Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
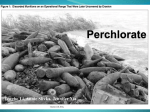
Is a Perchlorate Clean-up Necessary? 5 by Tengbo Li, Annie Slivka, and Jennifer Xia Quantitative Methods in Public Policy Decisions Professor Richard Wilson January 2009 Introduction Perchlorate (ClO4-) is used as an oxidizer in rocket fuel, explosives, flares, and fireworks. The United States Department of Defense (DoD) has used the chemical since the 1940s, citing its "high ignition temperature, controllable burn rate, and stable chemical characteristics," which minimize the chance of accidents during handling and storage.4 In the private sector, firms that specialize in aerospace technology, like Aerojet and Lockheed Martin, also use perchlorate extensively. The DoD and such firms typically dispose of perchlorate by dumping large amounts of the chemical into local water supplies. As a result, concentrations of perchlorate in water supplies across the United States have increased drastically, particularly in the West and Southwest. Perchlorate concentrations of 100,000 ppb and higher have been found.5 Of the 3,700 public drinking water systems across the United States, 153 have high enough concentrations of perchlorate to be considered "contaminated."5 Perchlorate has been shown to pose a significant human health risk, as it interferes with the transport of iodide into the thyroid. Iodide is essential to the production of T3 and T4, hormones which play an important role in the development of the central nervous system and skeletal growth in fetuses and infants. In addition, T3 and T4 regulate metabolic activity and affect nearly every organ system in the human body. Perchlorate prevents the production of T3 and T4 by binding competitively with the sodium-iodide symporter (NIS protein), which has a higher affinity toward perchlorate than to iodide. Sufficiently high levels of perchlorate in the body can cause developmental problems, especially in infants (via lactation) and fetuses (via the placenta), resulting in mental retardation, and lower IQ and motor ability.2 The Environmental Protection Agency's recommended perchlorate level in water, 24.5 ppb, has been in effect since 2005. However, numerous water supplies around the United States continue to have levels of perchlorate exceeding the recommended level. This is mainly due to the high cost of removing perchlorate from the water; a thorough cleanup of contaminated drinking water throughout the United States would cost billions of dollars. Recently, the EPA has recommended an even lower safe level of 1 ppb. Cleaning the highly-contaminated Colorado River system alone to meet this standard would cost $40 billion.12 Until significantly more cost-effective methods of treating perchlorate are discovered, a mass cleanup of perchlorate to meet EPA standards would be expensive and ultimately futile. A new study released by the Office of the Inspector General of the EPA on December 30, 2008 further supports our conviction that a mass cleanup is not the correct method of addressing the issue. The new study reveals that lowering perchlorate levels in drinking water only slightly improves human thyroid function.13 It also reveals that even setting extremely conservative levels of perchlorate intake would not necessarily "prevent mental damage in children."13 In addition, the study indicates that factors that were not included in the NAS study, such as the presence of other dangerous chemicals in drinking water, may pose much stronger risks to humans than perchlorate.13 Addressing these other factors may prove to be far more beneficial to human health than cleaning up perchlorate alone. A thorough cleanup of perchlorate in the environment, particularly around sources of drinking water and farm land, would be ideal for human health. However, due to the high costs and relative lack of benefits of reducing perchorate levels in drinking water, we strongly recommend against a mass cleanup. We advocate a more reasonable solution: to implement a new law requiring the safe removal and storage of perchlorate waste. Background Perchlorate is a chemical compound that is both naturally occurring and manufactured for use in many products, such as: rocket fuels, missiles, matches, dyes, paints explosives, flares, and fireworks, employed in large part because it is the least reactive oxidizer of the generalized chlorates. As Alex Beehler, the Assistant Deputy under the Secretary of Defense, explains it, "Since the 1940s, Department of Defense has used potassium and ammonium perchlorate as an oxidizer in explosives, pyrotechnics, rocket fuel, and missiles. If it by far the safest, most efficient and stable propellant oxidizer available. Perchlorate has a high ignition temperature, controllable burn rate, and stable chemical characteristics that reduce handling and storage risks and the likelihood of unexpected detonations." 4 1 Perchlorate is also highly soluble, or easily dissolved and transported in water, which means that if allowed to contaminate free water sources, it can very easily spread and infiltrate large quantities of water in all its capacities: groundwater, surface water, as well as soils and other mediums that contain large amounts of water. Studies have found perchlorate to have contaminated at least 400 groundwater sites and well as 153 of the 3,700 public drinking water systems in the United States at levels of anywhere from less than 1 part per billion to more than 3.7 million parts per billion, however most sites did not have high levels of perchlorate. 70% of the contaminated sites had less that the 24.5 parts per billion reference dose set by the EPA, while only 14 of the 153 public water systems had concentration levels above this reference level. While it is noted that due to faults in tracking and testing for perchlorate, there are many possible undetected sites, most are expected to have low levels of concentration, very few are expected to have significantly risky levels.1 Consumption of Perchlorate The FDA conducted a study in 2004-2005 to try and determine the amount of perchlorate consumed. It gathered produce data from areas of reportedly high perchlorate, such as Southern California and Arizona, and data for beverages from across the country. Figures of interest include spinach and collard greens at 115 and 92.4 ppb, respectively, and milk and bottled water at 5.81 and less than 0.5 (non-detected in all samples) respectively.6 6 In a 2007 analysis of the risk of perchlorate consumption, taking into account such variables such as methods and frequency of consumption of certain foods, the FDA proceeded to analyze the data from the 2004-2005 exploratory study and determined estimated perchlorate exposure to be 0.053 microgram/kg-day for all people 2 and older, primarily due to milk and then tomato consumption. The other two population groups, chosen as sensitive subgroups, included in the study were children 2-5 years of age and females 15-25, which had estimated mean perchlorate intakes of 0.17 and 0.037 microgram/kg-day, respectively.7 6 This estimate is similar to the estimated dose of 0.066 micrograms of kilograms of body weight per day for the U.S. population aged 20 and older in Blount et al. based on a study of adjusted geometric means of urinary levels in 2,820 participants. The 95th percentile in adults was at .234 microgram/kg-day, and only 11 adults out of the 1618 subjects had over the recommended EPA reference dose. This same study also estimated the population of pregnant women to also have an estimated median perchlorate dose of 0.066 micrograms/kg-day.8 Health Risk Perchlorate, like any chemical, has many temporary effects in large amounts, everything from itching, tearing, and pain to gastroenteritis to eventually ringing of the ears, dizziness, elevated blood pressure, blurred vision, and tremors; however, the main issue in question is how much perchlorate is required to cause chronic disorders, namely metabolic disorders of the thyroid. 5 Studies have not yet found any other chronic effects of increased levels of perchlorate in the adult body, but there have been links to impairment of the development of skeletal and nervous systems in infants. Perchlorate and the Thyroid The thyroid gland produces two hormones: triiodothyronine (T3) and thyroxine (T3). Thyroxine is a precursor hormone with little or no intrinsic biologic activity, but it is converted both in the thyroid and in other organs, into triiodothyronine. They are crucial in metabolic activity and affect almost every organ system in the body. Furthermore, T3 is required for fetuses and infants to insure normal development of central nervous systems as well as skeletal systems.2 2 Iodide plays an essential role in the synthesis of T3 and T4, because its element, iodine, is a component of both molecules. It can only be gained through consumption: the World Health Organization recommends 150 micrograms/day for adults, 200 for pregnant women, 90-120 for children 2-11, and 50 for infants under 2.2 2 It is transported into the thyroid by a protein molecule called the sodium/iodide symporter, or the NIS protein. However, the NIS protein will also bind with other ions, like perchlorate. The problem is that the NIS protein actually has a higher affinity to binding with perchlorate than iodide, which means that at high levels, perchlorate can dramatically reduce the movement of iodide into the thyroid gland. 2 9 On the other hand, thyroid hormone production and secretion are closely regulated by the hormone thyrotropin (thyroid-stimulating hormone, TSH) by the pituitary gland which stimulates virtually every step of the process. The pituitary gland increases secretion of TSH when serum levels of the two hormones are low (hypothyroidism), and decreases secretion when serum levels are high (hyperthyroidism). There are also few if any symptoms of temporarily low T3 and T4 levels, besides the possibility of an enlarged thyroid gland. In addition, 80% of conversion from T4 to T3 occurs outside of the thyroid, especially in the brain, so with increased levels of TSH, conversion rates outside the thyroid can increase significantly regardless of the effects of perchlorate on the thyroid. Thus, only daily iodide intake of below about 10 to 20 micrograms will cause hypothyroidism. However, it is still debated how low hormone levels must drop and for how long to cause adverse health effects. There is potential that sensitive populations, such as people with thyroid disorders, pregnant women, fetuses and infants, there is an increased risk of adverse health effects.2 Hypothyroidism in fetuses and infants In fetuses and infants, T3 is necessary for the development of many crucial structures in the nervous and skeletal systems. It stimulates the development and growth of neurons, glial cells, synapses between neurons, myelin sheaths that surround neuronal processes, and neurotransmitters as well as the transcription of “several genes whose products are important for neural development”. Additionally, it is necessary for the normal growth of long bones and the production of the pituitary growth hormone and an insulin-like growth factor.2 Fetuses receive all their iodide from their mothers; thus “the consequences of severe combined maternal and fetal hypothyroidism during fetal life and in newborn infants include microcephaly (small brain), mental retardation, deaf-mutism, paraplegia or quadriplegia, and movement disorders. Those abnormalities are not reversible by treatment with T4.” Additionally, "newborn infants who have hypothyroidism may have other abnormalities, including lethargy, poor muscle tone, poor feeding, constipation, and persistent jaundice, if not at birth then thereafter. The changes are similar to those which occur in older children and adults who have hypothyroidism, and, in contrast with the neurologic abnormalities, they are reversible with adequate T4 treatment." 2 Key Studies: Because of the health risks associated with perchlorate intake, various studies have been conducted to determine a level of perchlorate intake by humans which would have no adverse health effects. The Greer et al. study of 2001 examined the effects of perchlorate exposure in healthy adult humans over a 14-day period. Male and female volunteers were given perchlorate in drinking water in the following doses: 0.007, 0.02, 0.1, and 0.5 mg/kg-day.14 Greer et al. measured the iodide uptake before exposure to perchlorate, on the second day of exposure, the fourteenth day of exposure, and the fifteenth day (the day after the final exposure). Greer et al. determined that perchlorate ingestion had little effect on thyroid function, except in the case of 0.5 mg/kg-day.14 On the fifteenth day, however, thyroid function returned to normal even in individuals exposed to a level of 0.5 mg/kg-day. Greer et al. concluded that the "true noeffect level" was either approximately 0.0052 or 0.0064 mg/kg-day, based on two methods of calculation.14 In 2005, the National Academy of Sciences (NAS) conducted another study to determine a no-effect level. The NAS study determined that this level was 0.0007 mg/kg-day, a factor of ten less than the original Greer study. This new no-effect level was based on the Greer et. al. study. Using Greer et al.'s recommended level of 0.007 mg/kg-day, the NAS included an uncertainty factor of 10 to account for pregnant women, fetuses, and infants, the portion of the population most susceptible to the health hazards associated with perchlorate.2 The NAS considered other uncertainty factors, including the effects of long-term exposure, but concluded that such factors were negligible. Based on the recommendations of the NAS, the Environmental Protection Agency (EPA) set 24.5 ppb (the equivalent of 0.0007 mg/kg-day) as the suggested maximum concentration level of perchlorate in drinking water. Most recently, on December 30, 2008, the Office of the Inspector General (OIG) of the EPA released a new study that questioned the NAS findings and subsequent EPA regulation. The new study rejects the NAS findings on the basis that the NAS did not consider chemicals like thiocyanate and nitrate in their evaluation of the risk of perchlorate contamination. The new study argues that thiocyanate and nitrate, despite being present in lower concentrations than perchlorate in drinking water, are up to twelve times more potent than perchlorate in inhibiting thyroid function. Additionally, the new study shows that reducing perchlorate from a level of 24.5 ppb to even 6 ppb, a 4-fold reduction, would only improve maternal thyroid intake 1%.13 Perhaps most importantly, the new study examines the impact of lack of iodide in the diet on thyroid function, revealing that low levels of iodide in the diet can have an inhibiting effect on the thyroid 50 times stronger than that of perchlorate contamination alone.13 While the OIG study does not show that setting the perchlorate concentration level at 24.5 ppb level is necessarily misguided, the OIG study does point to other issues of concern, foremost being the lack of iodide intake, which affects nearly 7% of, or 276,000, American infants born each year. Lack of iodide intake in the diet leads directly to T4 deprivation, and consequently to problems such as lower IQ, ADHD, and lower motor performance.13 We can address lack of iodide intake effectively by providing low-cost iodide screening for pregnant women. We recommend that doctors inform pregnant women about the risks of low iodide intake and encourage them to consider preventative measures such as iodide supplements and highiodide content foods. The OIG study further reinforces the thesis that a mass cleanup would be ineffectual. A 1% increase in iodide intake via the reduction of perchlorate levels in drinking waters, which presents no measurable decrease in terms of the risk of perchlorate-associated problems, is hardly worth the billions of dollars it would cost to perform a mass cleanup. Methods of removal: If a clean-up of perchlorate were deemed necessary, there are three different ways possible, but none efficient for vast usage. Mainly, the chemical itself is not very reactive to chemical treatments such as removal by a “reducing agent.” The chemical characteristics of perchlorate do not encourage new methods of removal to develop and make it virtually impossible to remove low levels of perchlorate from water. Secondly, the characteristics of the soil and water that the perchlorate contaminates varies from site to site also make it impossible to use the same technology at all sites, especially if other chemicals are also contaminating the same soil or water. 10 At the moment, there are three ways to remove perchlorate: “biological and biochemical reactor treatment systems, conventional chemical reactor treatment systems, and separation and concentration technology.” Until better technology is found, most removal is currently being done by “Biological treatment and ion (anion) exchange systems.” Under this treatment, microbes convert perchlorate into chloride and oxygen. To do this, "anoxic conditions" are needed along with alcohol or another "electron donor to sustain the microbes." The removal would most likely happen by flowing the contaminated groundwater through a tank that contains the microbes. The system is potentially viable in the long term as it does not have any "waste resin" and is "less expensive than ion exchange." However, biological treatments are not an accepted practice on drinking water in the United States (though they are used in California where perchlorate levels have gone down from 2500 ug/l to 4 ug/L). 10 The other most prevalent method of removal currently is the "ion exchange system" which removes perchlorate ions by replacing them with chloride ions. This system may be the answer for potential clean-ups as unlike the biological treatment system it is potentially viable over more conditions, is produced by more than one manufacturer, and is accepted for use on drinking water. However, this system does not "destroy" the perchlorate, but just removes it: this system leaves behind a waste product which then must be disposed of. This makes this system more expensive; though more testing and technology is currently being done that may lower costs. Overall, there are many potential ways to remove perchlorate, but no clear effective method that funding is available for.10 Who would be held responsible? A number of private corporations could be found liable for their unrestricted use of perchlorate and forced by the courts to pay for the perchlorate clean up. One example is at the Kerr-McGee Chemical Corporate in Nevada: this chemical plant is located near the Colorado River whose drinking water is used by twenty million. Perchlorate has been found in “higher than expected” amounts in 38 milk samples and 67 out of 78 lettuce samples taken far downstream from the plant. Experts estimate that river sentiments contain about twenty million pounds of perchlorate at this point and will remain contaminated for the next fifty years. In a river that serves so many for drinking water, this is not good news. Another pertinent example is also in Nevada at the American Pacific Plant, the sole current producer of the chemical in the US. This plant produces about 20 millions pounds each year of perchlorate and as a result in the ground near the factory perchlorate is found in levels up to 750,000 ppb. This high concentration descends three hundred feet below the plant and “through five groundwater layers.” Former workers describe the “careless handling” of the chemical and "disposal ... in a trench on the factory site, and washing down the plant-creating a pond of contaminated water called 'lake louise." Very few companies have paid damages or truly privately changed their ways. The defense corporation Lockheed Martin did spend $80 million to clean up one site in 1998 and has pledged another $180 million over the next twenty years over fears of liability. No major court case has taken place yet.11 Considering that roughly ninety percent of perchlorate in the U.S. is manufactured for or used by the military and NASA,5 the defense department would be responsible for the almost all clean-up costs rather than the private companies listed above. After all, perchlorate is used for rocket fuel and, therefore, the defense department is responsible for discarding, and just leaving, missiles to close to ground water. This would most likely result in the Department of Defense spending between 16 and 165 billion dollars.5 This cost estimate varies so greatly as the Defense Department does not have an efficient way of monitoring which areas are contaminated as each sub-agency (the navy, army, etc) has a different way of counting areas and has different assumptions in their classifications of contaminated land. Depending on which agency, different levels of concentration of perchlorate and different testing methods are used to determine how many contaminated sites there are. Further, one acre of clean up varies from 800 to 7,600 dollars depending on which agency owns that acre. Considering that the Defense Department has about 24 million acres of possible clean up and there might be more unreported acres, a better record and testing system is needed to fully understand the cost burden that clean up would place on the Department of Defense.5 This huge amount of capital required to start clean up is not exactly realistic for a department that spends 12 billion a month in Iraq. Thus, the Defense Department has not made any solid effort to clean up yet. They have made some recent strides to test new sites and have promised that they will act if they find any site above the appropriate level. For example, the Defense Department proudly boasts that one site’s groundwater that they cleaned up is completely fine now. The Department has also pledged 114 million dollars to find new ways to recycle perchlorate, detect it, and create substitutes. One substitute for military operations was scheduled for manufacture in 2008, though unclear if this has happened.4 114 million dollars is a good start for the Department, but is not very much compared to lowest estimated cost of a potential clean up: 14 billion. Until better technology is created to treat contaminated sites most cost effectively, the EPA will likely have little chance to make the Department of Defense fund the clean up. Cost-Benefit Analysis: If the Department of Defense were willing to pay for the clean-up, the clean-up may not even be a socially efficient cost. 276,000 infants are born each year in the U.S. at risk as their mother’s have low T4 levels. Cost of screening all adults for hypothyroidism is only the cost of a simple blood test, Radioimmunoassay (RIA), which depending on availability costs around just $5. Additionally, the CDC estimates that 44 million women are at risk with low iodine levels. For those 44 million to develop complications from perchlorate, current studies offer significant support that they must be in an environment of consistently high exposure to perchlorate. In the case that all these conditions are met and they do develop hypothyroidism, there are drugs like Levothyroxine, a pure synthetic T4 drug, that have already been developed for other wide-ranging causes of hypothyroidism. Cost estimates for Levothyoxine are about $120 a year for the rest of their life, and even this might be unecessary.15 As hypothyroidism is not a chronic illness, in the case of perchlorate obstruction, studies point toward the simple solution of increasing iodide intake to cure the illness at very low general costs.16 It is unclear exactly how much medical costs would be with no cleanup, but based on these rough numbers, we can postulate a total significantly lower than the billions needed for the clean-up. 2 We came to a primitive conclusion on clean-up costs based on a couple basic calculations. From the range of $16-165 billion Defense of Department (see Who should be held responsible?), we based our approximation on about a $100 billion expenditure for full perchlorate clean-up.5 We also calculate approximately 84% of all perchlorate contamination linked to the Department of Defense, (see table in Background) from the estimates of about 90% of all perchlorate manufactured (21% of all perchlorate activity) for the Department of Defense in addition to the 65% of all perchlorate activity attributed to the Department of Defense, NASA, and other defense industries. Thus, using simple cross-multiplication (.84/$100=1.00/x) we estimate that total clean-up costs would lie somewhere around $120 billion. Conclusion: Therefore, we recommend that four actions be taken. One, areas of high concentration should be cleaned. There are very few in the nation with hundreds of thousands particles per billion of perchlorate. These Defense Department and private sites along with the other 14 drinking water systems that have thus far been identified should be cleaned immediately. Sites with low contamination, on the other hand, do not necessitate a federal mandate to be cleaned. Thus, secondly, instead of cleaning up all sites, a better cross-agency monitoring system for the remaining sites should be developed. The EPA and DoD should be required to work together to keep our water safe.1 Thirdly, safe storage and disposal should be required of both private manufacturers and the Defense Department. Leaving used munitions next to rivers should not be acceptable, and legislation should be used to enforce this. Lastly and perhaps most importantly, all women, and not just those who are identified as at-risk women, should be screened for low-iodine levels as a measure to stop the easily preventable and highly deleterious effects of low-iodine levels in fetuses, namely developmental restrictions in skeletal and nervous systems. Overall, perchlorate is dangerous in high concentrations, has significantly contaminated some of our sources of drinking water, but with proper monitoring and responsible actions can be dealt with efficiently and economically. Works Cited 1. “Perchlorate: A System to Track Sampling and Cleanup Results is Needed.” United States Government Accounting Office: Report to the Chairman on Environment and Hazardous Materials, Committee on Energy and Commerce, House of Representatives. May 2005. GAO-05-462. www.gao.gov/cgi-bin/getrpt?GAO05-462. 2. Johnston, Richard B. Jr and et al. Health Implications of Perchlorate Ingestion. Washington, National Academy of Sciences, 2005. http://www.nap.edu/catalog/11202.html. 3: Blount, Pirkle, Osterloh, Valentin-Blasini, and Caldwell. "Urinary Perchlorate and Thyroid Hormone Levels in Adolescent and Adult Men and Women Living in the United States". Environmental Health Perspectives. Volume 114, Number 12. December 2006. http://www.ehponline.org/members/2006/9466/9466.pdf. 4. Beehler, Alex. Statement of Mr. Alex Beehler Assistant Deputy under Secretary of Defense (Environment, Safety, & Occupational Health) Before the Subcommitte on Environment and Hazardous Materials of the House Energy and Commerce Committee April 25, 2007. http://energycommerce.house.gov/cmte_mtgs/110ehm-hrg.042507.Beehler-testimony.pdf. 5. “DOD Operational Ranges: More Reliable Cost Estimates and a Proactive Approach to Identifing Contamination are Needed.” United States General Accounting Office: Report to Congressional Requesters. May 2004. (GAO-04-601) www.gao.gov/cgi-bin/getrpt?GAO-04-601. 6. “2004-2005 Exploratory Survey on Perchlorate in Food” U.S. Food and Drug Administration: Center for Food Safety and Applied Nutrition: Office of Plant & Dairy Foods. Updated May 2007. http://www.cfsan.fda.gov/~dms/clo4data.html. 7. “Preliminary Estimation of Perchlorate Dietary Exposure Based on FDA 2004/2005 Exploratory Data.” U.S. Food and Drug Administration: Center for Food Safety and Applied Nutrition: Office of Plant & Dairy Foods. May 2007. http://www.cfsan.fda.gov/~dms/clo4ee.html. 8. Blount, Benjamin C et al. "Perchlorate Exposure of the US Population, 2001–2002." Journal of Exposure Science and Environmental Epidemiology (2007) published online 18 October 2006. http://www.nature.com/jes/journal/v17/n4/abs/7500535a.htm. 9. Waldman, Peter. “Perchlorate Runoff Flows to Water Supply of Millions: A Fuel of Cold War Defenses Now Ignites Health Controversy.” Wall Street Journal. 16 Dec. 2002. http://www.mindfully.org/Pesticide/2002/Perchlorate-Water-Cold-War16dec02.htm. 10. Jarabek, Annie M. Disposition of Comments and Recommendations for Revisions to ‘Perchlorate Enviromental Contamination: Toxicological Review and Risk Characterization External Review Draft (January 16, 2002)’. United States Environmental Protection Agency. http://physics.harvard.edu/~wilson/FRESHMAN%20SEMINAR/Perchlorate/EPA%20Perchlorate%20Respo nse%20to%20NAS%2010-27-2003.pdf. 11. Madsen, Travis and Sujatha Jahagirdar. The Politics of Rocket Fuel Pollution: The Perchlorate Study Group and its Industry Backers. California, Environment California Research & Policy Center, 2006. 12. Lee, Jennifer. "Second Thoughts on a Chemical: In Water, How Much is Too Much?" New York Times. 2 March 2004. http://query.nytimes.com/gst/fullpage.html?res=9C05E7DE173FF931A35750C0A9629C8B63&scp=1&sq=c olorado%20river%20perchlorate&st=cse 13. Wilson, Michael. "Office of Inspector General Scientific Analysis of Perchlorate." Environmental Protection Agency Office of the Inspector General. Washington DC: Environmental Protection Agency, 2008. http://www.epa.gov/oig/reports/2009/20081230-2008-0010.pdf 14. Greer, Monte A., et al. "Health Effects Assessment for Environmental Percholate Contamination: The Dose Response for Inhibition of Thyroidal Radioiodine Uptake in Humans." Environmental Health Perspectives 110.9 (Sep. 2002): 927. Academic Search Premier. EBSCO. Harvard Library System, Cambridge, MA. 27 Jan. 2009 <http://ezpprod1.hul.harvard.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=aph&AN=7555751 &site=ehost-live&scope=site>. 15. Shomon, Mary. "Thyroid Organizations Take On Generic Levothyroxine: Should You Be Concerned About Taking Generic Thyroid Drugs?" About.com. 4 Oct. 2006. http://thyroid.about.com/od/thyroiddrugstreatments/a/oct2006.htm. 16. Norman, James. "Hypothyroidism: Too little thyroid Hormone: Diagnosis and Treatment of Hypothyroidism." endocrineweb.com. http://www.endocrineweb.com/hypo2.html.