Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
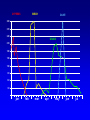
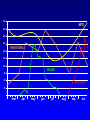
L’IMMUNOTERAPIA: ATTUALE Giovanni Passalacqua Allergy & Respiratory Diseases Dept.Internal MedicineUniversity of Genoa ITALY IMMUNOTERAPIA SPECIFICA (ITS) Somministrazione di estratti allergenici purificati (prima a dosi crescenti e poi a dose di mantenimento), al fine di ottenere la riduzione della risposta clinica all’allergene stesso. L’immunoterapia allergene specifica è un vaccino a tutti gli effetti La via tradizionale di somministrazione è quella iniettiva sottocutanea (SCIT), ad oggi affiancata anche dalla via sublinguale (SLIT) Leonard Noon 1877-1913 ISHIZAKA NOON UK CSM 1986 Randomized trials EMPIRICAL USE IgE 1928 2012 1960 ROMAGNANI Allergoids SLIT 1986 Mechanisms Th1/Th2 Peptides Recombinants WHO Pos Pap Liposomes Adjuvants 1990 1998 DURHAM DNAITS ILIT EPIT 2012 Rands DA. Anaphylactic reaction to desensitization for allergic rhinitis and astma Br Med J 1980; 281: 854 Frankland AW. Anaphylactic reaction to desensitization. Br Med J 1980; 281: 1429 Ewan PW. Anaphylactic reaction to desensitization. Br Med J 1980; 281: 1069 Committee on the safety of medicines (CMS) CMS Update Desensitizing vaccines Br Med J 1986; 293:948 26 fatalities since 1957 certainly due to IT 11 of them since 1980 Dal 1910 fino agli anni ’70: Prescrizione ingiustificata dell’ITS Prescrizione non corretta Pratica non adeguata, senza regole precauzionali e con estratti scadenti DUBBIA EFFICACIA E SCARSA SICUREZZA Desensitizing vaccines 26 deaths due to SCIT Committee on the Safety of Medicines BMJ 1986 Non-injection routes for immunotherapy ... the overall aim of improving safety of immunotherapy and making it more convenient for the patients... EAACI IT Position Paper 1993 WHO Pos Pap. Therapeutical vaccines for allergic diseases Allergy 1998 Standards for practical allergen-specific immunotherapy. Allergy 2006 Allergen immunotherapy: A practice parameter third update JACI 2011 L'ITS e' mirata invece all'allergene causale e non all'organo principalmente coinvolto.” L’ITS non è un trattamento di ultima scelta da usare se i farmaci falliscono, ma è complementare ad essi. L’ITS è efficace nelle allergie da -Inalanti (acari, pollini, alcuni funghi, epitelio di gatto) - Veleno di imenotteri RINITE SINTOMI SCIT - Meta-analysis: Symptom score RINITE FARMACI Calderon M et al 2007 Passalacqua G, Canonica GW. Clin Exp Allergy 2011 Cochrane 2010 MEDICATIONS BHR Cochrane 2010 SLIT: THE LITERATURE 75 RDBPC TRIALS 8 RANDOMIZED OPEN TRIALS 6 COMPARATIVE (SLIT vs SCIT) 5 TRIALS IN OTHER DISEASES 1st WAO pos pap (2009): 60 trials 2nd WAO pos pap (2013): 77 trials After 2013: 82 trials 9/22 big trials conducted in the USA ARIA Update on immunotherapy SR Durham and G.Passalacqua JACI 2007 SCIT SLIT Clinical efficacy: Rhinitis Ia Ia Clinical Efficacy: Asthma Ia Ia Clinical efficacy: Children (rhinitis) Children (asthma) Ib Ib Ia Ia Prevention of new sensitizations Ib IIa Longterm effect Ib IIa Prevention of asthma IIb IIb Indications Not costeffective? Mild intermitt. Mild Moderate- persistent severe intermitt. Moderatesevere persistent RHINITIS IMMUNOTHERAPY. ASTHMA HIGH RISK? Intermitt. Mild Moderate Severe Aspetti pratici. In Italia è formalmente un “named patient product” (preparato dalla ditta per ciascun paziente dietro indicazione), anche se ad oggi i vaccini per ITS vengono preparati su scala industriale, come i farmaci Gli estratti sono standardizzati (ossia è nota la quantità di allergene maggiore e la potenza) Si effettua una fase di graduale incremento del dosaggio (solitamente 1/sett per 2 mesi), seguita da una fase di mantenimento (1/mese). Per allergeni pollinici si può effettuare un trattamento prestagionale. Per allergeni perenni, il trattamento è continuativo. Durata consigliata 3-5 anni, da sospendere se dopo 2 anni non si ha beneficio. I fattori da valutare nella prescrizione dell’ITS 1 2 3 4 5 6 7 Il disturbo deve essere IgE - mediato (skin test o RAST positivi) L’allergene responsabile deve essere individuato con sicurezza Valutare la gravità e la durata dei sintomi l trattamento farmacologico é sufficientemente ben tollerato? Il paziente é in grado di affrontare l’ITS? (costi, impegno, stile di vita) È disponibile un vaccino standardizzato? L’efficacia del vaccino che si intende usare é dimostrata? CAUSAL ROLE OF THE ALLERGEN(S): Clinical history and exposure SKIN TESTING RAST ASSAY NASAL (CONJUNCTIVAL) CHALLENGE MOLECULAR DIAGNOSIS SLIT (IT in general) for the clinically relevant allergen(s) Preferably one, but in selected cases 2 or 3 extracts. BIRCH CYPRESS OLIVE 300 270 240 GRASS 210 180 150 120 90 60 30 jan feb mar apr may jun jul 300 MITE 270 240 210 PARIETARIA 180 150 120 GRASS 90 60 RAGWEED 30 mar apr may jun jul aug sep oct Vrtala S Allergy 2008 Verificare ed annotare la dose, l’ora e il sito di iniezione Visitare il paziente!!! Iniezione sottocutanea Aspirare per escludere di iniettare in un vaso Tempo di osservazione 30 minuti PREMEDICATION: PROS: Preventing reactions Avoiding severe reactions Diminishing reactions’intensity CONS: May mask symptoms’ onset May delay appropriate treatment INDUZIONE O BUILD-UP Flac 1 0.2 0.4 0.6 Flac 2 Flac 3 0.2 0.4 0.6 0.2 0.4 0.6 MANTENIMENTO 0.8 0.8 1 2 3 4 5 6 7 8 9 10 11 12 settimane 4 5 6 7 8 9 10 11 12 mesi NO BUILD UP 7/60 MAINTENANCE DAILY 31/60 MAINTENANCE 3/wk 20/60 MAINTENANCE 2/wk 7/60 MAINTENANCE 1/wk 2/60 POLLEN CONTINUOUS 8/43 POLLEN PRESEASONAL 3/43 POLLEN COSEASONAL 3/43 POLLEN PRECOSEASONAL 29/43 INIZIO: Prima della stagione di pollinazione (2 mesi) In qualsiasi momento per i perenni SCHEMA: Tradizionale, cluster, rush MANTENIMENTO: Prestagionale, precostagionale, continuo DURATA: Almeno 3-5 anni, poi se beneficio sospendere Se non beneficio dopo 2 anni sospendere VALUTAZIONE: Clinica (riduzione dei sintomi e dei farmaci) The optimal maintenance dose has been clearly identified (by dose-ranging studies) only for grass tablets. It is 15-25 mcg major allergen per day (30 times an equivalent SCIT course) Dose ranging studies are lacking for the remaining alllergens The efficacy has been anyway proven over a wide range of doses, and therfore the recommendation of the manufacturers should be followed. CONTRAINDICATIONS •Co-existent uncontrolled asthma (within the UK, presence of asthma is considered a relative contraindication). •Patients taking beta blockers •Patients with other medical/immunological disease •Small children (less than 5 years) •Pregnancy (maintenance injections may be continued during pregnancy) •Patients unable to comply with the immunotherapy protocol POSTPONE INJECTION IF: Concurrent ilness Asthma Exacerbation of allergy FATALITIES Lockey RF et al. JACI 1987 Period: 1945-1984 46 fatalities Reid MJ et al. JACI 1993 Period 1985-1989 17 fatalities FATALITIES: 1/2.000.000 injections RISK FACTORS Based on nonfatal reactions Uncontrolled asthma Severe asthma Use of betablockers Rush immunotherapy Use of new vials Technical errors Based on fatal reactions Uncontrolled asthma Severe asthma Use of betablockers Rush immunotherapy Build-up phase Use of new vials Technical errors Estimated incidence of fatalities < 1/2.000.000 injections The omission of the build-up phase seems not to increase the risk of adverse events. Build up is usually not done with the more recent tablet preparations Short build-up courses (1-5 days) can be applied, according to the manufacturer’s suggestion and to own experience COSA OCCORRE PER LA SCIT: Adrenalina (iniezione i.m.) Broncodilatatore short acting Steroide orale e i.v. Antistaminico orale e i.v. Set da infusione Ossigeno Ambu GRADING OF SYSTEMIC REACTIONS 1) Nonspecific reactions (likely non IgE-mediated) disomfort, nausea, headache, arthralgia 2) Mild systemic reactions mild rhinitis/asthma (PEF>60%) responding to b2 agonists/antihistamines 3) Non life-threatening systemic reactions Urticaria, angioedema, severe asthma (PEF<60%) Responding well to treatment 4) Anaphylaxis itching, urticaria, bronchospasm, with HYPOTENSION requiring intensive care Malling & Weeke, Allergy 1993 SLIT No fatal or near-fatal event reported since 1986 6 cases of anaphylaxis SLIT: KNOWN SIDE EFFECTS Local: oral itching-swelling stomach-ache nausea-vomiting Systemic: Urticaria/angioedema Rhinitis Asthma Anaphylaxis Relatively frequent. Usually self-resolve after the first doses without treatment. If persist reduce the dose. Rare. Give symptomatic treatment and reduce the dose. If persist, stop SLIT Exceptional. Treat properly and stop SLIT CONTRAINDICATIONS Systemic immunological diseases Immunodeficiecies Malignancies Cardiovascular diseases Severe/uncontrolled asthma Age < 5 years (relative contraindication) Modified from WHO 1998 Explain to patients the possible side effects Explain that side effects tend to disappear after few doses Suggest medications (e.g. oral antihistamines) to control local side effects if any Administer the first dose under medical supervision EFFETTI “SPECIALI” DELL’ITS Efficacia a lungo termine dopo la sospensione Prevenzione di nuove sensibilizzazioni Riduzione del rischio di insorgenza di asma Modificazione della risposta immunitaria AUTHOR (ref) ALLERGEN Mosbech (36) Grass Grammer (37) Ragweed Hedlin (38) PATIENTS DURATION SIT LONG-LASTING EFFECT 2.5 years 6 years 61 adult/children 4 months 2 years Cat/dog 32 adult/chidren 3 years 5 years Des Roches (39) Mite 40 adult 1-4 years 3 years Ariano (40) Parietaria 35 adult 4 years 4 years Durham (41) Grass 52 adult 3-4 years 3 years Eng (43) Grass 25 children 3 years 12 years Specific immunotherapy has long-term preventive effect of seasonal and perennial asthma: 10-year follow-up on the PAT study Jacobssen, Allergy 2007 PREVENTIVE EFFECTS OF SUBLINGUAL IMMUNOTHERAPY IN CHILDHOOD. AN OPEN RANDOMIZED CONTROLLED STUDY MAURIZIO MAROGNA MD1 , D.TOMASSETTI1, A. BERNASCONI1, F.COLOMBO1, ALESSANDRO MASSOLO BS2, A. DI RIENZO BUSINCO4, GIORGIO W CANONICA MD3, GIOVANNI PASSALACQUA MD3 AND SALVATORE TRIPODI MD4 1 3 Pneumology Unit, Cuasso al Monte, Macchi Hospital Foundation, Varese 2 Department of Animal Biology, University of Pavia, Pavia Allergy & Respiratory Diseases,Department of Internal Medicine, Genoa University 4 Pediatric Allergy Unit, S. Pertini Hospital, Rome AAAI 2008, 101: 261 MONOSENSITIZED PATIENTS 70 70 60 60 *** 50 40 % PATIENTS % PATIENTS PERSISTENT ASTHMA *** 30 *** *** 50 40 30 20 20 NS 10 10 baseline CONTROLS 3rd year baseline 3rd year SLIT FARMACI Azione rapida Effetto preventivo NO SI NO SI Effetti collaterali SI Costo BASSO Lunga durata SIT NO NO ALTO SI CONSENSO NELLA PRATICA ALLERGOLOGICA Immunoterapia ITS per via sottocutanea Consenso scritto! Informazione? ITS per vie non iniettive (sub-linguale) Consenso? CONCLUSIONI Farmacoterapia e immunoterapia hanno meccanismi diversi Il loro effetto è additivo L’ITS consente un risparmio di farmaci sintomatici L’ITS ha effetti preventivi e a lungo termine che i farmaci non hanno L’ITS agisce contemporaneamente su naso e bronchi FARMACI E ITS NON SONO MUTUAMENTE ESCLUSIVI