Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
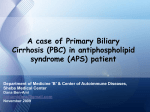
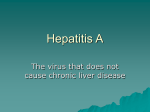
CHOLESTASIS Dr Allister Grant Consultant Hepatologist 7.2.12 Cholestasis • Cholestasis is an impairment of bile formation and/or bile flow • Symptoms of fatigue, pruritus and in its most overt form, jaundice. • Early biochemical markers in often asymptomatic patients – increases in serum alkaline phosphatase (ALP) – γ -glutamyltranspeptidase (γGT) – Conjugated hyperbilirubinaemia at more advanced stages. • Cholestasis – classified as intra-hepatic or extra-hepatic. Chronic Cholestasis • >6mo • Most chronic cholestasis is intra-hepatic • Asymptomatic patients are usually picked up by routine blood tests • ALP iso-enzymes • γGT is too sensitive and not specific for liver disease -Glutamyl transpeptidase • The high sensitivity and very low specificity seriously hampers the usefulness of this test • If ALP is elevated and GGT is elevated then the raise in ALP is likely to be hepatic in origin • Elevated in – – – – – a whole host of liver diseases Drugs/Alcohol Obesity/ dyslipidaemia/ DM CCF Kidney, Pancreas, Prostate Investigation of Cholestasis Raised ALP Check GT if isolated rise Dilated bile ducts 1) Stop alcohol 2) Stop hepatotoxic drugs 3) Advise weight loss if BMI>25 Non-dilated bile ducts 4) Recheck LFT’s after an interval Persistently raised ALP Ultrasound + Full liver screen Consider MRCP ERCP Other imaging Diagnosis madeTreat disease Non diagnostic Ixconsider Liver biopsy Hepatocellular cholestasis Cholangiocellular cholestasis • • • • • • • • • • • • • • • • • • • • Sepsis-, endotoxaemia-induced cholestasis Cholestatic variety of viral hepatitis Alcoholic or non-alcoholic steatohepatitis Drug- or parenteral nutrition-induced cholestasis Genetic disorders: e.g., BRIC, PFIC, ABCB4 deficiency Intra-hepatic cholestasis of pregnancy (ICP) Erythropoietic protoporphyria Malignant infiltrating disorders: e.g., hematologic diseases, metastatic cancer Benign infiltrating disorders: e.g., amyloidosis, sarcoidosis hepatitis and other granulomatoses, storage diseases Paraneoplastic syndromes: e.g., Hodgkin disease, renal carcinoma Ductal plate malformations: e.g., congenital hepatic fibrosis Nodular regenerative hyperplasia Vascular disorders: e.g., Budd–Chiari syndrome, veno-occlusive disease, congestive hepatopathy Cirrhosis (any cause) • • • • • Primary biliary cirrhosis (AMA+/AMA-) Primary sclerosing cholangitis Overlap syndromes of PBC and PSC with AIH IgG4-associated cholangitis Idiopathic adulthood ductopenia Ductal plate malformations: biliary hamartoma, Caroli syndrome Cystic fibrosis Drug-induced cholangiopathy Graft vs. host disease Secondary sclerosing cholangitis: e.g., due to various forms of cholangiolithiasis, ischemic choangiopathies (hereditary haemorragic telangiectasia, polyarteritis nodosa and other forms of vasculitis), infectious cholangitis related to AIDS and other forms of immunodepression, etc. Drug Induced Cholestasis • Intrahepatic Hepatocellular Cholestasis • Intrahepatic Cholangiocellular Cholestasis • Ductopenic • Granulomatous • Allopurinol Antithyroid agents Augmentin Azathioprine Barbiturates Captopril Carbamezepine Chlorpromazine Chlorpropamide Clindamycin Clofibrate Diltiazem Erythromycin Flucloxacillin Isoniazid Lisinopril Methyltestosterone Oral contraceptives (containing estrogens) Oral hypoglycemics Phenytoin Trimethoprim-sulfamethoxazole Mr S • 62yr old • 25 yr history of UC/PSC • Limited details due to frequent movement around the country Mr S • 1990’s Seen at Royal Free- ?Listed for OLTx and then removed from list • Ampullary stenosis 1994 • Recurrent pancreatitis • Recurrent cholangitis • 1998 ERCP lower CBD narrow, no dominant strictures Mr S • 2000 Inverness- Recurrent cholangitis, short attacks • Ciprofloxacin (PRN at home) • 2003 Seen in Hemel Hempstead- cholangitis, ERCP’s • Severe post –ERCP pancreatitis Mr S • Leicester Aug 2003 • Gastro referral from GP 2004 • “Feels bad most weeks” • Has a cocktail of Ciprofloxacin, Hyoscine, Pethidine, DHC to take when feels bad Mr S • Had been having colonoscopic surveillance, but not for 2 years • Ex Smoker • Appendicectomy, Depression • Olsalazine 500mg bd, Omeprazole 10mg od UDCA 150mg tds FeSO4 Mr S • OPD Nov • Hx of severe post ERCP pancreatitis obtained • LFT's persistently ALP 400-700 • Referred to Hepatology • Advised rotating ABx Mr S • What next? Mr S • USS- CBD stone, IHD’s mildly dilated Thickened ducts • MRCP Mr S Mr S Mr S • What next? Mr S • Dec 04 Admitted with jaundice and fever • Had not started Abx • WCC 19, Bili 52, ALP 614 • Enterococcus species • ERCP Mr S Mr S Mr S • Post ERCP ALP >1000 • Gradually settled • URSO increased to 500mg tds (65kg) • Started rotating ABx Mr S • Free of cholangitic episodes for 18 mo • Occasional fleeting pain • ALP 600, Bili 22 Primary Sclerosing Cholangitis Definition A chronic inflammatory cholestatic disease Progressive destruction of bile ducts May progress to cirrhosis Aetiology unknown Relationship to IBD • IBD in 60-80% of PSC patients • UC more common than Crohn’s (2:1) • PSC in Crohn’s disease almost always involves the colon • 2-10% of UC patients have PSC Survival in PSC Compared to Olmsted County 1.0 Survival Control population PSC (no transplant) 0 0 5 10 15 Follow up (Years) Bamba K et al Gastro 2003 20 Cholangiocarcinoma • Lifetime prevalence of 10-30% • Annual risk 1.5% per year • Difficult to diagnose • Patients also have late risk of HCC PSC and Bowel Cancer • 25% PSC develop cancer or dysplasia cf 5.6% with UC alone • Cancers associated with PSC tend to be more proximal, are more advanced at diagnosis and more likely to be fatal • Need yearly colonoscopic surveillance Recurrence of PSC Post Transplant Alexander J et al Liver transplantation 2008 PSC Clinical Presentation • Asymptomatic 15-44% • Symptomatic • • • • • • • • • • • Fatigue Pruritus Jaundice Hepatomegaly Abdominal Pain Weight Loss Splenomegaly Ascending cholangitis Hyperpigmentation Variceal Bleeding Ascites 75 70 30-69 34-62 16-37 10-34 30 5-28 25 2-14 2-10 Diagnosis • Cholangiography – either MRCP or ERCP – multifocal strictures and dilatation usually affects both intra and extrahepatic ducts • Clinical,biochemical and histological features PSC Diagnostic Criteria • Exclude – HIV cholangiopathy – Cholangiocarcinoma – Biliary tract surgery or trauma – Choledocholithiasis – Congenital abnormalities – Ischaemic cholangiopathy – Stricturing due to TACE PSC • Prevalence of auto-antibodies in PSC • P-ANCA 80% • AMA <2% • ANA 50-60% • SMA 35% p-ANCA is not specific for PSC • PSC 80% • UC 75% • AIH 80% • PBC 30% Cholangiography Role of Liver Biopsy in PSC • Can help to confirm diagnosis • May help to exclude an overlap syndrome • If cholangiogram is normal then may help to exclude small duct PSC • For staging and prognostication • Not always needed Small Duct PSC • 5% of PSC • Normal cholangiogram but biopsy showing PSC • Can progress to classical PSC (12%) • May exist with or without UC Probability of Survival Survival curves for patients with small duct and large duct PSC (p<0.05) Months since diagnosis Björnsson E et al. Gut 2002;51:731-735 Primary Biliary Cirrhosis PBC Epidemiology • Female:male ratio of 9:1 • Most common during middle age • Presentation similar between genders, races, and sexes • Prevalence: 19-150 cases/million • Incidence: 4-15 cases/million/yr • Incidence/prevalence rates increasing? • Familial clustering Kaplan et al. NEJM 2005;353(12):1261 PBC-Asymptomatic Disease • 50-60% of patients (earlier diagnosis) • 36-89% of asymptomatic patients develop symptoms within 4.5-17 years • Elevated AMA (M2) • Liver biopsy • Liver chemistry tests – Normal – Cholestatic • 50-70% 10 year survival in asymptomatic patients • UDCA associated with better survival when compared to preUDCA era Balasubramaniam et al. Gastroenterology 1990;98(6):1567 PBC Symptomatic Disease • • • • • • Fatigue (common) Pruritus Jaundice Hepatosplenomegaly RUQ pain Hyperpigmentation Koulentaki et al. Am J Gastroenterol 2006;101(3):541 • Xanthomas and xanthelasmas • Dyslipidemia • Extrahepatic autoimmune diseases • Complications – Portal hypertension – Chronic cholestasis PBC Complications • Chronic cholestasis – Loss of bone density – Malabsorption – Steatorrhea • Bile salt deficiency • Pancreatic disease • Coeliac disease – Vitamin A, D, E, K deficiency • Portal hypertension – Oesophageal and gastric varices – Ascites – Encephalopathy – SBP – HRS or HPS – Hepatocellular carcinoma PBC Metabolic Bone Disease • 30-50% of patients • Classification – Osteoporosis: common – Osteomalacia: rare • Diagnosis and F/U – DEXA scan – Every 2-3 yrs • Management – Calcium and vitamin D – Adequate exercise – Oestrogen replacement • Post menopausal – Other medications • Bisphosphonates • Strontium Ranelate – Transplantation • Progressive disease PBC Metabolic Bone Disease Compression fractures PBC Hypercholesterolemia • • • • • Elevated cholesterol: 85% of patients Stage I or II disease: increased HDL predominates Stage III or IV disease: increased LDL No increased risk for ischemic heart disease Lipid-lowering drugs not recommended unless there is a separate lipid disorder • Plasmapheresis for xanthomatous neuropathy and symptomatic planar xanthomas PBC Dyslipidemia Xanthelasmas Xanthomas Xanthomas Xanthomas PBC Associated Diseases • Thyroid disease – Hashimoto’s thyroiditis – Grave’s disease • • • • • • Scleroderma CREST syndrome Sjogren’s syndrome Arthritis Raynaud’s phenomenon Coeliac disease • Renal tubular acidosis – Proximal – Distal • Gallstones • Haematologic disorders • Inflammatory bowel disease (rare) • Pulmonary interstitial fibrosis (rare) PBC Non-Invasive Tests • Biochemical tests – – – – – – – – – Alkaline phosphatase γGT 5’ nucleotidase AST and ALT Bilirubin Total cholesterol Serum IgM Prothrombin time Albumin Dickson et al. Hepatology 1989;10(1):1 Muratori et al. Clin Liver Dis 2008;12(2):261 Kaplan et al. N Engl J Med 2005;353(12):1261 • Serology – – – – – AMA (95%) ANA (50%) SMA (50%) Anti-centromere Anti-thyroid • Medical imaging – Ultrasound – CT – MR or MRCP PBC Histology • Stage I (portal) – Inflammation of interlobular and septal bile ducts – Granulomatous (florid duct) lesion • Stage II (periportal) – Inflammation of interlobular and septal bile ducts – Ductular proliferation Scheuer et al. Mayo Clin Proc 1998;73(2):179 • Stage III (septal) – Inflammation of interlobular and septal bile ducts – Fibrosis – Bile duct loss – Cholestasis • Stage IV (cirrhotic) – Established cirrhosis PBC Pathology Cirrhosis NRH PBC Overall Management • Survival of patients with PBC inferior to that of a healthy control population • Medical treatment warranted in all patients • No medical therapy has been shown to conclusively alter the history of PBC • Goals of treatment – Slow disease progression – Treat complications PBC Medical Management • Ineffective – – – – – – Corticosteroids Azathioprine Cyclosporine Penicillamine Colchicine Chlorambucil • Possibly effective – Methotrexate – Mycophenolate mofetil • Effective – Ursodeoxycholic acid • Improvement in symptoms • Improvement in LFTs • Improvement in histology • Improvement in transplant free survival PBC-UDCA • Effective dose: 13-15 mg/kg/day indefinitely • Mechanism of action – – – – – Promotes endogenous bile acid secretion Replacement of hepatotoxic (endogenous) bile acids Stabilizes biliary epithelial cell membranes Alters HLA I-II expression on biliary epithelial cell Inhibits biliary cell apoptosis • Improvement in LFTs • Delays disease progression and improves transplant-free survival • Follow LFTs every 3-6 mo. Poupon et al. N Engl J Med. 1994;330(19):1342 Heathcote et al. Hepatology 1994;19(5):1149 PBC Incomplete Responders to UDCA • 66% of patients • Definition – Failure to normalize LFTs – Development of cirrhosis on therapy • Predictors of incomplete response – High alkaline phosphatase or GGT – Advanced disease prior to UDCA initiation • Assess: patient compliance, UDCA dose, overlap syndrome Combes et al. Hepatology 1995;22(3):759 Poupon et al. J Hepatolol 2003;39(1):12 PBC Liver Transplantation • Patient and graft survival – 1 yr : 83-92% – 5 yr : 75-85% • Higher risk of rejection • PBC recurrence – – – – – – 15 to 25% of patients at 10 years Granulomatous bile duct injury AMA does not define recurrence Exclude other post transplant disorders Intermediate term patient and graft survival are good Use of UDCA for recurrent disease uncertain Liermann et al. Hepatology 2001;33(1):22 PBC Pruritus • Antihistamines – 50% response rate • Cholestyramine – 90% response rate • UDCA – Inconsistent results • Rifampin – Rapid onset of action – Can cause liver injury • Other medications – Opiate antagonists – Sertraline – Ondansetron? • Other – Extracorporeal support – OLT PBC Vitamin Deficiency • Vitamin A – – – – 20% of patients Night blindness Replace as appropriate Can cause liver injury • Vitamin D – Replace as appropriate – Can cause liver injury – Supplemental calcium • Vitamin E – Rarely seen in adults – Neurologic sequelae • Reduced proprioception • Ataxia – Replace as appropriate • Vitamin K – Risk of hemorrhage – Replace as appropriate Natural History and Prognosis • PBC progresses over 15-20 yrs • Median survival – Asymptomatic disease: 10-16 yrs – Symptomatic disease: 7.5-10 yrs – Bilirubin (80μg/L): 2 yrs PBC Summary • Important cause of chronic cholestatic liver disease • Middle-aged females predominate • Immune pathogenesis favored • Other autoimmune diseases frequently coexist • PBC progresses in most patients PBC Summary • Complications of portal hypertension and chronic cholestasis associated with progressive disease • UDCA is standard medical therapy for all patients • Transplantation reserved for patients with marginal liver reserve and complications Primary Biliary Cirrhosis (PBC) Age Gender Assoc’d Dx vs. Primary Sclerosing Cholangitis (PSC) 40-60 10-30 Female Male RA, CREST Scleroderma Ulcerative Colitis Crohn’s Disease Sjogren’s Primary Biliary Cirrhosis (PBC) Age Gender Assoc’d Dx vs. Primary Sclerosing Cholangitis (PSC) 40-60 10-30 Female Male RA, CREST Scleroderma, Sjogren’s Ulcerative Colitis Crohn’s Disease Primary Biliary Cirrhosis (PBC) Age Gender Assoc’d Dx vs. Primary Sclerosing Cholangitis (PSC) 40-60 10-30 Female Male RA, CREST Scleroderma, Sjogren’s Ulcerative Colitis Crohn’s Disease Primary Biliary Cirrhosis (PBC) Age Gender Assoc’d Dx vs. Primary Sclerosing Cholangitis (PSC) 40-60 10-30 Female Male RA, CREST Scleroderma, Sjogren’s Ulcerative Colitis Crohn’s Disease Ducts Affected Small to medium All ducts Primary Biliary Cirrhosis (PBC) Age Gender Assoc’d Dx 40-60 10-30 Female Male RA, CREST Scleroderma, Sjogren’s Ulcerative Colitis Crohn’s Disease Ducts Affected Small to medium Method of Dx vs. Primary Sclerosing Cholangitis (PSC) ?Biopsy All ducts MRCP/ERCP Mr Y • 53 year old married man presented at GGH -end Aug 09 • Chest Pain/Abdo pain and loose stools • Troponin negative • Abnormal LFT’s ALT 212 ALP 522 Bili 21 ALB 37 Amylase 33 Initial liver screen • IgG slightly elevated • IgM slightly elevated • • • • Caeruloplasmin A1AT level Ferritin TFT Imaging • USS– echogenic mass in left lobe -5x4x2cm – Probably complex haemangioma- some doppler flow and some other small similar lesions By week later ALP>1000 Transferred to Liver Unit • • • • • • HBsAg neg HCV ab neg EBV IgG pos CMV neg Autoantibodies neg Tumour markers neg • CT – Multiple haemangiomata – Multiple enlarged nodes at porta 12mm – ? SB polyp – RMZ consolidation Rash on palms and soles biopsied 9/9/09- non specific Liver biopsy arranged and done 17/9/08periductal fibrosis and biliary inflammation • VDRL/TPHA Positive • Commenced on penicillin • Referred to GUM • LFT’s completely normalised in 2 months Suggested reading