Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
ICU Pain Management
Bryan Sloane
June 2009
Pain Management
• Managing pain is especially important in critically
ill and trauma patients. Pain form an injury or
illness can increase blood pressure, heart rate, and
increase blood glucose; all of which can lead to
serious complications.
• Definition: Analgesic is a pain killer derives from
Greek an- ("without") and algos ("pain")
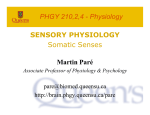
How is pain measured?
• A visual analog scale is used for conscious
patients. The patient chooses a number
between 1 and 10 for the amount of pain
they are having, with 1 being the lowest
amount of pain and 10 being the highest.
Pain Assessment cont.
• Pain is measured for unconscious patients
by observing their level of agitation and
movement. Vial signs can also be an
indication of pain levels if they exceed the
patients baseline vitals for their
injury/illness.
How is pain controlled
• Medications like Analgesics,
antidepressants, and antiseizue medications.
• Acupuncture, Placebo, other alternative
practices
• Transcutaneous Electrical Nerve
Stimulation (TENS)
• Surgery, Physical and aquatic therapy,
Psychological support
How pain works
• Nociceptor Receptors in the skin and
internal organs are sensitive to painful
stimuli. The receptors are free nerve
endings connected to small diameter
myelinated A nerve fibers and unmyelinated
C nerve fibers. When these receptors are
activated, they send a signal to the spinal
cord that is processed as pain.
Gate Control Theory
• Patrick Wall and Ronald Melzack in 1965
• pain is a function of the balance between the
information traveling into the spinal cord through
large nerve fibers and information traveling into
the spinal cord through small nerve fibers
• Large nerve fibers carry non-nociceptive
information and small nerve fibers carry
nociceptive information. If the relative amount of
activity is greater in large nerve fibers, there
should be little or no pain. However, if there is
more activity in small nerve fibers, then there will
be pain.
Analgesic Medications
• Most common are Non-steroidal antiinflammatory (NSAIDS)
– inhibit cyclooxygenases, leading to a decrease
in prostaglandin production. This reduces pain
and also inflammation
• Opiates and morphinomimetics
– Morphine, the standard of Opiate Pain Control
Morphine
• Main effect is binding to and activating µopioid receptors in the Brain
• Increase Dopamine production in neurons in
the ventral tegmental area (VTA), which
project to the nucleus accumbens (NA)
• Very addictive, similar in molecular
structure to Heroin
• Molecular Similarities between Morphine and
Heroin
• Only difference is acetyl groups (Rx Drug on
Left, illegal drug on right)
Fentanyl
• potency is approximately 81 times that of
morphine
• Works via the same pathway
• Both can be delivered by Patient Controlled
Analgesia (PCA) when patient awake and
alert. PCA consists of a self-activating
infusion pump programmed to deliver a set
number of pain medication in an hour.
Alternative Therapy
• Acupuncture
• 1. Stimulation of large diameter nerve fibers that
inhibit pain
• 2. Could be placebo effect. Causes release of
endorphins
• 3. Some types of acupuncture may stimulate small
diameter nerve fibers and inhibit spinal cord pain
mechanisms (opposite of gate theory)
Other Therapies
• Hypnosis
– 1. May activate the pain-inhibitory pathway from the
brain to the spinal cord (not opiate pathway)
– 2. May act somewhere in the brain to shift a patient's
attention away from the pain.
• PT
– relieve pressure/compression on nerves/tissue through
movement
• Nitric Oxide Gas (NO)
– Laughing gas, administered with oxygen, has potential in
prehospital use, already used in other countries.
Sources
• Chudler, Eric. "Pain." Neruoscience. Jan.
2009. Washington University. 8 June 2009.
• Erdek, Michael, and Peter Pronovost.
"Improving assessment and treatment of
pain in the critically ill." Journal for Quality
in Healthcare 16 (2004): 59-64.
• Drugs.com