Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
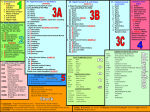
PATIENT ASSESSMENT: I. II. III. BSI Precautions Scene Size Up Initial Assessment IV. Rapid Trauma Assessment or Focused History and Focused Physical Exam V. VI. VII. VIII. Patient History (s.a.m.p.l.e. History) Detailed Physical Exam Ongoing Assessment Patient Hand-off & FRPCR I. BSI Precautions II. Scene Size Up: Scene safe? NOI or MOI (nature of Illness or Mechanism of Injury) Number of patients Additional resources Update EMS regarding additional resources and any other information. Considers Stabilization of c-spine? III. Initial Assessment: Identify and treat Immediate and obvious life threats. General Impression: *General appearance (Well, ill, injured) *Age, sex, *Pat’s chief complaint/ MOI (why was EMS called) *Trauma (penetrating or blunt force) or medical, *Brief assessment of environment in which emergency has taken place. *Identify and treat immediate and obvious life threats. *Position patient for assessment Responsiveness: check for altered mental status. Use AVPU scale. A- ALERT- responsive, alert, oriented. (Oriented x 3? Responsive to person, place & date) V- Verbal- Disoriented, but responds to verbal stimuli. (doesn’t know place or date) P- Painful- Responds only to painful stimuli. (pinch or sternal rub only if necessary) U- UNRESPONSIVE- Does not respond to any stimulus, does not open eyes, respond verbally or flinch with pain. Airway & Breathing *Open airway (head tilt chin lift/ jaw thrust) and make sure it is patient (Suction?) (Can conscious pat. speak?) *Airway adjunct (unconscious, semi-unconscious) *Assess breathing (adequate/ inadequate) (rate and volume) (signs of inadequate breathing) *Initiate appropriate oxygen therapy consider ventilations *Expose chest, check for injuries and treat life threats *Check for equal chest rise on both sides. Circulation: (Pulse Rate, Rhythm & Adequacy) (Skin Condition, Color, Refill & Temp.) *Presence or absence of pulse. (rate, rhythm, adequacy) Is heart pumping blood to all parts of body adequately? (Any cyanosis?) *Responsive adult pat. use radial pulse, child radial or brachial, infant brachial. *Unresponsive adult pat. check carotid, child carotid or femoral, infant brachial. *IN ALL IF PULSE IS ABSENT, BEGIN CPR. *Assess pat’s. skin at this time as well (color, temp., capillary refill & condition). Signs of shock. (Capillary refill at room temp. 2s infants, c hildren adult male; 3s for adult female; 4s elderly) *Perform a BLOOD SWEEP checking for & treating serious external bleeding. Priority: *At this point you should be able to prioritize your patient. -High priority pats. (not breathing or need ventilating). -Low priority pats. (stable, minor complaints). *Update EMS on patient status. Report the following: -Pats. Age & Sex -Chief complaint -Level of Responsiveness -Airway & Breathing status -Circulation status to include severe bleeding -Vital signs (if any have been taken to this point) *Ask EMS for ETA so you can continue pat. care and prepare for EMS arrival. IV. Rapid Trauma Assessment (and immediate transport) OR: Focused History and Focused Physical Exam (on scene) If doing a rapid trauma assessment, perform as you would a detailed physical exam but only treat life threats. Treat secondary non-life threats during detailed physical exam. The rapid trauma assessment should take about 60 to 90 seconds. Inspect, palpate, auscultate (with stethoscope), listen, and smell. Begin with the head and work to the feet. You may use DOTS (Deformities, open injuries, tenderness and swelling) or DCAPBTLS (Deformities, contusions, abrasions, punctures, burns, tenderness, lacerations, swelling). BE SURE TO GET A BASELINE SET OF VITALS and record your findings (Blood pressure, pulse rate, respiration rate, pulse ox) Head: Inspect and palpate scalp and skull, inspect and palpate face, including ears (for cerebral spinal fluid), pupils for PERRL (Pupils equal round and reactive to light, nose and mouth for any signs of injuries that may be blocking the airway. D- DEFORMITIES O- OPEN INJURIES T- TENDERNESS S- SWELLING Neck: Inspect the neck for tracheal deviation, jugular vein distention, large lacerations and punctures. Palpate both the anterior and posterior aspects of the neck. Note posterior muscle spasms that may indicate injury to the c-spine. Apply cervical collar. Dress puncture with an occlusive dressing sealed on 4 sides. DOTS- Chest: Expose the chest. Inspect and palpate for open wounds, flail segments, muscle retractions, and uneven chest movement (paradoxical movement). Perform a quick four point auscultation of the chest to listen for the presence and equality of breath sounds. Listen to upper right lung, upper left lung, lower left lung, lower right lung. Dress a chest puncture with an occlusive dressing sealed on 3 sides. Dress a flail chest with a bulky dressing and do not tape all the way around the patient. DOTS- Abdomen: DOTS- Examine the 4 quadrants. Palpate quadrant patient complains of pain in last. Look for any evidence of trauma or distention. Palpate for tenderness and rigidity. Pelvis: (Push in and gently pull down) inspect for evidence of trauma. If patient complains of pain or there is obvious deformity, do not palpate. DOTS- Extremities: Include pulse evaluation, movement & sensation in each extremity. Do a 4 point inspection of each extremity. DOTS- Back: Only if no spinal injury or with proper number of responders trained in rolling pat. Look for any injuries including penetrating injuries. ROLL PATIENT ONTO SPINE BOARD. DOTS- Vitals: Obtain a baseline set of vitals Obtain & record complete set of vitals to include Blood pressure, pulse rate, respiration rate, pupil evaluation, and pulse ox. (BP auscultation preferred, palpation acceptable. V. Patient History: (S.A.M.P.L.E history) Begin history with open ended question like “Why did you call today” or “Describe how you feel”. Cannot conduct if patient is unconscious, instead attempt to obtain information from bystanders. Signs and Symptoms: (OPQRST) *Sign- can be observed. *Symptom- can not be observed, rather must be described by pat. Onset- when did it start? What were you doing? Provokes- what makes it worse or better? Quality- What is pats. description of pain? Radiates- Where is the pain? What does it feel like? Does it radiate out to any other part of the body? Severity- On a 1-10 scale (1 = good, 10 = worst pain of life) have pat. rate pain. Time since onset- How long have you had this problem? Allergies: *Are you allergic to medications or foods? *What happened the last time you had a reaction? Medications: *What medications do you take? *How much did you take and when? Pertinent Past History: *Do you have heart problems, breathing problems, diabetes, mental illness, high blood pressure, seizures, other illnesses? *Did you fall? Last oral intake: *When/what did you last eat or drink? *Have you consumed any alcohol or recreational drugs today? Events leading up to the injury or illness: *What happened before the incident? *What occurred between onset and EMS arrival? *What where you doing when the incident occurred? VI. DETAILED PHYSICAL EXAM: (And management of secondary/non-life threating injuries) Conduct just as you did for rapid trauma assessment except slow down and manage all secondary injuries) Head: DOTS- Neck: DOTS- Chest: Be sure to conduct a 4 point auscultation in addition to inspection and palpation. DOTS- Abdomen: Examine the 4 quadrants. Palpate quadrant patient complains of pain in last. DOTS- Pelvis: (Push in and gently pull down) DOTS- Extremities: Include pulse evaluation, movement & sensation in each extremity. DOTS- Back: Only if no spinal injury or with proper number of responders trained in rolling pat. DOTS- VII. ONGOING ASSESSMENT: Continually reassess you patient until pat. is turned over to EMS. *Reassess stable pat. every 15 min. *Reassess unstable pat. every 5 min. *Reassess vital signs *Reassess level of responsiveness (AVPU) *Reassess & correct any airway problems. *Reassess breathing for rate & quality. Ventilate if necessary. *Reassess pulse for rate and quality. *Reassess skin temp., color, refill & condition. *Repeat any portions of physical exam that might be necessary (BP, pupils etc.) *Reassess you interventions (treatment) to see if they are effective. *Continue to calm and reassure the patient. VIII. Handoff Report: *When EMT/ Paramedics arrive, you must be prepared to tell them appropriate information about your patient and any treatment you have provided. The following should be included in your Handoff Report: *Age & Sex of patient *Chief complaint *Level of Responsiveness (AVPU) *Airway and Breathing status *Circulation status *Physical Exam findings including Vitals. *Patient history *Interventions (treatments) and patient’s response to them *Any changes you may have observed. Example: This is George Jeffers. He is 62 and his wife could not wake him from a nap. He responds only to painful stimulus. We had to suction him and assist ventilations. The physical exam did not turn up anything, but his wife says he has diabetes. He took his insulin, had a small meal and then worked all morning in the yard. His wife says this has happened before. His vitals were pulse 120 and weak, respirations 10 and shallow, blood-pressure110/68. Pupils were equal and reactive and skin cool and moist.