Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
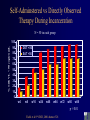
Initiation of Antiretroviral Therapy (ART) Christopher Behrens, MD Northwest AIDS Education & Training Center University of Washington When Should Patients with HIV be Treated with ART? • Benefits – reduced morbidity & mortality – immune system recovery • Drawbacks – toxicities – lifestyle changes – potential for developing resistance Initiation of Antiretroviral Therapy: Key Considerations • Symptoms & Opportunistic Infections • CD4 count • Viral Load • Anticipated Adherence - patient ‘readiness’ Initiation of ART: Case A 29-year old woman comes to the clinic for routine HIV care; she has been HIV-infected for about 4 years, and has never received antiretroviral treatment. Her most recent CD4 count is 330 cells/mm³ and her viral load is 88,000 copies/mL. Would you suggest she start antiretroviral therapy? What does a CD4 count of 330 cells/mm³ mean? HIV Infection is characterized by a steady decline in the number of CD4 cells CD4 Cell Count (cells/mm³) Acute Infection Asymptomatic HIV Infection AIDS 1,000 CD4 cell count 500 200 high risk of opportunistic infections 4-8 Weeks Up to 12 Years Time 2-3 Years mm³ (cells/mm³) Mellors et al. Ann Intern Med 1997;126:946. When Should ART be Initiated? An analysis of prospective studies • 13 cohort studies from Europe & North America • 12,574 patients initiating ART – – – – – Median age 38; mostly men Median baseline CD4 count 250; VL 74,000 Median month of ART initiation: 12/1997 Mostly PI-based regimens 24,310 person-years of followup Egger et al. Lancet 2002; 360:119-30. Analysis of 13 cohort studies: effect of baseline CD4 count on response to initial ART Years from starting HAART Egger et al. Lancet 2002; 360:119-30. Findings: effects of clinical stage on clinical progression Years after starting HAART Egger et al. Lancet 2002; 360:119-30. Findings: effect of baseline HIV Viral Load on response to ART Years from starting HAART Egger et al. Lancet 2002; 360:119-30. Cohort studies: conclusions • Initiation of ART after HIV-related symptoms had developed was associated with a less durable response to ART • For the asymptomatic patient, CD4 count at initiation of ART carried strongest prognostic significance, corroborating findings from other studies1-4 • Age, infection via IDU, history of AIDS-related illness also appeared to affect durability of clinical response to ART 1. Chen RY et al. 8th CROI, Chicago 2001 2. Hogg RS et al. JAMA. 2001;286:2568-2577 3. Sterling et al, 9th CROI, Seattle 2002 4. Palella et al, 9th CROI, Seattle 2002 Caveats • High VL (>100,000 copies/mL) also carried prognostic significance, but – few patients initiated on efavirenz or ritonavir-boosted regimens – other recent studies have not demonstrated a clear correlation between baseline viral load and efficacy of ART1,2 • Observational study: other potential confounding factors (e.g., adherence, hemoglobin) could have affected results 1. Philips AN et al. JAMA 2001;286:2560-2567. 2. Hogg RS et al. JAMA 2001;286:2568-2577. Implications for Clinical Practice • Ideally, initiate ART before CD4 count drops below 200 cells/mm³ and before clinical symptoms develop • A benefit for treatment before CD4 count falls below 350 may exist, but the small risk of clinical progression if therapy is deferred must be balanced against drawbacks of ART • If CD4 already less than 200 or clinical progression has occurred, ART is clearly indicated as soon as patient is ready to start Implications for Clinical Practice: Significance of Baseline Viral Load • Initiation of ART before VL >100,000 copies/mL may allow for more therapeutic options and greater clinical success • However, highly potent efavirenz- or boosted PIbased regimens may be equally effective in patients with high baseline viral loads1-3 • VL is a marker for rate of CD4 decline: more frequent monitoring in patients with high VL? 1. XIV International AIDS Conference, July 2002. Abstract TuOrB1189 2. Arribas JR et al. AIDS 2002;16(11):1554-6. 3. Walmsley S et al. NEJM 2002 346(26):2039-46. CD4 Count, Viral Load, and Clinical Course Primary Infection Seroconversion 10,000,000 AIDS Plasma HIV RNA 1,000,000 100,000 10,000 Plasma RNA Copies 1,000 CD4 Cell Count Intermediate Stage 1,000 CD4 Cells 100 500 10 1 4-8 Weeks Up to 12 Years 2-3 Years When Should ART be Initiated? DHHS Guidelines Clinical Category CD4 count Viral Load Recommendation Symptomatic (AIDS, severe Sx) Any value Any value Treat Asymptomatic, AIDS < 200/mm3 Any value Treat Asymptomatic > 200/mm3 Any value but < 350 Asymptomatic > 350/mm3 > 100,000 copies/mL Asymptomatic > 350/mm3 < 100,000 copies/mL Treatment should be offered following full discussion of pros and cons with each patient Most clinicians recommend deferring therapy, but some would treat Defer therapy DHHS Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents, October 6, 2005. When Should ART be Initiated? IASUSA Guidelines Yeni et al. JAMA. 2004;292:251-265. Recent Advances in Antiretroviral Therapy incremental gains in convenience, tolerability, and insights into toxicity have added up to significant improvements in management of HIV disease Advances in Antiretroviral Therapy: Easier Regimens • Lower pill burden • Once-daily dosing – Fixed dose combinations • • • • TDF/FTC (Truvada) ABC/3TC (Epzicom) AZT/3TC (Combivir) AZT3TC/ABC (Trizivir) – Fewer pills for same effect • • • • • efavirenz nelfinavir fosamprenavir lopinavir/ritonavir saquinavir • • • • • • • • • tenofovir 3TC, FTC abacavir ddI efavirenz atazanavir fosamprenavir (w/ ritonavir) saquinavir (w/ ritonavir) lopinavir/ritonavir • Fewer food restrictions with newer agents and with ritonavir boosting of protease inhibitors Advances in Antiretroviral Therapy: Improvements in Toxicity • New drugs with less toxicity – Tenofovir: no dyslipidemia compared with d4T – Atazanavir: no dyslipidemia compared with other PIs • Improved Understanding of Toxicities – Nevirapine toxicity: identification of high-risk groups • women CD4 >250 cells/mm³ • men CD4 >400 cells/mm³ – Mitochondrial toxicity as basis for many long-term toxicities – Clarification of which NRTIs are most likely to cause mitochondrial toxicity (d4T, ddI, ddC) – Partial clarification of lipodystrophy Timing of Initiation of ART Is the Pendulum Swinging Back to Earlier Treatment? Before you start… Resistance Testing Adherence Issues Resistance in treatment-naïve individuals is becoming more common Recently Infected, ART Naïve, United States Little SJ, Holte S, Routy JP, et al. N Engl J Med. 2002;347:385-94 Persistence of Resistant Strains Following Primary HIV Infection • 11 subjects with primary HIV infection who deferred ART and who had at least one major drug resistance mutation identified at presentation, followed with serial resistance assays. – – – – 7 subjects with NNRTI resistance 2 with NRTI and PI resistance 1 with NNRTI and PI resistance 1 with resistance to all three classes of drugs • NNRTI resistance was lost slowly: the average time to reversion of 103N variants to mixed 103N/K populations was 196 days following the estimated date of infection (153 to 238 days, 95%CI). • PI resistance was not lost at all: In the 4 patients with protease resistance mutations, no reversion was detected at 64, 191, 327, and 342 days after infection. • Complete reversion of genotypic resistance was observed in only one patient, at 1019 days after infection. Little SJ. 11th CROI, February 2004, Abstract 36LB Antiretroviral Resistance Testing: Guidelines for Implementation Clinical Setting/ Recommendation Rationale Recommended: •Virologic failure during ART Determine role of resistance in drug failure and maximize the number of active drugs in the new regimen •Suboptimal suppression of viral load Determine the role of resistance in drug failure and maximize the number of active drugs in the new regimen (VL) after initiation of ART Determine if resistant virus was transmitted; select •Acute (primary) HIV infection regimen accordingly •Chronic HIV infection before Assays may not detect minor resistant species, but some starting ART resistance mutations may persist for years. Consider testing early after diagnosis of HIV infection. Usually not recommended: •After discontinuation of drugs •Plasma VL <1,000 copies/mL Resistance mutations may become minor species in the absence of selective drug pressure Resistance assays unreliable if VL is low Adapted from DHHS, Antiretroviral Guidelines, October 6, 2005 Initiation of Antiretroviral Therapy: Key Considerations • Symptoms & Opportunistic Infections • CD4 count • Viral Load • Anticipated Adherence - patient ‘readiness’ Adherence: Case 1 • A 23 year old single woman with HIV infection diagnosed two years ago. • No history of antiretroviral therapy. • Current CD4 count is 230 cells/mm³. • Her physical exam is remarkable only for oral candidiasis (thrush). • Review of her past medical history includes depression, which she admits has been worse lately. • Current medications include nortriptyline and oral contraceptives. Adherence • Which of the following factors in her situation suggests that adherence may be problematic for her? A. B. C. D. her depression she is already symptomatic with HIV infection her age (less than 30 years old) all of the above factors are associated with reduced adherence to antiretrovirals. Adherence • Which of the following factors in her situation suggests that adherence may be problematic for her? A. B. C. D. her depression she is already symptomatic with HIV infection her age (less than 30 years old) all of the above factors are associated with reduced adherence to antiretrovirals. Adherence “Drugs don’t work if people don’t take them.” - C. Everett Koop Virologic Control falls sharply with diminished adherence Patients with HIV RNA <400 copies/mL, % 100 80 60 40 20 0 >95 90-95 80–90 70-80 <70 PI adherence, % (electronic bottle caps) Paterson, et al. 6th Conference on Retroviruses and Opportunistic Infections; 1999; Chicago, IL. Abstract 92. Self-Adminstered vs Directly Observed Therapy During Incarceration % with VL < 50 copies/mL N = 50 in each group 100 90 80 70 60 50 40 30 20 10 0 DOT <50 SAT <50 w4 w8 w16 w24 w48 w64 w72 w80 w88 p < 0.01 Fischl et al 8th CROI, 2001 abstract 528 Predictors of Poor Adherence • • • • • • • active alcohol1 or substance2 abuse work outside the home for pay1 depressed mood1 lack of perceived efficacy of ART3 lack of advanced disease4 concern over side effects4 regimen complexity5 1. Chesney MA. 37th ICAAC, 1997; Toronto. Abstract 281. 2. Cheever LW, Curr Infect Dis Rep 1999 Oct;1(4):401-407. 3. Horne R, et al. 39th ICAAC, 1999; San Francisco. Abstract 588. 4. Wenger N, et al. 6th CROI, 1999, Abstract 98. 5. Stone VE, et al. JAIDS 2001; 28:124-131 Factors Associated with Higher Levels of Adherence • • • • • twice-daily or once-daily regimens1,4 belief in own ability to adhere to regimen1 not living alone2 dependent on a significant other for support2 history of opportunistic infection or advanced HIV disease3 1. Eldred L, et al, J Acquir Immune Defic Syndr Hum Retrovirol 1998;18:117-125. 2. Morse EV et al, Soc Sci Med 1991;32:1161-1167. 3. Singh N, et al, AIDS Care 1996;8:261-269. Factors Associated with Higher Levels of Adherence • Belief in efficacy of antiretroviral therapy • Belief that non-adherence will lead to viral resistance Wenger N, et al. 6th Conference on Retroviruses and Opportunistic Infections, 1999; Chicago. Abstract 98. How good are clinicians at predicting their patients’ adherence? A. B. C. D. 95% 85% 75% Not much better than flipping a coin Clinicians’ Estimates of Adherence Not Much Better Than Random Bangsberg Paterson Haubrich Steiner Bosely Charney Caron Gilbert Blowey Mushlin 2001 2000 1999 1995 1995 1967 1978 1980 1997 1977 JAIDS Annals Int Med AIDS Arch Int Med Eur Resp J Pediatrics Clin Pharmacol Can Med Assoc J Ped Nephrology Arch Int Med ART ART ART AZT Inhaled terbutaline Penicillin Antacids Digoxin Cyclosporin Hypertensive Improving Adherence: Before Initiation of Therapy Assess patient's understanding and acceptance of the regimen: negotiated plan Investigate and manage medical barriers to adherence • Try to use simple regimens – Twice-daily or better – Without food requirements if possible Adapted from: Miller et al., The AIDS Reader 10(3):177-185, 2000. Improving Adherence: After Initiation of Therapy • Close follow-up • Ask patient to verbalize treatment regimen • Education about adherence • Consider cues, alarms to remind patients of dosing • Referral to community support groups • Involve other members of the health care team Back to Case 1 • You confirm her viral load and CD4 count; she keeps her follow-up appointments and appears to understand the importance of adherence. You start her on an antidepressant medication and refer her for counseling. 3 months later her depression is significantly improved and she feels ready to initiate ART. • What regimen would you recommend? Selecting the Initial ART Regimen Combination Antiretroviral Therapy (ART) • Combination of at least 3 drugs, usually: – 2 NRTIs (the “NRTI backbone”), plus: – 1 NNRTI or 1-2 PIs • Therapy with only one or two agents allows HIV to overcome therapy through resistance mutations HIV Life Cycle and Classes of ARVs HIV Nucleoside Analogues (NRTIs) Reverse Transcriptase RNA DNA Nucleus Fusion Inhibitors Host Cell Non-Nucleosides (NNRTIs) Protease Inhibitors (PIs) FDA-Approved ARVS: NRTIs FDA-Approved ARVS: NNRTIs and PIs FDA-Approved ARVS: PIs (cont.) and Fusion Inhibitor Ritonavir intensification of other Protease Inhibitors (PIs) • PIs, like many medications, are metabolized in the liver by the cytochrome P450 enzyme complex • Ritonavir inhibits this complex, thereby boosting serum levels of co-administered PIs • Low doses of ritonavir can be used to increase the potency and simplify the dosing of PI-based regimens An Example of Ritonavir Boosting: Indinavir/Ritonavir BID PK Study 10,000 IDV/RTV q12h: 800/200 High-fat Meal Indinavir Plasma Concentration (nM) 800/100 High-fat Meal 1,000 400/400 High-fat Meal IDV q8h: 800 mg Fasted 100 0 2 4 6 8 Time after dose (hours) 10 12 6th Conference on Retroviruses and Opportunistic Infections; 1999. Abstract 362. Preferred Initial ART Regimens: DHHS Guidelines • NNRTI-based: Efavirenz* + 3TC or FTC + AZT or tenofovir * except during first trimester of pregnancy or women with high pregnancy potential • PI-based: Lopinavir/ritonavir (Kaletra) + 3TC or FTC + AZT DHHS Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents, October 6, 2005. Atazanavir: favorable dosing and toxicity profile • 2 pills once daily • Not associated with dyslipidemia1 and hyperglycemia2, unlike other PIs • Case reports of reversal of lipodystrophy when PI switched to ATV 1. Piliero P et al. 9th CROI, Seattle, February 2002. Abstract 706-T. 2. Sension M et al, 4th Intl Lipodystrophy Workshop, San Diego, 2002. Abstract 36. AI424-034: Atazanavir vs Efavirenz 100 90 % Responders • N=810 treatmentnaïve patients randomized to AZT/3TC plus either efavirenz or atazanavir • Mean baseline viral load 4.85 log copies/mL • Mean baseline CD4 count 320 cells/mm³ 80 Efavirenz Atazanavir 70 Line 4 VL <400 copies/mL 60 50 p = NS 40 30 VL <50 copies/mL 20 10 0 4 8 12 16 24 32 Week Squires KE et al. 42nd ICAAC, September 2002. Abstract 1076. 40 48 Initial ART: Practice • NNRTI-based: efavirenz + 3TC or FTC + AZT or tenofovir * except during first trimester of pregnancy or women with high pregnancy potential • PI-based: lopinavir/ritonavir (Kaletra) or atazanavir/ritonavir + 3TC or FTC + AZT or tenofovir Initial ART: Practice Anchor Drug NRTI backbone Dosing Daily pill burden Efavirenz AZT + 3TC bid 3 TDF + FTC qd 2 AZT + 3TC bid 6 TDF + FTC bid 5 AZT + 3TC bid 5 TDF + FTC qd 4 Lopinavir/ ritonavir Atazanavir/ ritonavir Initial HAART: Future? Anchor Drug Efavirenz Lopinavir/ ritonavir Atazanavir/ ritonavir NRTI backbone Dosing Daily pill burden AZT + 3TC bid 3 TDF + FTC qd 2 ABC + 3TC qd 2 AZT + 3TC bid 6 TDF + FTC bid 5 ABC + 3TC bid 5 AZT + 3TC bid 5 TDF + FTC qd 4 ABC + 3TC qd 4 ABC hypersensitivity may be more severe with qd versus bid dosing 10% % of patient with reaction • CNA30021: n = 770 treatment naïve patients randomized to ABC 300mg bid versus ABC 600mg qd • Combined with 3TC plus efavirenz (each once daily) • Equivalent treatment efficacy • ? More severe hypersensitivity with qd dosing 8% 9% ABC 600mg qd ABC 300mg bid 7% 6% 5% 4% 2% 2% 2% 0% 0% hypersensitivity Epzicom package labeling, August 2004 severe hypersensitivity severe diarrhea Which ART regimen performs best in clinical trials? Regimen (trial) Results from Comparable Trials: ITT analysis of VL <400 c/mL at Week 48 AZT + 3TC + IDV (START II) AZT + 3TC + ATV (AI424-034) AZT + 3TC + EFV (AI424-034) AZT + 3TC + ABC (CNA3005) d4T + ddI + IDV (START II) AZT + 3TC + IDV (DMP-006) AZT + 3TC + IDV (AVANTI 2) AZT + ddI + NVP (INCAS) AZT + 3TC + NFV (AVANTI 3) AZT + 3TC + IDV (CNA3005) AZT + 3TC + IDV (START I) d4T + ddI + 3TC (Atlantic) d4T + 3TC + IDV (START I) d4T + ddI + NVP (Atlantic) 2 NRTIs + SQV-SGC (NV-15355) d4T + 3TC + NFV (M98-863) AZT + 3TC + ABC (CNAB3003) d4T + ddI + IDV (Atlantic) AZT + 3TC + EFV (EPV20001) AZT + 3TC + EFV (DMP-006) % with HIV RNA <50 copies/mL at 48 Weeks (ITT) d4T + 3TC + LPV/RTV (M98-863) d4T + 3TC + EFV (GS-903) TDF + 3TC + EFV (GS-903) d4T + 3TC + EFV (GS-903) TDF + 3TC + EFV (GS-903) 0 10 20 30 40 50 Based on: Bartlett. Presented at: 7th CROI; 2000; San Francisco, Calif. Poster 519. 60 70 80 90 100 Selection of the Initial ART regimen: Summary • Regimen potency • Patients’ preference regarding pill burden, dosing frequency, and food and fluid considerations • Potential adverse effects • Baseline antiretroviral resistance profile • Co-morbidity or conditions such as tuberculosis, liver disease, depression or mental illness, cardiovascular disease, chemical dependency, pregnancy, and family planning status • Potential drug interactions with other medications DHHS Antiretroviral Therapy Guidelines, July 2003, p. 14. Case 1, continued You decide to start her on AZT (zidovudine) plus 3TC (lamivudine) plus efavirenz. What are your goals of therapy? What follow up labs do you arrange, and when? Antiretroviral Therapy: Optimal Response ART Initiated CD4 count (cells/mm3) Viral Load (copies/mL) 1000000 Viral Load 100000 10000 1000 100 50 50 10 0 1 2 3 Time (months) 4 5 6 7 8 Antiretroviral Therapy: Optimal Response ART Initiated 200 Viral Load 100000 CD4 Count 150 10000 100 1000 50 100 50 50 10 0 0 1 2 3 4 Time (months) 5 6 7 8 CD4 count (cells/mm3) Viral Load (copies/mL) 1000000 Follow-up Laboratory Testing • Viral load & CD4 counts, initially once monthly after starting therapy; can space out to every 3 months if doing well • Goals are undetectable viral load (<50 or 75 copies/mL) and rise in CD4 count • CBC, electrolytes, LFTs at regular intervals to monitor for toxicity, also when signs or symptoms develop Case 2 • A 33 year old woman with a CD4 count of 30 cells/mm³ initiates antiretroviral therapy with a regimen of AZT + 3TC + nevirapine (NVP) • Initially she feels better, but 3 weeks later she returns complaining of fevers, night sweats, and swollen lymph nodes • Physical examination is remarkable for: – Fever of 38.7 C – Bilateral axillary enlarged, tender lymph nodes – Weight 120 lbs (unchanged from when she initiated ART) What is likely responsible for her symptoms? A. She is having a toxic reaction to her ART medications B. Her ART regimen is not working, as evidenced by development of a new opportunistic infection C. Her ART regimen is working so well that her newly strengthened immune system is reacting against a previously unrecognized infection D. I have no idea what is going on with her Case continued • You order diagnostic tests including blood cultures and a biopsy and culture of her enlarged lymph nodes Gram stain of lymph node: acid-fast bacilli in macrophages. www.med.sc.edu:85/fox/mycobacteria.htm Immune Reconstitution Syndrome • Reflects newly invigorated immune system mounting an inflammatory response against an infection that was previously clinically silent in the face of severe immunodeficiency • Common among patients with robust rise in CD4 count (e.g., over 100 cells/mm³) in the first several weeks following initiation of ART • Typically managed by continuing ART and administering anti-inflammatory medications to control symptoms, such as NSAIDS and/or steroids • Occasionally discontinuation of antiretrovirals is necessary Clinical Presentation & Course of Common Immune Reconstitution Syndromes IRD Clinical Manifestations Onset Typical Course MAC Lymphadenitis, high fever, infiltrates on chest x-ray 1 - 12 wk Resolves with continued ART and antiMAC therapy; may require corticosteroid therapy CMV Retinitis and vitreitis 1 - 2 mo Resolves with continued ART and antiCMV therapy Uveitis 2 mo - 2y Macular edema, epiretinal membrane formation, cataracts Herpes zoster Localized 1 - 4 mo Resolves with acyclovir therapy TB Fever, worsening infiltrates/effusion on chest film, mediastinal and peripheral lymphadenopathy 1 - 6 wk Resolves with continued ART and antituberculous therapy; may require corticosteroid therapy Cryptococcal meningitis New headache, meningismus, increased number of white blood cells in cerebrospinal fluid 1 wk - 8 mo Resolves with continued ART and antifungal therapy IRD, immune restoration disease; MAC, Mycobacterium avium complex; CMV, cytomegalovirus. Qazi NA et al. AIDS Reader 12(10):452-457, 2002. Initial Antiretroviral Therapy: Summary • ART has made HIV a treatable and manageable chronic disease for many patients • ART consists of at least 3 drugs, generally from 2 or more classes • When to initiate therapy remains controversial, but probably best to start before CD4 falls below 200 cells/mm³ • Consider adherence and baseline viral load when designing initial regimen • Goal is undetectable viral load (<50 copies/mL) and rise in CD4 count • Monitor closely after initiation of therapy