Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
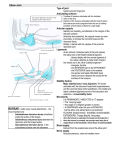
1 Description The olecranon is a bony prominence of the ulna that represents that bone’s most proximal posterior surface at the elbow. While the medial border of the olecranon is a part of the flexor carpi ulnaris origin and the lateral border is an attachment point for the anconeus muscle, the major muscle attachment is that of the triceps. The olecranon can thus be fractured (avulsed) by a traction force from triceps contracture. The subcutaneous position of the olecranon renders it susceptible to direct trauma as well. Displaced fractures of the olecranon often disrupt the articular surface of the elbow joint; these have to be realigned with surgery. Further, because the triceps can displace fractures that were originally not displaced, and because the elbow is relatively intolerant of prolonged immobilization, surgical treatment rather than casting is often needed even for fractures with minimal displacement. Figures: radiograph of displaced fracture 2 Structure and function The olecranon is a strong process of the proximal and posterior ulna that, together with the coronoid process, forms the trochlear notch. This notch holds the trochlea of the distal humerus forming the ulnohumeral articulation, the hinge joint of the elbow. The trochlear notch is covered with articular cartilage, therefore most olecranon fractures (except the ones occurring exclusively on the tip) are, by definition, intra-articular fractures. Successful treatment of olecranon fractures requires not only reestablishment of the extensor mechanism (which would be disrupted if/when a fracture displaces) but preservation of elbow stability. The main side-to-side (valgus and varus) stabilizers of the elbow are the collateral ligaments and the ulnohumeral/radiohumeral articulation, which provide a buttress against compressive forces laterally. The olecranon is an important stabilizer too: it blocks anterior translation of the ulna with respect to the distal humerus just as the coronoid process of the ulna resists posterior subluxation of the ulna. The triceps muscle inserts into the proximal ulna and posterior third of the olecranon. Its fibers blend with the periostium of the olecranon, the lateral ligaments and the articular capsule, forming a strong fibrous covering. This fibrous covering prevents fractures from being dramatically displaced unless the force is so great that the soft tissues rupture along with fracture of the bone. The lateral border of the olecranon is an attachment point for the anconeus muscle. The ulnar nerve runs on the posterior aspect of the elbow, behind the medial epicondyle of the humerus; it then turns anterior joining the ulnar artery. Its proximity to the olecranon makes it vulnerable to injury when fractures occur. The medial border of the olecranon is a part of the flexor carpi ulnaris origin. 3 Patient presentation Patients with fractures of the olecranon present with elbow pain after direct elbow trauma or a fall. The clinical examination can detect varus/valgus instability, but the primary determination is whether the extensor mechanism is intact. The mechanism of injury often determines the fracture pattern. If there is a fall on a semi-flexed arm, when the hand strikes the ground, the triceps muscle forcefully contracts, resisting further flexion of the elbow. This “breaking the fall” reaction leads to breaking the bone: an avulsion fracture of the tip of the olecranon, pulled off by the triceps. This mechanism is more commonly seen in elderly patients. Less frequently, the cause is direct trauma to the tip of the elbow, which usually leads to comminuted fractures. This is mostly the mechanism in younger patients. In elderly patients, the bone fracture is often an isolated finding. The diagnostic attention is paid to determine why the patient fell. In younger patients, the mechanism of injury is often of higher energy and diagnostic attention is paid to make sure that there are no associated injuries elsewhere. Other less common mechanisms are hyperextension injuries, such as those resulting in elbow dislocation in adults or supracondylar fractures in children. These can fracture the olecranon when it is impacted against the olecranon fossa of the distal humerus. Stress fractures due to muscle forces such as throwing are a rare cause of olecranon fractures in adults, however in young pitchers it is relatively common. Because most fractures of the olecranon involve the joint surface, there is generally hemorrhage into the joint with a resultant effusion. This produces pain and swelling. Skin openings are somewhat common given the subcutaneous location of the ulna. Ulnar nerve neurapraxia may develop in 2-5% of cases. 4 Clinical evidence A standard lateral radiograph of the elbow is sufficient for evaluation of isolated olecranon fractures. A true lateral X-ray is of paramount importance because it helps to determine the extent of the fracture, degree of displacement, comminution, radial head subluxation, and the degree of articular surface involvement. A non-displaced, transverse, or slightly oblique intra-articular break near the base of the olecranon is the most commonly seen olecranon fracture. Figures: radiograph of nondisplaced fracture If there is absence of radiographical evidence of a fracture, an important sign to look for on the lateral X-ray is the fat pad sign. This is a sign of intra-articular effusion; distension of the joint capsule elevates the fat pads on top of it, suggesting an intra-articular fracture. Figures: radiograph of fat pad (same as radial head) It is important to assess for fracture displacement potential on radiographs. That is, most olecranon fractures exhibit little or no displacement, but some may displace with elbow motion. Thus, a fracture is considered non-displaced only when the fracture gap is less than 2mm even when the elbow is flexed at 90°. Joint stability can also be inferred from radiographs. If the fracture involves more than 50% of the ulnohumeral articulation, the elbow can be assumed to be unstable. Associated lesions such as coronoid fractures, radial head fractures or torn collateral ligaments may also produce instability. 5 Epidemiology Olecranon fractures account for 10% of elbow fractures in adults. In children, by contrast, with excessive forces on the elbow, the distal humerus is more likely to be broken. This is because the olecranon is comparatively shorter and thick before skeletal maturity. This point is noteworthy because the presence of an olecranon fracture in a child suggests a primary bone disease such as osteogenesis imperfecta. 6 Differential diagnosis Anterior elbow dislocations often occur with associated olecranon fractures, especially when a posterior direct blow is suffered. Lateral radiographs confirm this association. Similarly, Monteggia fractures (ie a fracture of the proximal third of the ulna with dislocation of the head of the radius) can be produced by the same mechanism as an olecranon fracture; this would be detected with adequate radiographs. Supracondylar fractures of the humerus should also be considered, especially in children who fall on semiflexed arms and/or suffer direct blows on the elbow. Radial head fractures and fractures of the coronoid process may produce elbow instability and complicate olecranon fractures. An abnormality in the relationship between the osseous landmarks (i.e. line and triangle formed by epicondyles and olecranon) may be used to distinguish between intra-articular fractures, dislocations and supracondylar fractures. 7 Red Flags Comminution of an olecranon fracture suggests higher energy and implies other associated injuries (which must be diligently excluded) Blood on the skin may signify an open fracture, perhaps sustained by the bone poking out when the fracture is maximally displaced, then retracting back into the skin when the bone straightens out somewhat. Inadequate imaging. Even if the presentation is classic for an isolated elbow injury, films of the wrist are required. 8 Treatment options and outcomes The treatment goals are to maintain a stable and anatomic reduction, achieve stability of the joint, and enable early active motion . Fractures with up to 2mm of displacement with intact extensor mechanisms may be treated with three to four weeks of casting in a long arm cast. The elbow can be placed between 45° and 90° of flexion. After one month, supervised passive motion is started until radiographic evidence of union is achieved, then active movement is encouraged. Fractures with significant displacement (>2mm) or comminution may require surgical intervention because of compromise of the extensor power. Approximately 70% of the extensor power is estimated to be lost when the fracture is displaced more than 1.5 cm. FIGURES: EYE CANDY SHOWING Rx FIGURE Tension band wiring: A tension band wire is the most common fixation technique for simple displaced fractures without comminution, especially avulsion type fractures. It uses Kirchner wires and tension wires and works by compressing the fracture surfaces together. FIGURE Intramedullary screw fixation: Intramedullary screw fixation is the most secure technique. Biomechanically, screw fixation does not provide as secure a fixation as tension-band wiring. However, by adding a tension band, excellent fixation can be obtained. FIGURE Plate fixation: Plate fixation is recommended for extensive comminuted or unstable oblique fractures and also when associated injuries are present (e.g. coronoid fractures). Excision of the fracture fragment and reattachment of the triceps tendon may be indicated in elderly patients with osteoporotic bone and in low-demand patients, especially when the fragment is too small or comminuted for successful internal fixation. Olecranon fractures heal well in most instances and recovery of normal function is achieved in more than 95% of patients. Functional outcome is dependent on fracture severity, length of immobilization, and patient factors. The best outcomes are observed in patients who have minimally displaced fractures treated non-operatively. In patients treated operatively, symptomatic hardware requiring removal is the most frequent complication. Injury to the ulnar artery, the median or anterior interosseus nerves (AIN) is possible with penetration of the K-wires through the anterior cortex of the ulna. Infection following operative treatment happens rarely. Heterotopic ossification occurs in 10-15% of patients. Loss of motion is rarely significant (less than 15° of extension) and nonunion occurs in about 1% of patients and is treated by internal fixation and bone grafting . 9 Risk factors and prevention Risk factors include any underlying medical pathology that could cause a fall (e.g. syncope), especially in older patients. Also, any pathology that could weaken the bone like osteogenesis imperfecta in children or those that cause osteopenia such as osteoporosis, steroid use, or vitamin D deficiency. Type of physical activity becomes a risk factor only in young pitchers who are prone to stress fractures. Elbow pads for high contact sports and activities may be used to protect from direct blows that could cause fractures. 10 Miscellany In mixed martial arts competitions, an elbow drop (a move in which a fighter drives his elbow into the opponent's body) takes advantage of the strength of the olecranon. It is forbidden primarily because of the risk to the recipient of the blow, though of course the striker may sustain a fracture too. Olecranon is a word of Greek origin whose second root is “kranion”, meaning head. (The word “cranium” has the same root.) Still, the olecranon should not be thought of as the “ulnar head” as the first root is “olene”, meaning “elbow”. 11 Key terms olecranon; ulna; ulnar nerve neurapraxia; triceps advancement; tension band wiring; bipartite olecranon; patella cubiti. 12 Skills Recognize on examination failure of the extensor mechanism, fracture displacement and joint instability; correctly interpret radiographs and describe fracture pattern; identify fractures that would require operative treatment; apply elbow immobilization until definitive treatment is obtained.