Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
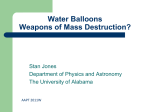
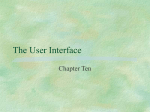
The Internet Journal of Thoracic and Cardiovascular Surgery TM ISSN: 1524-0274 Home | Current Issue | Archives | Instructions for Authors | Disclaimer | Printable Version Intra Aortic Balloon Pump (IABP) Counterpulsation P. J Overwalder, M.D. Department of Surgery I Division of Cardiac Surgery University Hospital Graz Citation: P. J Overwalder: Intra Aortic Balloon Pump (IABP) Counterpulsation . The Internet Journal of Thoracic and Cardiovascular Surgery. 1999. Volume 2 Number 2. Table of Contents History Physiologic Effects of IABP Therapy Control of the IABP Insertion Techniques Complications Experience at a Single Center References History In 1958 Harken described for the first time a method to treat left ventricular failure by using counterpulsation or diastolic augmentation. He suggested removing a certain blood volume from the femoral artery during systole and replacing this volume rapidly during diastole. By increasing coronary perfusion pressure this concept would therefore augment cardiac output and unload the functioning heart simultaneously 1 , 2 . This method of treatment was limited because of problems with access (need for arteriotomies of both femoral arteries), turbulence and development of massive hemolysis by the pumping apparatus. Even experimental data showed that no augmentation of coronary blood flow was obtained 3 . Then in the early 1960s Moulopoulus et al. 4 , 5 from the Cleveland Clinic developed an experimental prototype of the intra-aortic balloon (IAB) whose inflation and deflation were timed to the cardiac cycle. In 1968 the initial use in clinical practice of the IABP and it`s further improvement was realized resp. continued by A. Kantrowiz`s group 6 , 7 . In its first years, the IABP required surgical insertion and surgical removal with a balloons size of 15 French. In 1979 after subsequent development in IABP technology a dramatic headway with the introduction of a percutaneous IAB with a size of 8,5 to 9,5 French was achieved 8 , 9 . This advance made it for even nonsurgical personnel possible, to perform an IAB insertion at the patient’s bedside. In 1985 the first prefolded IAB was developed. Today continued improvements in IABP technology permit safer use and earlier intervention to provide hemodynamic support. All these progresses have made the IABP a mainstay in the management of ischemic and dysfunctional myocardium. Physiologic Effects of IABP Therapy After correct placement of the IAB in the descending aorta with it`s tip at the distal aortic arch (below the origin of the left subclavian artery) the balloon is connected to a drive console. The console itself consists of a pressurized gas reservoir, a monitor for ECG and pressure wave recording, adjustments for inflation/deflation timing, triggering selection switches and battery back-up power sources. The gases used for inflation are either helium or carbon dioxide . The advantage of helium is its lower density and therefore a better rapid diffusion coefficient. Whereas carbon dioxide has an increased solubility in blood and thereby reduces the potential consequences of gas embolization following a balloon rupture. Inflation and deflation are synchronized to the patients’ cardiac cycle. Inflation at the onset of diastole results in proximal and distal displacement of blood volume in the aorta. Deflation occurs just prior to the onset of systole (Fig. 1) . Figure 1: Intra aortic balloon (IAB) during systole and diastole The primary goals of IABP treatment are to increase myocardial oxygen supply and decrease myocardial oxygen demand. Secondary, improvement of cardiac output (CO), ejection fraction (EF), an increase of coronary perfusion pressure, systemic perfusion and a decrease of heart rate, pulmonary capillary wedge pressure and systemic vascular resistance occur 10 , 11 , 12 (Tab.1) There are several determinants of oxygen supply and demand (Tab.2). Table 1: Hemodynamic effects of IABP Therapy Table 2: Determinants of Myocardial Oxygen Supply and Demand In particular systolic wall tension uses approximately 30% of myocardial oxygen demand. Wall tension itself is affected by intraventricular pressure, afterload, enddiastolic volume and myocardial wall thickness. Regarding to the studies of Sarnoff et al. the area under the left ventricular pressure curve, TTI (= tension-time index ), is an important determinant of myocardial oxygen consumption 13 . On the other hand, the integrated pressure difference between the aorta and left ventricle during diastole (DPTI = diastolic pressure time index) represents the myocardial oxygen supply (i.e. hemodynamic correlate of coronary blood flow) 14 , 15 . Figure 2: Schematic representation of coronary blood flow, aortic and left ventricular pressure wave form with / without IABP. (Effects on DPTI and TTI . Balloon inflation during diastole augments diastolic pressure and increases coronary perfusion pressure as well as improving the relationship between myocardial oxygen supply and demand (DPTI:TTI ratio) a) Inflation of the balloon during diastole (= augmentation of the aortic diastolic pressure) increases coronary blood flow ( DPTI ). b) Deflation of the balloon occurs just prior to the onset of systole and reduces impedance to left ventricular ejection (TTI ). This results in less myocardial work, decreased myocardial oxygen consumption and increased cardiac output 16 . Control of the IABP TRIGGERING To achieve optimal effect of counterpulsation, inflation and deflation need to be correctly timed to the patient’s cardiac cycle. This is accomplished by either using the patient’s ECG signal, the patient’s arterial waveform or an intrinsic pump rate. The most common method of triggering the IAB is from the R wave of the patient’s ECG signal. Mainly balloon inflation is set automatically to start in the middle of the T wave and to deflate prior to the ending QRS complex. Tachyarrhythmias, cardiac pacemaker function and poor ECG signals may cause difficulties in obtaining synchronization when the ECG mode is used. In such cases the arterial waveform for triggering may be used. TIMING and WEANING It is important that the inflation of the IAB occurs at the beginning of diastole, noted on the dicrotic notch on the arterial waveform. Deflation of the balloon should occur immediately prior to the arterial upstroke. Balloon synchronization starts usually at a beat ratio of 1:2. This ratio facilitates comparison between the patient’s own ventricular beats and augmented beats to determine ideal IABP timing. Errors in timing of the IABP may result in different waveform characteristics and a various number of physiologic effects (Fig. 3). Figure 3: Arterial pressure wave form alterations associated with inflation and deflation of the IAB If the patient’s cardiac performance improves, weaning from the IABP may begin by gradually decreasing the balloon augmentation ratio (from 1:1 to 1:2 to 1:4 to 1:8) under control of hemodynamic stability . After appropriate observation at 1:8 counterpulsation the balloon pump is removed. Indications and Contraindications (Table 3) Early purposed indications for intraaortic balloon pumping have included cardiogenic shock or left ventricular failure, unstable angina, failure to separate a patient from cardiopulmonary bypass and prophylactic applications, including stabilization of preoperative cardiac patients as well as stabilization of preoperative noncardiac surgical patients 10, 17 , 18 , 19 , 20 , 21 . Today more extending indications are: Cardiac patients requiring procedural support during coronary angiography and PTCA, or as a bridge to heart transplantation. Further on in pediatric cardiac patients and as well as in patients with stunned myocardium, myocardial contusion, septic shock and drug induced cardiovascular failure the IABP can be life-saving 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 IABP therapy should only be considered only for use in patients who have the potential for left ventricular recovery, or to support patients who are awaiting cardiac transplantation. Absolute contraindications of IABP are relatively few (Tab.3). There are successful reports of its usage in patients with aortic insufficiency 32 , 33 and in patients with acute trauma to the descending aorta 34 . Table 3: IABP Counterpulsation Indications and Contraindications Insertion Techniques In the early years of IABP - therapy, insertion of the balloon was performed by surgical cut down to the femoral vessels. After a longitudinal incision in the groin, the femoral arteries were identified and controlled. A vascular graft was then sewn to the common femoral artery in an end-to-side fashion. The balloon was introduced into the artery via the graft and properly positioned in the thoracic aorta and the graft tightly secured to the distal portion of the balloon catheter. Finally the skin incision was closed. Removal of the balloon required a second operation. Since 1979, a percutaneous placement of the IAB via the femoral artery using a modified Seldinger technique allows an easy and rapid insertion in the majority of situations. After puncture of the femoral artery a J-shaped guide wire is inserted to the level of the aortic arch and then the needle is removed. The arterial puncture side is enlarged with the successive placement of an 8 to 10,5Fr dilator/sheath combination. Only the dilator needs to be removed. Continuing, the balloon is threaded over the guide wire into the descending aorta just below the left subclavian artery. The sheath is gently pulled back to connect with the leak-proof cuff on the balloon hub, ideally so that the entire sheath is out of the arterial lumen to minimize risk of ischemic complications to the distal extremity. Recently sheathless insertion kits are available. Removal of a percutaneously placed IAB may either be via surgical removal or closed technique. There are alternative routes for balloon insertion. In patients with extremely severe peripheral vascular disease or in pediatric patients the ascending aorta or the aortic arch may be entered for balloon insertion 35 , 36 . Other routes of access include subclavian, axillary or iliac arteries 37 , 38 , 39 . Complications Although the incidence of complications has decreased significantly as experience with the device has increased, IABP therapy in today’s patients` population does still hold a risk for complications (Tab.4). Because today’s patient population is elderly (68 - 80 years), very often female and may suffer from severe peripheral vascular disease and hypertension or diabetes. The most common vascular complication is limb ischemia. It may occur in 14-45% of patients receiving IABP therapy 40 , 41 . Therefore the patient must be consistently observed for any symptoms of ischemia during IABP counterpulsation. If signs of ischemia appear the balloon should be removed. In general, vascular injuries should be dealt with directly by surgical interventions and repair. Balloon related problems and infection require removal and / or replacement of the IAB . Table 4: Complications of IABP counterpulsation Experience at a Single Center Treatment of low cardiac output syndrome using IABP counterpulsation has been used at our institution since 1983. Till December 1993 a total number of 440 patients (pts) (9,95%) out of 4420 patients, who underwent cardiac surgery procedures with the use of cardiopulmonary bypass, were supported with an IABP.(Age distribution : Tab. 6) There were 294 male and 146 female patients. Overall survival rate after implantation of the IABP was 75% (n=330 pts) . Table 5: Diagnosis prior to IABP implantation Table 6: Age Distribution of IABP patients In the early years (1983-1989) as method of choice, implantation of the balloon was performed via a surgical cut down of the femoral artery. Complications were observed in 20 pts (8.4%) : In 9 pts (3.7%) positioning of the balloon was impossible due to severe vascular disease, 5 pts (2.1%) developed a thrombosis of the femoral artery and 1 patient (0.4%) died because of untreatable thrombosis of the mesenteric artery. Hospital mortality in this group was 36% (survival rate of 64%). Mean pumping time was 3 days (1 - 15). Since 1990 we prefer the percutaneous insertion of the device. After a learning curve more than 90% of 202 patients received an IABP using this technique. Complication rate was less than 8% (mainly leg ischemia with amputation of the leg in 1 patient, 3 infections of the puncture point and 4 cases of impossible positioning of the balloon ). Survival rate was 68.5% (hospital mortality of 31.5%) . 278 pts (63%) received the balloon pump at the operating theater - mainly because of failure to wean from cardiopulmonary bypass -151 pts (34,3%) at an intensive care unit and 11 pts (2,5%) as a bridge to transplant. Table 6 shows a detailed list of all various diagnoses prior to IABP therapy . References 1. Harken DE (1958) Presentation at the International College of Cardiology, Brussels, Belgium 2. Harken DE (1976) Circulatory assist devices. Med Instrum 10: 215 3. Dormandy JA, Goetz RH, Kripke DC (1969) Hemodynamics and coronary blood flow with counterpulsation. Surgery 65: 311 4. Moulopoulos SD, Stephen R, Topaz S et al (1962) Extracorporeal assistance to the circulation and intraaortic ballon pumping. Trans Am Soc Artif Int Org 7: 85 5. Moulopoulos SD, Topaz S, Kolff WJ (1962) Diastolic balloon pumping (with carbon dioxide) in the aorta - a mechanical assistance to the failing circulation. Am Heart J 63: 669 6. Kahn JK, Rutherford BD, McConahay DR (1990) Supported High Risk coronary angioplasty using intraaortic balloon pump counterpulsation. J Am Coll Cardiol 15: 1151 7. Kantrowitz A, Tjonneland S, Freed PS et al (1968) Inital clinical experience with intraaorta balloon pumping in cardiogenic shock. JAMA 203: 113 8. Bregman D, Casarella WJ, (1981) Percutaneous intraaortic balloon pumping: Initial clinical experiences. Ann Thorac Surg 29: 153 9. Hauser AM, Gordon S, Ganzadharen V et al (1982) Percutaneous intraaortic balloon counterpulsation . Clinical effectiveness and hazards. Chest 82: 422 10. Bolooki H (1984) Clinical application of Intra-Aortic Ballon Pump. Mount Kisco, NY, Futura Publishing 11. Sarnoff SJ, Braunwald E, Welch GH et al (1958) Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension time index. Am J Physiol 192: 148 12. Akyurekli Y, Taichmann JC, Keon WJ (1980) Effectivness of intra aortic balloon counteroulsation and systolic unloading. Can J Surg 23: 122 13. Pennington DG, Swartz MT (1990 ) Mechanical circulatory support prior to cardiac transplantation. Sem Thor & Cardiovasc Surg 2(2): 125 14. Grotz RL, Yeston NS (1989) Intraaortic balloon counterpulsation in high risk cardiac patients undergoing non cardiac surgery. Surgery 106: 1 15. Hoffman JIE, (1978) Determinants of prediction of transmural myocardial perfusion Circulation 58: 381 16. Lembo NJ (1989) Failed angioplasty and intraaortic balloon pumping. Cardiac assist 5(1): 5 17. Ayers Sm, (1988) The prevention and trearment of shock in acute myocardial infarction. Chest 93 (suppl): 17S 18. Bolooki H (1989) Emergency cardiac procedures in patients in cardiogenic shock due to complications of coronary artery disease. Circulation 79 (suppl I): I-137 19. Georgen RF, Diertrick JA, Pifarre R, et al. (1989) Placement of intraaortic balloon pump allowing definitive surgery on patients with severe cardiac disease. Surgery 106: 808 20. Golding LAR, Loop FD, Petes M, et al. (1980) Late survival following use of intraaortic balloonpumping in revascularization surgery. Ann Thorac Surg 30: 48 21. Grotz RL, Yeston NS (1989) Intraaortic balloon counterpulsation in high risk cardiac patients undergoing non cardiac surgery. Surgery 106: 1 22. Anwar A, Mooney MR, Sterzer SH (1990 ) Intra-aortic balloon counterpulsation support for elective coronary angioplasty in the setting of poor left ventricular function: A two center experience. J.Invas.Cardiol.1(4): 175 23. Bavaria JE, Furukawa S, Kreiner G (1990) Effect of circulatory assist devices on stunned myocardium. Ann Thorac Surg 49: 123 24. Freedberg RS, Friedmann GR, Palu RN, et al. (1987) Cardiogenic shock due to antihistamine overdose. Reversal with intraaortic balloon counterpulsation JAMA 257: 660 25. Iberer F, Roupec R, Dacar D, et al (1990) Surgical Implantation of the intra-aortic balloon pump via the arteria femoralis . Angio 12(2) : 43 26. Lamberti JJ, Cohn LH, CollinsJJ Jr, (1974) Iliac artery cannulation for intraaortic balloon counterpulsation. J Thorac Cardiovasc Surg 67: 976 27. Lane AS, Woodward AC, Goldman MR (1987) Massive propranolol overdose poorly responsive to pharmacologic therapy: Use of the intra aortic balloon pump. Ann Emerg Med 16(12): 1381 28. McBride LR, Miller LW, Nauheimer KS, et al. (1989) Axillary artery insertion of an intraaortic balloon pump. Ann Thorac Surg 48: 874 29. Mercer D, Doris P, Salerno TA (1981) Intra-aortic counterpulsation in septic shock Can J Surg 24(6): 643 30. Ohmann EM, Califf RM, George BS, et al. (1991) The use of intraaortic balloon pumping as an adjunct to reperfusion therapy in acute myocardial infarction Am Heart J 121: 895 31. Shirkey AL, Loughridge BP, Lain KC (1976) Insertion of the intraaortic balloon through the aortic arch. Ann Thorac Surg 21: 560 32. Vigneswaran WT, Reece IJ, Davidson KG (1985) Intraaortic balloon pumping : seven years`experience. Thorax 40: 858 33. Yellin E, Levy I, Bregman D, et al (1973) Hemodynamic effects of intraaortic balloon pumping in dogs with aortic incompetence. Trans Am Soc Artif Intern Org 19: 389 34. Ammons MA, Moore EE, Moore FA, et al (1990) Intraaortic balloon pump for combined myocardial contusion and thoracic aortic rupture. J Trauma 30: 1606 35. Gueldner TL, Laurence GH (1975) Intraaortic balloon pumping in children. Ann Thorac Surg 19: 88 36. Shaw J, Taylor DR, Pitt B (1974) Effects of intraaortic balloon counterpulsation in regional coronary blood flow. Am J Card 34: 552 37. KantrowitzA, Wasfie T, Freed PS, et al. (1986) Intraaortic balloon pumping 1967 through 1982: Analysis of complications in 733 patients. Am J Cardiol 57: 976 38. Maccioli GA, Lucas WJ, Norfleet EA (1988) The intra-aortic balloon pump: A review. J. Cardiothor. Anesth. 2: 365 39. Mayer JH (1978) Subclavian artery approach for insertion of intra-aortic Balloon J Thorac Cardiovasc Surg 76: 61 40. Kantrowitz A, Tjonneland S, Krakauer J et al (1968) Clinical experience with cardiac assistance by means of intra aortic phaseshift balloon pumping. Trans Am Soc Artif Intern Org 14: 344 41. Mayer JH (1978) Subclavian artery approach for insertion of intraaortic Balloon J Thorac Cardiovasc Surg 76: 61