Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Marburg virus disease wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Chagas disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Leishmaniasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Onchocerciasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
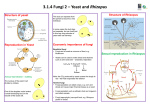
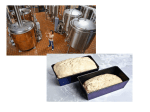
LAB 21 OBSERVATION OF FUNGI FUNGI DISEASES OBSERVATION OF PREPARED SLIDES (use photos from chapter 11.1 to help you identify the structures you see and the names of the fungi). Look at the fruiting bodies, and know the life cycles of the following phylums: 1. Ascomycota (observe under 400x, not oil!) a. Penicillium: conidia and conidiospores (amorph/asexual) b. Aspergillus: conidia and conidiospores (amorph/asexual) c. Peziza: asci, ascospores (teleomorph/sexual) d. Saccharomyces (beer yeast): parent cells and buds; use 1000x for this one. 2. Zygomycota a. Rhizopus: anamorph and teleomorph: sporangia, sporangiospores, zygospores 3. Basidiomycota: teleomorph; observe the mushroom coprinus Draw each of these slides on data sheet 11.1; on the last page are some blank circles where you can draw coprinus and peziza. OBSERVATION OF LIVE CULTURES Place one drop of lactophenol cotton blue on a clean slide. The phenol in this dye penetrates the chitinous cell wall of the fungi to stain the fruiting body; it will also penetrate your skin, and it is toxic! Use gloves and goggles. Sterilize a probe needle and stick it into your agar block to hold it down. Use sterile forceps to lift the cover slip off. Take the cover slip, MOLD FACING DOWN, and touch the side of the slide to the dye for a few seconds, and then let it fall down onto the slide. Wick off the excess dye and throw the paper towel into the biohazard bag. Observe under 400x (NOT OIL), and draw your pictures. Discard entire slide and coverslip into the broken glass box. Do not clean and reuse these slides. CLINICALLY SIGNIFICANT DISEASES: OPPORTUNISTIC MYCOSES 1. Aspergillosis: can occur anywhere in the body, but is most common in the lungs. Some people just have allergies to this mold. X-ray of aspergillosis shows aspergilloma (“fungus balls”) which are mycelium and white blood cells. Although opportunistic diseases are usually seen in immunocompromised people, healthy people who are overexposed can also get sick. Since this mold loves grains, farmers are especially at risk. Some species make a mycotoxin called aflatoxin, which is a potent liver carcinogen. 2. Ringworm: these skin lesions are circular, so they look like a worm. It is caused by a group of fungi called dermatophytes, which live on keratin (found in skin, hair, and nails). Dermatophyte infections are the most common fungal infections in humans. They are known as “tinnea”. Fungi like moisture, and feet are in a dark, moist environment, so infection is common there. Athlete’s foot is known as tinnea pedis. You get it by just walking barefoot, exposing the skin to the air where spores are. If there is a slight scratch in the skin, the fungi can get in. They form itchy vesicles. When scratched, the fungus spreads. Treatment is topical creams. When dermatophytes infect the nails it is called onychomycosis. The nails get thick, chalky, discolored. Topical creams don’t penetrate the nails. Oral medicines like griseofulvin kill the fungus but are also toxic to the liver. Onychomycosis is common with age. Ringworm can also occur in the scalp, usually in children. The hyphae are fluorescent, so you can use a Wood’s Lamp, which shines with ultraviolet light, and see the hyphae glow. When dermatophytes cause a skin rash, they can be diagnosed by scraping a bit of the skin onto a slide, and adding KOH, which dissolves the skin cells and leaves the hyphae. The hyphae, when observed under the microscope, are diagnostic for dermatophytes. 3. 4. 5. 6. Candidiasis Cryptococcosis Histoplasmosis San Joaquin Valley Fever Rhizopus (sexual) FUNGI DISEASES Be able to draw and label the following fruiting bodies for the quiz this Thursday: Rhizopus (asexual; haploid): sporangiophore, columella, sporangium, sporangiospores, rhizoids, and stolon. Rhizopus (sexual; diploid): gametangia, suspensors, zygospore Aspergillus (asexual): conidiophore, vesicle, philiae, conidospores (or conidia), foot cell. Penicillium (asexual): conidiophore, metula, philae, conidiospores (or conidia) Peziza (sexual; haploid): ascus, ascospores Coprinus (sexual; haploid): gill, basidium, basidiospores Here is the taxonomic classification: PHYLUM Ascomycota Ascomycota Zygomycota Basidiomycota CLASS Ascomycetes Ascomycetes Zygomycetes Basidiomycetes GENUS Penicillium Aspergillus Rhizopus Coprinus MYCOTOXINS Basidiomycota makes mushrooms which are either edible or deadly. The species agaricus is the edible “Button mushroom” in stores. The species amanita is deadly and produces a mycotoxin called phaloidin (damages liver). The species psilocibe (called “magic mushrooms”) produces a mycotoxin called psilocybin, which is a hallucinogen like LSD. Aspergillus makes a mycotoxin called aflatoxin (grains, jelly, peanut butter); damages liver. CONTINUATION OF DISEASES FROM HANDOUT: CHAPTER 12 NOTE: Opportunistic pathogens: Aspergillus, ringworm, Cryptococcus, Candida, Pneumocystic pneumonii. NOTE: The term “yeast” is referring to just the morphology (single cell fungus, reproduces by asexual budding, may or may not have sexual cycle); “yeast” is not the taxonomy. NOTE: There are two major branches of the immune system. Humeral immunity is the type of white blood cell that can make proteins (antibodies) which kill the invading organism. Cell-mediated immunity (CMI) does not make antibiotics; the white blood cells kill the invading organism directly. If the CMI cells (T-cells) are not working (AIDS patients), opportunistic pathogens can take over and cause disease. Cryptococcus neoformans Lives in soil rich in nitrogen, especially bird droppings. Common in urban areas (cities) because of the pigeons. Not as common in rural (country) areas. People do not get sick unless their immune system is not healthy. The disease starts out as a primary pulmonary infection with flulike symptoms of cough, congestion, fever. Most people recover easily. In the immunocompromised, the disease progresses to Cryptococcosis, where it starts as pneumonia and disseminates (spreads) to the blood and then to the CNS (central nervous system). It causes neurological damage in those who survive. The Blood-Brain Barrier (BBB) does not allow compound of large molecular weight to cross into the brain, so most drugs cannot treat CNS infections. Treatment is either Amphoteracin B (injected or IV), which is potent, but side effects include kidney damage, or Fluconazole (or other “azole” medicines) which is oral (pill form). This disease can cause meningitis (headache, fever, stiff neck), but so do many other diseases, including bacteria and viruses. The meds for each disease are different, so it is important to make the correct differential diagnosis (DDx: to differentiate this organism from others). The azole medicines affect the sterols in the plasma membrane, so they work on fungi, but most bacteria do not have sterols. A sample of CSF (cerebrospinal fluid) is taken from the patient and cultured and stained with India ink. Seeing a budding yeast with a huge capsule around it is diagnostic. The capsules serve to resist phagocytosis (being eaten) by white blood cells. Candida albicans This is an endogenous flora (naturally found on our bodies). Endogenous flora compete with each other and should remain balanced. If one organism dies off (such as after antibacterial medicines) one other organism (like Candida) can take over and cause disease. Candida albicans is normally found in the mouth and vagina. The oral form of this disease is called thrush. It can occur in newborns after passing through a birth canal, and babies don’t have a fully formed immune system until after they are a year old. Thrush can also occur in diabetics, elderly, and AID patients. When it occurs in the esophagus, it makes it hard to swallow. When the disease is in the vagina, it is called vulvovaginitis (affects 5% of women right now). It can also occur in wet areas of the skin and is common among dishwashers. This form is called Cutaneous Candidiasis, and can be mistaken for a bacterial “jock itch” or diaper rash. Although it looks like a dermatophyte infection, those creams won’t work here. Candida albicans can be grown on cornmeal agar, where it makes pseudohyphae (elongated buds) which is the DDx. There is also a Germ Tube Test: incubate the yeast with plasma serum for one hour and the cell sends out long tube-like pseudohyphae called germ tubes. Chlamidiospores are also seen and are only on Candida. There are also test kits (like the one for the API) that diagnose Candida by the sugars it ferments. There are five opportunistic yeasts that we have covered: Candida albicans Cryptococcus neoformins Pneumocystic corynei Histoplasma capsulatum Blastomyces dermatitidis The last two on the above list are the only true pathogens (cause disease in healthy people) because they are thermodimorphic. The yeast form is only in the tissue phase. The environmental phase (in the soil) is not a yeast; it is a mold with conidia. The patients are not contagious because the tissue phase is not communicable. The environmental phase is the infectious stage. Histoplasma capsulatum This organism is found in soil that is rich in nitrogen, especially caves with bat droppings (guano). Such caves are moist, rich in nitrogen, and have dead organic material there, which are ideal conditions for molds. Spelunkers are people who explore caves, usually on their hands and knees. Their nose is close to the floor, so they inhale the conidia spores. Hunting dogs get it the same way. When you hear the word “cave”, think of Histoplasma. Histoplasmosis is endemic in certain areas, such as the Mississippi and Ohio River valleys which carve into organic matter in the ground. They are located in the Midwest, south, and eastern areas of the country, where the climate is moist. The tissue phase is a budding yeast. The disease starts with flu-like symptoms and a cough. X-rays show lesions that are similar to TB, but the medicines are different, so the DDx is important. There is a skin test for histoplaasmosis, similar to the one for TB. You can also do a KOH wet mount on a skin lesion; a budding yeast is diagnostic. The disease is chronic, and relapsing over many years. It can disseminate into the skin, GI, and renal systems. HIV patients are particularly at risk. Treatment is Amphoteracin B or Fluconazole. These just treat the disease, but it won’t cure it. Coccidiodes immunis This is known as San Joaquin Valley Fever. It grows in the soil in its mold form. Under the microscope, you can see arthrospores (finger-like phalange-shaped). These break off and are carried by the wind where people inhale them. The people are not contagious because the infectious stage in the environmental phase. This organism differs from histoplasmosis and Blastomyces in that it requires long periods of dry (arid) weather, and then a heavy rain. That makes it endemic to west Texas, Mexico, Baha, South America, southern California, Arizona, and New Mexico. The blood of everyone who lives in the San Joaquin Valley tests positive for the organism, but they don’t usually get the disease. That’s because you need to be exposed to a large amount to get sick; therefore farmers are at risk. Caesar Chavez fought for the rights of immigrant farm workers, who were given short tools to weed the farms, so their noses were close to the ground to inhale the spores. They also were not paid well and had poor nutrition, so they would get the disease. Once the spores get into the lungs, thermodimprphism occurs, and the sporangia form a spherule (not a yeast bud). The primary pulmonary infection is flu-like symptoms, and then it can disseminate into the bones, skin, and CNS. It is a recurring disease with treatment but no cure. Treatment is Amphoteracin B or Fluconazole. Note that there are only a few drugs for the mycoses, while there are many antibacterial medicines.