Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
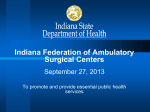
RareMetastaCcLesionsoftheInternalAuditoryCanal RichardJ.Wiet,MD1,2;RobertA.Balsta,MD1,2;R.MarkWiet,MD3; RichardByrne,MD4;ArnoldRivera,MD5;JennaLiole,BS1 1EarIns>tuteofChicago,2Northwestern University Feinberg School of Medicine –Dept. of Otolaryngology, 3 Rush University Medical Center – Dept. of Otorhinolaryngology, 4 Rush University Medical Center – Dept. Neurosurgery, 5 University of Missouri –Dept. of Otolaryngology Abstract Thegoalofthisstudyistoelucidatethekeydifferencesbetweenthemore commonves>bularschwannoma(VS)oftheinternalauditorycanal(IAC),andthe raremetasta>clesiontotheIAC. Studydesign:Retrospec>vecaseseries Selng:Ter>aryreferralcenter Methods:History,histology,audiogram,MRIscans,cerebrospinalfluid(CSF) cytologywereviewedofpa>entswhohadmetasta>clesionstotheIAC. Dis>nguishingpaoernsofthemetasta>ccasestotheIACwereanalyzed. Results:Eachpa>enthadahistoryofpriormalignancy.Themostfrequent metastasescamefromthebreast-threeoftheseventotalcases.Otherprimary malignanciesoriginatedfromtheparo>d,gastric,andthecolon.Theprimary malignancyloca>onforonecasecouldnotbeiden>fied.Allsevenpa>ents complainedofsomedegreeofhearingloss,fiveaccompaniedwithdizziness,and threewithfacialparesis.Fourpa>entshadbilateralneoplasmswithintheIAC. LeptomeningealcarcinomatosiswasfoundintwoCSFsamples.Avariedformof adenocarcinomawasiden>fiedinthreemetastasesfollowedbyinfiltra>ng lobularcarcinomapleomorphicvariant;invasive,andhighgradeductal carcinoma;andmoderatelydifferen>atedsquamouscellcarcinoma.Thedura>on betweendiagnosisofmetastasistotheIAC,andiden>fica>onoftheprimarysite rangedfrom24to48months. Conclusion:Metasta>cdiseasetotheIAC/CPangleshouldbesuspectedincases withsuddenhearingloss,ageexceeding55years,facialnerveneuropathy,anda historyofpriormalignancy.CSFcytologyshouldbeconsideredasadiagnos>ctool incasessuspectedofmetasta>cdisease. IntroducCon Refinementsinneuroradiologyhavecontributedtothediagnosisofmoresubtle internalauditorycanal(IAC)lesionsthroughmagne>cresonanceimaging(MRI). Subtlelesionsmaybedifficulttodifferen>atebetweenthemorecommon ves>bularschwannomaandametasta>clesion.Apasthistoryofaprior malignancy,e.g.,lungcarcinomaorbreast,mandatesconsidera>onformetastasis totheIACfromadistantsite.Metastasiscanoccurbytheseedingofmalignant cellsintotheleptomeningesfromasolidtumor.Metastasismaypresentwithor withoutanaccompaniedcranialnerveneuropathysuchasfacialparesis. Ves>bularschwannomaandmetasta>clesionstotheIACmayappearnearly iden>caloninfusedMRI.Therehavebeenfewmetasta>cIACcasesreportedin theliterature.Itissuspectedthattheactualincidencemaybeunderes>mated. Theobjec>veofthisstudyistoelucidatefactorssuppor>ngthesuspicionofa metasta>ctumortotheIAC. MethodsandMaterials SevencasesofmetastasistotheIACwereobtainedfromEarIns>tuteofChicago (EIC),fromRushUniversityMedicalCenterandfromtheU.ofMissouri.An addi>onalcasewassubmioedbyA.Rivera,formerfellowofEIC.Caseswere monitoredoveranumberofmonths. Results Please,refertothetablebelow.Primaryistheoriginalmalignantsite,andthe metasta>csideistheloca>onofthetumorwithintheleAorrightIAC/CPA. “None”underCSFcytologydenotesatestwasnotperformedordisclosed.“NA” indicatesnotavailablefromtherecord. Case Age Sex Primary Discussion MetastasistotheIACfromadistantsiteistypicallyknownasleptomeningeal carcinomatosis.Metasta>cseedingoftheleptomeningesoccursbyhematogenousspread, ordissemina>onthroughveinsorlympha>cs.Themostfrequentprimarysitesof malignancythatmetastasizetotheIACarethelungs,followedbythebreast,andGItract.1 Malignantreportablecasesnumberinthelowhundredsmakingdetec>ondifficult.Similar configura>onsbetweenmetasta>clesionsandVS,ongadoliniumenhancedMRIoftheIAC, haveledtorecommenda>onsforhighresolu>onMRI,wheresegmentsofthecranialnerves maybethickened.2Proteininthesubarachnoidspacefromfluidaoenuatedinversion techniquescanalsosuggestmetasta>cdisease.3Perfusionweightedimaging(PWI)MRI, withlowperfusionparametersraisethesuspicionofmetasta>cfocus.4PET/CTscansare notaccurateatthebaseoftheskull.BilateralIACmetastases,asseenwithcases3,4,5and 6,canoAenbeconfusedwithNeurofibromatosisII,especiallyinyoungpa>ents. Lumbarpuncturemayassistindiagnosis,ascytologymaybeposi>veformalignantcells. However,20-50%ofpa>entswithleptomeningealcarcinomatosismayhavenega>ve cytology(asincase6).ElevatedlymphocyteandproteininCSFareconsistentbutnot diagnos>cofmetastasis.Recently,CSFbiomarkersaidinreducingtheamountof malignancyneededforaposi>vereading.Forexample,CSFanalysiswithcarcinoembryonic an>gen(CEA)canbeusedasabiochemicalmarkerwhensuspiciousofadenocarcinoma.5 Neweremphasisisplacedoncancergenomics,classifyingtheDNAofeachlesiontotailor treatmentsanddefinethemechanismofbrainmetastasis.6 Generally,metastasistotheIACoccursinolderindividualswithahistoryofcancer.Fiveof ourcaseswereolderthan50.7Cranialnerve7deficitisafrequentsignofleptomeningeal carcinomatosisoftheIAC;threeofourcasespresentedwithfacialweakness.Rapid unilateralorbilateralhearinglosswasthemosttypicalcomplaintinourcaseseries.Sudden orrapidlyprogressivehearinglossistypicallythefirstsign,andfacialnervepalsy,whichis lesscommon,canoAensuggestmalignancy.8Inourcases,allpa>entswiththeexcep>onof 1,diedwithin12monthsaAerdiagnosis. Figure1. Case3:MetastaCc breastcarcinoma infiltraCngmiddleear andpermeaCng ganglion(1031k) MRIfromcase4witharrowsindicaCngmetastaCc diseasebilaterallytotheIACs Figure2. Case3:NeoplasCccells areposiCvefor cytokeraCn(x200) ImagesprovidedbyPaoloGaouso,MD,RushUniversityPathology Figure1:1031k,Figure2:855k Conclusions IndividualswithIACmetasta>cdiseasetypicallyhaveapasthistoryofaprimarymalignancy elsewhere.Whenpresentedwithsuchacase,theclinicianshouldbesuspiciousof malignancyespeciallywhenthereisasuddendropinhearingwithassociatedwithfacial neuropathyinanolderindividual.ThetreatmentforIACmetastasiscanvary,butgenerally radiotherapyandchemotherapyispreferred.Surgeryisretainedforyoungerindividuals withasinglelesionsymptoma>cfromseverever>go,orrequiredforofficialdiagnosisand treatmentmodality.Thesurvivalofpa>entsdiagnosedwithIACmetastasesisoAena maoerofmonths. MetastaCc ENTSymptoms (Side) CSFCytology Approximate monthsbetween MetastaCc& Primaryfinding Approximate Histology monthsbetween Metastasis& Death 1 59 M Paro>d IAC(R) Dizziness,hearingloss None 24 19 Highgradeductalcarcinoma 2 74 M Unknown IAC(L) Dizziness,hearingloss,facialweakness None 48 8 Moderatelydifferen>atedsquamouscell carcinoma 3 41 F Breast IAC(B) Dizziness,earfullness,headaches,bilateral>nnitus,hearingloss Posi>ve(metasta>cbreast carcinoma) 28 5 Adenocarcinomamammarytype 4 68 F Colon IAC(B) Dizziness,facialweakness,suddenhearingloss Posi>ve(Probable Malignancy) NA 1 Colonadenocarcinoma. 5 50 M Gastric IAC(B) Dizziness,facialweakness,bilateralsuddenhearingloss,bilateral>nnitus None NA 0.5 Adenocarcinoma 6 59 F Breast IAC(B) Dizziness,hearingloss,seizures Nega>ve 30 Aliveasof2011 Lobularcarcinomapleomorphicvariant 7 33 F Breast IAC/CPA(R) HearingLoss,Intermioenthoarsenessanddysphasia None 24 Aliveasof2015 InvasiveDuctalcarcinoma References Contact RichardJ.Wiet,MD 11SaltCreekLn.Ste.101 HinsdaleIL,60521 1. DellaPupa,A,RosseooM,Ber>,F,etal.InternalAuditorycanalmetastasis.JournalofNeurosurgicalSciences.2010;54(4):159-162. 2. DemopoulousA.Clinicalfeaturesanddiagnosisofleptomeningealmetastasesfromsolidtumors.UpToDatewebsite.hop://www.uptodate.com/contents/clinical-features-and-diagnosis-of-leptomeningeal-metastases-from-solid-tumors.April22, 2015.AccessedNovember5,2015. 3. SinghSK,LeedsNE,GinsbergLE.MRimagingofleptomeningealmetastases:comparisonofthreesequences.AmericanJournalofNeuroradiology.2002;23:817-821. 4. ZimnyA,SasiadekM.Contribu>onofperfusionweightedmagne>cresonanceimaginginthedifferen>a>onofmenigiomasandotherextra-axialtumors:casereportandliteraturereview.JournalofNeuro-Oncology.2011;103(3):777-783.doi: 10.1007/s11060-010-0445-9. 5. KangSJ,KimKS,HaYS,etal.Diagnos>cvalueofcerebrospinalfluidlevelofcarinoembryonican>geninpa>entswithleptomeningealcarcinomatousmetastasis.JournalofClinicalNeurology.2010;6:33-37.doi:10.3988/jcn.2010.6.1.33. 6. LeeJ,ParkK,LimS,etal.Muta>onalProfilingofBrainMetastasisfromBreastCancer:MatchedPairAnalysisofTargetedSequencingBetweenBrainMetastasisandPrimaryBreastCancer.Ocotarget.2015;6(41):43731-43742.doi:10.18632/ oncotarget.6192. 7. RohlfsAK,BurgerR,ViebahnC,StrutzJ.Uncommonlesionsintheinternalauditorycanal(IAC):reviewoftheliteratureandcasereport.JournalofNeurologicalSurgery-PartA:CentralEuropeanNeurosurgery.2012;73(3):160-166.doi:10.1055/ s-0032-1304211. 8. FalcioniM,PiccirilloE,DiTrapaniG,RomanoG,RussoA.Internalauditorycanalmetastasis.ActaOtorhinolaryngologicaItalica.2004;24(2):78-82.