recognized as an indication for hyperbaric oxygen (HBO) by the Undersea and Hyperbaric Medical Society.[28][29] In 2002, Van Meter reviewed the publications surrounding the use of HBO in severe anemia and found that all publications report a positive result.[30] 2. Literature related to incidence and prevalence of anaemia. Early adolescence is a critical period for addressing anemia in both girls and boys. Adolescents can often be reached through educational and social activities. Existing settings such as schools and health facilities may offer opportunities to integrate nutrition education and actual services to reduce anemia. Nutrition awareness and education are particularly important given adolescents' poor knowledge of anemia, diet and health generally and of iron-rich foods specifically.21,22 Channels for reaching youth include A hematologic survey of 1,807 junior high school students in an urban area demonstrated a high incidence of anemia. Depending on the age of the student, the incidence of anemia among males ranged from 5.3 to 18.8 per cent and among females from 11.4 to 27.3 per cent. Analysis of red cell indices indicated that this anemia was hypochromic and microcytic and thus, presumably, a result of iron deficiency. Adolescence in India goes hand in hand with iron-deficiency anemia,says the latest NFHS report. While 56 per cent of adolescent girls are anemic, boys too are falling prey to the disease. Around 30 per cent of adolescent boys are suffering from anemia, the report states. The National Family Health Survey , conducted in 2005-06, presents the statistics that mark a growth in cases pertaining to anemia. Most of the anemic patients, especially women, suffer from mild to severe deficiency of iron. The hemoglobin count in most of the adolescent girls in India is less than the standard 12 g/decilitre, the standard accepted worldwide. In Uttar Pradesh alone, 85 per cent of children under the age of three years suffer from deficiency of iron, a leap of 11.3 per cent from the figures in NFHS 2, conducted in 199899. According to WHO estimates, India is one of the countries in the world that has highest prevalence of anemia. A study on the prevalence of anaemia was conducted among Jenukuruba primitive tribal children of Mysore district, Karnataka state. For the present study 175 children ranging in age group 6-10 years were selected and estimated the haemoglobin level by cyanmethaemoglobin method. The study revealed that, 36.57% of children were moderately anaemic, 26.29 per cent were mildly anaemic and 14.86 percent severely anaemic. On the whole 77.71% were suffering from differentforms of anaemia. Prevalence of anaemia was more among the girls than boys. A study was conducted to estimate the prevalence of anaemia among adolescent females and to study the socio-demographic factors associated with anaemia. A cross-sectional survey was conducted in an urban area under Urban Health Training Centre, Department of Preventive and Social Medicine, Government Medical College and Hospital, Nagpur. A total of 296 adolescent females were included in this study.. The Results shows the prevalence of anaemia was found to be 35.1%.. It was seen that anemia affects the overall nutritional status of adolescent females In an another multi country study on the nutritional status of adolescents carried out by the International Centre for Research on Woman, anaemia was found to be the widespread nutritional problem and its prevalence ranged from 32-55%. A study has conducted to find out the prevelance of anaemia in urban slums of NorthEast Delhi and reported the prevalence of anaemia among adolescent girls were significantly higher. A study was conducted on the prevalence of anaemia among school going girls and its relationship with various socio-demographic variable. To assess the magnitude of anaemia in school going, pre-adolescent and adolescent girls along with associated demographic variables. Prevalence of anaemia was 81.8% and had significant association with variables such as occupation of father, habit of post meal consumption of tea/coffee, consumption of green leafy vegetables and body mass index. Prevalence of anaemia necessitates pragmatic intervention to improve the dietary intake, nutritional supplement of iron and folic acid tablets. A study was conducted to assess the prevalence of anemia and determine serum ferritin status among 1120 apparently healthy adolescents sampled from 11 city and 2 rural schools in Chandigarh Anemia was observed more in rural (25.4%) as compared to urban (14.2%)adolescents (OR - 0.49, 95% CI - 0.34 to 0.70, P < 0.01). Iron stores estimated by serum ferritin in183 subjects were deficient in 81.7% and 41.6%of the adolescent girls and boys respectively. A study was conducted To investigate the severity and distribution of anemia among Indian adolescent girls aged 10 to 19 years and its association with socioeconomic and socio- demographic factors.. Results shows the highest prevalence of anaemia (99.9%) was observed in Jharkhand in eastern India.They concluded that Enhancement of the economic status of families, especially poor families, is a prerequisite to the amelioration of anaemia among adolescent girls. The level of education of the girls is also a major factor. A study was conducted on Two hundred sixty-five adolescent girls of Scheduled Caste community of Amritsar. The study showed that only 29.43% girls were normal and 70.57% were affected with various grades of anaemic condition, 30.57% girls being mildly anaemic and 27.17% moderately anaemic while12.83% suffered from severe anaemia. Severe anaemia had its wrath in age group 15.out of 265 girls studied, only 29.43% were normal and 70.50% were affected with various grades of anaemia.30.57% mildly anaemic, 27.17% moderately anaemic and 12.83% severely anaemic. High prevalence of anaemia has also been noted by various scientists among children of economically weaker sections and rural school children. A study was conducted on 177,670 girls aged 10 to 19 years. In this study, combined religion and caste into a single category to try to determine the effect of caste and religion socioeconomic and socio demographic , including place of residence ,age, educational status of the adolescent girls, house- bold standard of living, religion and ethnicity, region of the country, and marital status . .A total of 17 of 35 states or union territories had anaemia prevalence rates of more than 90% among adolescent girls. The study suggests an effect of socio-demographic factors in anaemia. A study was conducted to know the nutritional, anthropometric and dietetic status, the prevalence of anaemia, depletion of iron deposits and Vitamin A deficiency in female adolescents. Seventy-eight not pregnant female adolescents from an urban and a peri urban zone of Maracaibo, and a rural zone without infectious and inflammatory processes, were analyzed. Adolescents from the rural zone showed significant lower values of weight, height, body mass index BMI, and the highest prevalence of anaemia (66.67%), with respect to adolescents from the urban zone. The low iron status among adolescents from the rural zone determine that this is a high risk group to anaemia require prevention, control and supplementation strategies. 2. Literature related to causes and factors influencing anaemia. Adolescence is a “coming of age”, as children grow into young adults. These teen years are a period of intense growth, not only physically, but also mentally and socially. During this time, 20% of final adult height and 50% of adult weight are attained.1 Because of this rapid growth, adolescents are especially vulnerable to anemia. Proper nutrition, including adequate iron intake, plays an important part of your teenager’s growth and development. During adolescence, teenagers will acquire the knowledge and skills that will help them to become independent, successful young adults. Iron deficiency and iron deficiency anemia can affect this learning and development, but parents can help their teenagers stay healthy by teaching them some easy ways to prevent iron deficiency.Iron deficiency is the most common cause of anemia in adolescents in the United States, and an adolescent girl is 10 times more likely to develop anemia than a boy.2 Teenagers are at the highest risk of anemia during their adolescent growth spurt. Among girls, however, menstruation increases the risk for iron deficiency anemia throughout their adolescent and childbearing years.2 Boys, on the other hand, are at risk for anemia only during their adolescent growth spurt. Mexican-American teenagers and adolescents in lower-income homes are also at a higher risk. However, children from all backgrounds can develop iron deficiency and iron deficiency anemia.3-4 A study was conducted to determine the prevalence of anemia in a group of apparently healthy school adolescents selected from 2 distinct socio-economic areas (SEAs) in Baghdad; and to assess the importance of diet and some other factors which could be relevant in the epidemiology of anemia in adolescents.Results shows The prevalence of anemia among adolescents in HSEA was 12.9% compared with 17.6% in LSEA. Hemoglobin concentration in males was significantly correlated with age and dietary iron intake while in females it was correlated significantly with years of education of father and mother, number of pads and age at menarche.Anemia among adolescents was found to be a health problem of moderate severity. A study was conducted to assess the impact of socioeconomic and health related factors on the iron status of adolescent girls.These factors were studied in 180 girls aged 12 to 17 years living in two boarding schools from Pune. Results shows almost half the participants reported some health problems in the last four months before the study, whereas more than 75% auto-medicated before going to the hospital. The majority of the girls believed themselves to be in good health, although only 16% could define the term 'anaemia'. .girls whose mother was a manual worker, who came from a larger family and who auto-medicated , had a lower haemoglobin level, whereas girls who had started their menstruation had a lower SF level. Girls from a large family size and whose mother was a manual worker showed a higher risk of IDA. The findings indicate that iron deficiency is related to the occupation of the mother, family size, and auto-medication, Education. In an another study conducted to examine dietary pattern and nutritional status of adolescent college girls of Dhaka, Bangladesh with a particular focus on the prevalence of anaemia and appropriate knowledge about it among them. Sixty-five adolescent girls aged 15-19 years were selected randomly from Home Economics college of Dhaka. Results shows habitual dietary pattern indicated poor consumption of milk, liver and leafy vegetables.. The prevalence of anaemia among the participants was 23%. About 17% had low serum iron, 23% showed evidence of iron-deficient erythropoiesis. About 65% of the participants had correct knowledge about the causes of anaemia; while 72.3% and 80% respectively, knew about the prevention and treatment of anaemia. Surprisingly, 73.8% of the participants were not aware about the sources of iron-rich foods. A study was carried out in June and July 2007. Caregivers participated in a brief interview where demographic, health, and nutritional information was collected. A blood sample was collected from each adolescent, and haemoglobin levels were assessed with a point-of-care haemoglobin testing system. Results shows Three-quarters of adolescent were anaemic. Girls were significantly more likely to be anaemic than boys. Anaemic girls were significantly less likely to be underweight compared with their peers. Researchers found a striking prevalence of anaemia among clinically well girls. The rates of anaemia were higher than those found in previous studies conducted in similar settings in South Africa. 3. Literature related to prevention of anaemia. Education is fundamental to anemia reduction projects because adolescents have poor know-ledge about its causes and adverse effects. In a survey of adolescent girls in rural India, for example, more than one-half of the respondents did not know that diet is related to anemia and less than 5% mentioned excessive menstrual bleeding as a cause of anemia. Furthermore, 29% of the schoolgirls and 43% of the out-of-school girls had no knowledge of anemia's adverse effects.23 Iron supplementation projects have been tried in several types of settings. In the International Center for Research on Women's Guatemala metabolic study, researchers found that hemoglobin levels increased during iron supplementation but fell when a placebo was taken. This confirms the finding that while supplementation can rapidly improve iron status, continued interventions are necessary to maintain this improved status.25 Other studies/interventions showed some promising results. A MotherCare-supported study in India using a nutrition communication strategy to improve dietary intake and reduce anemia and undernutrition in early adolescent school girls was implemented over six months. A one-year post intervention evaluation showed significant increases in growth velocity, mean hemoglobin levels, anemia-related knowledge, and dietary behavior in the experimental, compared to the control, group.26 In Peru, a study supported by MotherCare comparing daily and intermittent supplementation in a group of adolescent girls showed that the prevalence of anemia significantly decreased with daily supplements, but there was no decrease among those receiving the intermittent dosage (2 days/week).27 In an U.S. clinical trial assessing the effects of iron deficiency on cognitive function, iron supplemented adolescent girls performed better on a test of verbal learning and memory than the control group.28 A birth survey in Nigeria found that pregnant adolescents who received antimalarial drugs and iron and folic acid supplements in the second half of pregnancy gained in height. Increased height is usually associated with a reduced incidence of cephalopelvic disproportion.29,30 In the U.S., a group of pregnant adolescents who received calorie, protein, vitamin and mineral supplements gave birth to infants with significantly higher mean weight than a group that received no supplements; larger effects were observed among girls under 16.31 A Helen Keller International project in Indonesia begun in 1996 will assess the impact of various strategies of improving iron status in girls. Three independent interventions— supplementation, a dietary approach and education—will be tested. The school setting will be assessed for its appropriateness as a channel for addressing adolescent nutritional problems.32 MotherCare is looking at effective ways to improve iron status among youth in India and Peru, and it is addressing anemia across broader age groups in many other countries.33 The following actions to reduce anemia in adolescents can be combined to fit different settings.24Reducing unwanted pregnancy (because pregnancy itself contributes to anemia) Educating and motivating young people about nutritional needs in schools, community settings, health venues, and through the media Increasing the iron content of food through dietary intake Increasing the iron content of food through fortification Increasing iron intake through supplement-ation Reducing blood loss by treating for parasites Reducing blood loss from hemorrhage by improving birthing or abortion practices and postabortion care A study was conducted to evaluate the effectiveness of. Universal supplementation of iron sulphate in the prevention of anaemia in adolescent girls between 2004 and 2005. .Universal supplementation with iron sulfate was effective in increasing serum Hb and decreasing risk of anaemia when administered on a daily basis. Improving the health of school-aged children can yield substantial benefits for cognitive development and educational achievement. A study was conducted to evaluate the impact of school-based anaemia prevention and enhanced literacy instruction on the health and educational achievement of school children in Kenya the primary outcomes are educational achievement and anaemia, the hypothesised mediating variables through which education is affected. A nested process evaluation, using semi-structured interviews, focus group discussion and a stakeholder analysis shows the community acceptability, feasibility and cost-effectiveness of the teaching in prevention of anaemia. A study was conducted to assess the prevalence of anaemia and determine serum ferritin status among 1120 apparently healthy adolescents sampled from 11 city and 2 rural schools in Chandigarh. All the boys and the girls were subjected to anthropometric examination and haemoglobin estimation.. The overall prevalence of anaemia calculated as per WHO Guidelines was significantly higher among girls as compared to boys Anaemia was observed more in rural as compared to urban .Result shows a high prevalence of anaemia among adolescent girls. 4. Literature related to national health programmes on anaemia. The strategies of the National Nutritional Anemia Control Program (NNACP) in India. The program, implemented through the Primary Health Centers and its subcenters, aims at decreasing the prevalence and incidence of anemia in adolescence. It focuses on three vital strategies: promotion of regular consumption of foods rich in iron, provisions of iron and folate supplements in the form of tablets to the high risk groups, and identification and treatment of severely anemic cases.. In October 1997, the Ministry of Health and Family Welfare in India organized a National Consultation on Control of Nutritional Anemia to review the epidemiology of nutritional anemia and the existing policy on nutritional anemia control. The programme was launched in 1970 to prevent nutritional anemia in mothers and children. Under this programme, the expected and nursing mothers as well as acceptors of family planning are given one tablet of iron and folic acid containing 60 mg elementary iron which was raised to 100 mg elementary iron, however folic acid content remained same (0.5 mg of folic acid) and children in the age group of 1-5 years are given one tablet of iron containing 20 mg elementary iron (60 mg of ferrous sulphate and 0.1 mg of folic acid) daily for a period of 100 days. This programme is being taken up by Maternal and Child Health (MCH), Division of Ministry of Health and Family Welfare. Now it is part of RCH programme. National programmes to control and prevent anemia have not been successful. Experiences from other countries in controlling moderately-severe anemia guide to adopt long term measures i.e. fortification of food items like milk, cereal, sugar, salt with iron. Nutrition education to improve dietary intakes in family for receiving needed macro/micro nutrients as protein, iron and vitamins like folic acid, B, B,C, etc. for hemoglobin synthesis is important. Nutritional Anemia Control Programme should be comprehensive and incorporate nutrition education through school health and ICDs infrastructure to promote regular intake of iron/ folic acid-rich foods, to promote intake of food which helps in absorption of iron and folic acid and adequate intake of food. The Ministry of Health and Family Welfare has revised the guidelines on IFA supplementation related to the National Nutritional anaemia Prophylaxis programme. This is the outcome of a long process, initiated with different consultations on anaemia in adolescent girls, the National Consultation on Micronutrients in end 2003 with ICMR/MHFW, work with the committee (chaired by DG ICMR) constituted subsequently and work with NRHM and different groups on the 11 th plan. Highlights of the same include the following The infants between 6-12 months should also be included in the programme as there is sufficient evidence that iron deficiency affects this age also. Children between 6 months to 60 months should be given 20mg elemental iron and 100 mcg folic acid per day per child as this regimen is considered safe and effective. National IMNCI guidelines for this supplementation to be followed. For children (6-60 months), ferrous sulphate and folic acid should be provided in a liquid formulation containing 20 mg elemental iron and 100mcg folic acid per ml of the liquid formulation. For safety reason, the liquid formulation should be dispensed in bottles so designed that only 1 ml cab be dispensed eachtime. Dispersible tablets have an advantage over liquid formulations in programmatic conditions. These have been used effectively in other parts of the world and in large scale Indian studies. The logistics of introducing dispersible formulation of Iron and Folic Acid should be expedited under the programme.The current programme recommendations for pregnant and lactating women should be continued.School children, 6-10 year old, and adolescents, 11-18 year olds, should also be included in the National Nutritional Anaemia Prophylaxis Programme (NNAPP).Children 6-10 year old will be provided 30 mg elemental iron and 250 mcg folic acid per child per day for 100 days in a year.Adolescents, 11-18 years will be supplemented at the same doses and duration as adults. The adolescent girls will be given priorityMultiple channels and strategies are required to address the problem of iron deficiency anaemia. The newer products such as double fortified salts / sprinkles/ ultra rice and other micro nutrient candidates or fortified candidates should be explored as an adjunct or alternate supplementation strategy. 5. Literature related to role of nurse in prevention of anaemia Educational settings - schools can incorporate nutrition education into family life education, health education, AIDS prevention courses, vocational training activities as well as organize sessions for out-of-school youth. Health facilities - health centers, clinics and hospitals can offer information about improving iron status. They can also provide services for anemia screening, reducing blood loss, and increasing iron intake (see actions below). Community outreach - peer education projects, workplace educational sessions, and social/ recreational activities can incorporate nutrition education into their programs. Media and public information - practical information about nutritional needs can be communicated to young people through all forms of mass media (TV, radio, print materials, movies) as well as by traditional media (plays, folk drama, fairs, puppet shows). In practice, nutritional education can be addressed within any setting or program that deals with reproductive and other health issues. Statement of the problem Assess the effectiveness of structured teaching module on prevention of anaemia among adolescent girls in selected Govt. school, Rural Bangalore, Karnataka. 6.3. Objectives of the study 1. To assess the pre-test knowledge regarding prevention of anaemia among adolescent girls 2. To assess the effectiveness of planned teaching on comparing the pre-test and post test prevention of anaemia by 4. To associate the post test knowledge of prevention of anaemia among adolescent girls in selected colleges, Bangalore with their selected demographic variables. Operational definitions In this study ASSESS: It refers to the statistical estimation of knowledge regarding prevention of anaemia among adolescent girls by using structured knowledge questionnaire. EFFECTIVENESS: It refers to the gain in knowledge as determined by the significant difference in pre-test and post-test knowledge and practice scores as elicited through structured knowledge questionnaire. KNOWLEDGE: it refers to the correct response of adolscent girls to the planned knowledge questionnaire on anaemia prevention. Hypothesis H1: There is a significant difference in the pre test and post test knowledge scores of adolescent girls regarding anaemia . H2: There is a significant association between the post test knowledge score of adolescent girls regarding prevention of anaemia. ASSUMPTIONS The adolescent girls may have knowledge on anaemia. Structured teaching programme is an effective way to improve the knowledge on prevention of anaemia. LIMITATIONS . 7. MATERIALS AND METHODS: 7.1: SOURCES OF DATA Adolescent girls studying in selected colleges in Bangalore. 7.2: METHODS OF DATA COLLECTION RESEARCH DESIGN AND APPROACH SETTING Pre - experimental , one group pre test post test design will be used. Study will be conducted in selected colleges in Bangalore POPULATION The population of the present study will be the adolescent girls SAMPLE Adolescent girls of selected colleges in Bangalore SAMPLE SIZE SAMPLING TECHNIQUE 60 Purposive sampling technique will be used to select the samples for the study. INCLUSION CRITERIA Adolescent girls those who are, Available during the time of collection. Willing to participate in the study data EXCLUSION CRITERIA Adolescent girls those who are, Who were not present DATA COLLECTION TOOL The tool for the data collection consists of two sections:Sec A: - A structured questionnaire to asses Socio-demographic Proforma of the study participants. Items on selected demographic variables like age, educational status, etc Sec B: - Structured knowledge questionnaire to assess the knowledge on anaemia prevention METHOD OF DATE COLLECTION Prior to data collection permission will be obtained from concerned authority. Consent will be obtained from the adolescent girls prior to the conduction of the study. Data will be administered collected knowledge by using self questionnaire to assess the knowledge and on the first day. The investigator delivers a STP on anaemia prevention on the same day. On the 7 th day post knowledge and practice will be assessed. DATA ANALYSIS METHODS. The collected data will be organized by 1. Descriptive statistics: Frequency distribution, percentage, mean, and standard deviation will be used to assess the demographic variables and the pre-test and post-test scores. 2. Inferential statistics: Paired t-test will be used to compare the pre-test and post- scores Chi-square test will be used to determine the association of post-test scores with the selected demographic variables. Analyzed data will be presented in the form of tables, diagrams, graphs based on the findings 7.3: DOES THE STUDY REQUIRED ANY INVESTIGATIONS OR INTERVENTION TO BE CONDUCTED ON PATIENTS OR OTHER HUMANS OR ANIMALS? IF SO, PLEASE DESCRIBE BRIEFLY. YES- pre test and post test will be conducted among staff nurses before and after structured teaching programme regarding Anaemia prevention 7.4: HAS ETHICAL CLEARANCE BEEN OBTAINED FROM YOUR INSTITION IN CASE OF 7.3? Yes informed consent will be taken from concerned authority of the institution prior to the study. Privacy ,confidentiality and anonymity will be guarded . Scientific objectivity of the study will be maintained with honesty and impartiality. Ethical Committee Title of the topic “A study to assess the effectiveness of planned teaching programme on prevention of anaemia among adolescent girls in selected colleges, Bangalore,Kartanaka” Name of the Candidate Mr.MANISH.SAXENA Course of the study and subject M.Sc. (N) 1st year. Community health Nursing. Prof. Veda Vivek Head of the Department Name of the guide Department of Community Health Nursing, Diana College of Nursing, Bangalore – 64. Ethical committee Members of Ethical committee: 1. Prof. Veda vivek Principal and HOD Department of Community Health Nursing Diana College of Nursing, Bangalore – 64. 2. Prof. Elizabeth Dora Head of the Department Department of Child Health Nursing Diana College of Nursing, Bangalore – 64. 3. Prof. Kalaivani Head of the Department Department of Obstetrics and Gynecological Nursing Diana College of Nursing, Bangalore – 64. 4. Prof. Vasantha Chitra.D Head of the Department Department of Medical Surgical Nursing Diana College of Nursing, Bangalore – 64 5. Prof. Kalai Selvi. S. Head of the Department Department of Psychiatric Nursing Diana College of Nursing, Bangalore – 64. 6. Prof. Rangappa Biostatistician GKVK, Jakkur International Airport Road Bangalore 1. 8. List of references 1. Latham MC. Human nutrition in the developing world.Rome: FAO, 1997: 147-55. 2. World Health Organization. Pregnancy and abortion in adolescence. Geneva: WHO, 1975; 583. 3. Barbin L, Barbin BJ. The cost of successful adolescent growth and development in girls in relation to iron and vitamin A status. Am J of Clin Nutr 1992; 55: 955-8. 4. World Health Organization. Programming for adolescent health and development. WHO Tech Rep Ser No. 886,1996. p. 2. 7. Ministry of Health and Family Welfare, Government of India. National Family Health Survey-III(NFHS-III), 2005-2006: India. Vol. 1. New Delhi: MoHFW. 2007 9.Signature of candidate . 10. Remarks of the guide 11.Name and designation of guide Prof. Veda Vivek. Head of the Department Department of Medical Surgical Nursing, Diana College of Nursing, Bangalore – 64. Signature Prof. Veda Vivek HOD Head of the Department Department of Medical Surgical Nursing, Diana College of Nursing, Bangalore – 64. Signature 12. Remarks of the Chairman & Principal Signature