Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
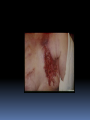
PHOTODYNAMIC THERAPY FOR BREAST CANCER Ron R. Allison, M.D. Medical Director 21st Century Oncology 801 WH Smith Blvd. Greenville NC USA 27834 252-329-0025 [email protected] Why PDT for breast cancer PDT has wide ranging success for various cutaneous lesions PDT offers excellent cosmesis PDT is non- carcinogenic PDT part of a multidisciplinary approach Clinical applications Primary therapy - PD/PDT - post excision for margins Salvage Therapy - Chest wall recurrence - metastatic lesions (of bone) Clinical applications Primary disease: No peer reviewed publications Salvage Therapy: Multiple publications PDT- CHESTWALL FAILURE FROM BREAST CANCER ECU Experience: R. Allison, R. Cuenca, G. Downie, C. Sibata 95 % DFS in advertisements… How about the forgotten 5%? Chestwall Failure Physiologic Lesions are painful, bleed, become infected, itch Dermal lymphatics spread everywhere Psychologic Watch tumors grow QOL stinks Initial Salvage Surgery for XRT failure XRT for surgical failure Chemo- as chestwall failure bodes for systemic disease However, a significant number of pts have continued chestwall failures despite several salvage attempts… Surgery XRT Chemo :Chestwall resections & reconstructions : 90% failure at surgical borders : Maximum dose is a reality : Rib fx, fibrosis, pneumonitis : 3rd line agents don’t give CR on chest wall PDT for Chestwall Works on cutaneous malignancies Literature shows good cosmetic and tumor response Does not stop other therapies Outpatient Minimal tx toxicity/discomfort Repeatable Clinical PDT for Chestwall 2 Distinct Systems: 1) High drug and lower light dose (directed at tumor) 2) Low drug and higher light dose (not as directed at tumor as you think) High Drug/Lower Light High Drug Normal 0000 000 0 Tumor 0000 000 0 000 0 Normal 0000 000 0 Lower Drug/High Light Low Drug Normal 0000 Tumor 0000 000 0 000 0 Normal 0000 Clinical Trials Author N Drug Light(J/cm2) Response Significant Morbidity Bandermonte 4 3mg 120 75% 75% RPCI 6 2 mg 75 75% 75% 6 1 mg 150 75% 25% 6 0.6 mg 30-240 0% 0% Allison/Mang 9 0.8 mg 150 90% 0% Taber 7 2 mg 100 90% 50% ECU 14 0.8 mg 150 90% 1 pt Chestwall PDT 50 Women with biopsy proven chestwall disease Age 43-70 No pt. lost to follow-up Range 3-18 months Initial Treatment Mastectomy and Chemo/Hormones: Lumpectomy + XRT + Chemo/Hormones: 1st Failure Mastectomy: XRT: Chemo: 2nd Failure XRT: Surgery: Chemo: At Presentation at ECU 44 pts on narcotic analgesics 40 pts with itching lesions 20 pts with open wound due to tumor All were progressing on chemotherapy 45 systemic mets (asymtomatic in all) PDT Photosensitizer : Off label Photofrin, 0.8 mg/kg Illumination : 632 nm diode laser Tx Protocol : 0.8 mg/kg Photofrin followed 48 hrs later by outpt illumination at 150 J/cm2 PDT Treatment 2215 lesions treated Outpatient therapy Sessions of 3-6 hours Ice patches used if illumination caused tenderness Results 91% CR- Defined as total lesion elimination with healing 9% PR- Defined as >50% reduction in lesions size without growth Minimum f/u 3 months (median=9 months) Treatment Findings All pts underwent outpatient therapy w/o complications All therapy given as prescribed No photosensitivity reaction Pain control is excellent Itching and symptoms removed Conclusions PDT is well tolerated Response is excellent Morbidity is acceptable The drug and light dose used offers good outcome PDT does not stop additional therapy if needed. Summary PDT can offer excellent palliation Outpatient procedure Pts who have had extensive surgery, XRT and chemo can respond well and heal Use PDT earlier in treatment course Treatment Day 3 months followup Other PS used for breast cancer * Purlytin Allison: 9pts, 1.2 mg/kg, 90% CR, minimal morbidity * Foscan Wyss: 7pts, 0.15 mg/kg, 90% response, 90 % morbidity (tissue slough) *Phthalocyanine (Pc4) Oleinick: 2pts, .135 mg/m2, Minimal response *Motexafin Lutetium Hahn: 5pts, 5 mg/kg, morbid Breast Surg, XRT: Excellent local control PDT to lumpectomy bed + XRT to breast PDT to lumpectomy bed alone! PDT to chestwall even in heavily pre-txd tissue: Excellent local control and cosmesis PDT for Dx via fluorescence Many questions on dose, timing, and technique Immune modulation via PDT?!