Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Rheumatic fever wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Aortic stenosis wikipedia , lookup
Artificial heart valve wikipedia , lookup
Electrocardiography wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
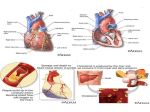
ISCHEMIC HEART DISEASE STUDY GUIDE PAT 823 Use this document to further enhance your understanding of Dr. O'Connor's lecture / handout on ischemic heart disease. Note that this does NOT represent additional study material. It is simply a study guide. Page numbers refer to the handout. PAGE 1 IHD occurs when the heart’s muscle is not receiving enough blood, and therefor is not being adequately oxygenated. There are several causes of this that are listed under “Basis for Coronary Perfusion Imbalance”. To expand upon a few of these: 1. Atherosclerosis narrows the lumen of a coronary artery. This stenosis causes blood flow to the heart to be diminished. 2. Arterial “spasm” refers to a prolonged state of contraction of the smooth muscle within the walls of the coronary artery. This vasoconstriction leads to narrowing of the coronary artery lumen. 3. Systemic hypotension decreases blood flow to all organs and tissues, including the heart. 4a. The coronary arteries originate directly off the aorta, immediately above the aortic valve. Therefore, certain diseases of the aortic valve can partially or totally occlude the ostia (origin) of the coronary arteries, causing decreased blood flow to the heart. 4b. Syphilis can cause disease to the aorta right at the area of the coronary artery ostia. Causes stenosis and decrease blood flow through the coronaries. 4c. Polyarteritis is a general term referring to inflammation of the walls of arteries. Results in thickening and narrowing of the arteries. Can affect the coronaries. 4d. Kawasaki disease (aka mucocutaneous lymph node syndrome) is a multifaceted, complicated disease that affects the young. For our purposes, it is important because it causes an arteritis (inflammation) of the coronary arteries. This can lead to such problems as aneurysm formation with superimposed thrombus, thus causing decrease blood flow through the coronaries. You certainly need to know the 5 major clinical consequences of atherosclerotic coronary artery disease (CAD): 1. Angina pectoris- Covered well in handout. Keep in mind, the heart injury seen in AP is reversible, i.e. the injured area is NOT necrotic. Once you rest, the area returns to normal health. Unstable angina refers to a change in a patient’s angina “pattern”. E.g. For a particular person, it normally takes walking up 10 stairs to trigger off angina. Later, only 5 stairs trigger his angina. This signifies progression of the stenosis of the coronary arteries. Silent ischemia refers to someone who has reversible heart injury that is NOT accompanied by paroxysmal chest pain. It is asymptomatic. Can occur in diabetics who have significant neuropathy. Atypical (Prinzmetal’s) angina occurs at rest. Most likely caused by spasm of coronary artery. 2. Myocardial infarction (MI)- Also covered well. An MI represents DEATH of heart muscle. More specifically, an area of heart muscle has undergone coagulative necrosis (re?) due to sudden, prolonged ischemia. If the zone of necrosis (death) is limited only to the innermost portion of the wall of the left ventricle (i.e. right next to the inner lining of the heart), then this is a subendocardial MI. If the necrosis involves the full thickness of the LV (from the interior to the exterior of the heart), then this is a transmural MI. 3. Congestive heart failure (CHF)- This is a CLASSIC complication of longstanding CAD. The heart muscle is being chronically hypoperfused and is therefor chronically ischemic. This leads to continual, low grade inflammation throughout the myocardium. Inevitably, multiple areas of the heart muscle will be destroyed and they will repair themselves by fibrosis (scarring). These scarred areas are non-functioning. Little by little, there is a decrease in the amount of heart muscle and an increase in the amount of scar tissue. This leads to a gradually increasing loss of pumping ability of the heart, i.e. (chronic) CHF. 4. Sudden death- due either to a huge MI (leads to acute CHF), or the sudden development of a fatal arrthymia. 5. Arrthymia- If the area of ischemia or infarct involves the conduction (“electrical”) system of the heart, any type of arrthymia can result, fatal or non-fatal. PAGE 2 Coronary artery anatomy- Anatomically, there are 2 coronary arteries. As noted above, both arteries have their origin directly off the aorta, directly above the aortic valve. 1. The right coronary artery (RCA) usually supplies blood/oxygen to the back (posterior) portion of the left ventricular (LV) wall, as well as to the posterior portion of the interventricular (IV) septum. (The IV septum is, of course, the muscle that separates the two ventricles). Thus, occlusion of the proximal portion of the RCA can lead to an MI in these areas. The RCA also supplies parts of the conduction system, namely the AV node and ventricular conduction system. So, occlusion can lead to arrthymias. 2. The left coronary artery (LCA) quickly bifurcates into two branches shortly after it leaves the aorta. Thus we have: a. Left main coronary artery- This represents the most proximal portion of the LCA, and runs from the aorta to the point of bifurcation. It is only about a half-inch long. b. Left anterior descending (LAD) branch of the LCA- This supplies blood to the front (anterior) portion of the LV wall, the anterior IV septum and the apex (tip) of the heart. It can also supply the AV node and ventricular conduction system. Sudden occlusion of the LAD can cause infarct to these areas, and can lead to arrhythmias. c. Left circumflex coronary artery (LCCA)- The other branch of the LCA. It brings blood to the lateral wall of the LV (i.e. the left-most side of the heart). Occlusion can lead to MI in this location. The LCCA also supplies the papillary muscles. These are the small muscles within the left ventricle to which the leaflets of the mitral valve are attached. If these muscles infarct, the mitral valve becomes incompetent, i.e. you develop mitral insufficiency (see Dr. O’Connor’s lecture on valve disease). This can be very grave indeed. Dr. O’Connor makes 4 points about coronary artery atherosclerosis: 1. The disease is worst in the proximal portions of the arteries (which run along the outer, i.e.epicardial, surface of the heart). The distal, smaller branches of the arteries (that lie within the heart muscle) are far less affected. 2. If atherosclerotic narrowing involves one branch of a coronary artery, you can bet that another branch(es) will also be narrowed. 3. The heart muscle can receive enough blood flow if the atherosclerotic narrowing of a coronary artery is no greater than 75%. Beyond 75%, the muscle becomes significantly ischemic/hypoxic (e.g. patient may experience ischemic chest pain). 4. Collateral circulation refers to branches of other, nonoccluded coronary arteries that may be able to supply blood to an ischemic area. Can help prevent, or limit the size of, an MI. PAGE 3 “Complications of Myocardial Infarction”- terms: 1. Pericardial tamponade- In some instances, an area of infarct may rupture, resulting in perforation of the LV wall. Blood will thus exit the heart and fill the pericardial sac (hemopericardium). This sac, which the heart lies within, is made of tough connective tissue so it is unable to expand in volume. Thus the blood will compress upon the heart and cause restriction of movement. The heart will be unable to pump blood. Cardiogenic shock can ensue. 2. Papillary muscle dysfunction/mitral insufficiency- See above discussion on LCCA. 3. Aneurysm of LV- Occurs when a large MI heals by scarring. The scarred portion of the LV wall is thin and flabby and, as such, will bulge out during systole when the pressure within the LV increases. This is an LV aneurysm. 4. Mural thrombus- The scarred remains of a healed MI is hypokinetic. It is incapable of contracting and beating. This inactive portion of the LV heart muscle is a setup for developing a superimposed thrombus on its inner surface. A portion of this mural thrombus can embolize (break off) and go anywhere in the body (except the lungs). If the mural thromboembolus travels to the brain, a stroke may occur. 5. Post infarction pericarditis- The inflammation that results from a transmural infarct can, by extension, involve the overlying pericardial sac. This pericarditis can cause adhesions between the heart and pericardial sac. This restricts the heart’s ability to pump and can lead to heart failure.