Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
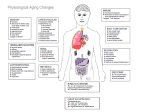
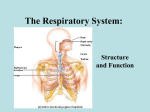
Respiratory Toxicology Michael S. Morgan University of Washington Email: [email protected] Respiratory System Functional anatomy Head airways (upper respiratory passages): nose, mouth, throat, bounded by vocal cords Tracheobronchial tree: trachea, bronchi, bronchioles; site of narrowing in asthma, bronchitis, emphysema Gas Exchange (pulmonary) region: alveoli, alveolar ducts, respiratory bronchioles; the acinus consists of one respiratory bronchiole plus all alveoli distal to it; primary site of gas exchange; site of damage in fibrosis, pneumonia, edema. Respiratory function Primary: Gas exchange - oxygen, carbon dioxide, water vapor Secondary: Communication Biotransformation of some hormones, drugs, and pollutants Defense against infection and entry of airborne toxicants Cardiovascular system A key partner in accomplishing gas exchange: Primary distribution system for metabolic gases, nutrients, absorbed agents Heart, blood vessels, blood (role of hemoglobin) Evaluation: heart rate, blood pressure, electrocardiogram, exercise stress test, angiography, chemical markers of muscle damage Respiratory system factors Major route of entry - surface area = 50-100 m2 Barrier thickness = 1 µm on average Affected by many hazardous materials Under neurologic and chemical (O2, CO2, pH) control Hypoventilation - underbreathing, relative to metabolic need Hypoxia - too little oxygen in air Evaluation: pulmonary function tests, eg spirometry; chest X-ray and CT imaging, allergen challenge, bronchoalveolar lavage (evaluation of harvested cells), NO production (marker of inflammation) Quantitative Aspects Ventilation and oxygen uptake: For a 70 kg person at rest, the flow rate of air in and out is 7.5 L/min, or 450 L/hour; the flow rate of oxygen into the blood is 21.5 g/hour During 30 minutes of aerobic exercise by the same person, the flow rate of air is 45 L/min, and amount of oxygen taken in is 85.7 g. In a 24 hour day, for the same person, the volume of air inhaled and exhaled is, on average, 15,000 L. Accomplishing this requires lungs that are flexible, with a thin membrane between air and blood, and airways that are have minimal obstruction. Inhalation Dosimetry Using the flow rates given: If the average PM10 concentration is 100 µg/m3, then the mass inhaled is 1.5 mg dust/day/70 kg body weight [100 µg/m3 x 15 m3 /day = 1.5 mg dust] If the ozone concentration is 0.1 ppm for three hours during the AM, and the rate of ventilation during this period is 10 L/min (light exercise) then the mass inhaled and deposited on the respiratory surfaces is 0.36 mg/day. (0.1 ppm ozone = 0.2 mg/m3) [0.2 mg/ m3 x 180 min x .010 m3/min = 0.36 mg] Deposition of Inhaled Agents Particle aerodynamic diameter D>10 µm: deposition in head, especially with nose-breathing D<10 µm: increasing penetration to tracheobronchial and gas exchange regions; minimum in deposition for D ≈ 0.5 µm Gas or vapor solubility in mucus and blood SO2: head deposition O3: distal airway and alveolar deposition Breathing pattern and pathway (nose v mouth) Increasing flow rate enhances deposition via impaction in head and larger tracheobronchial airways; decreasing flow rate enhances deposition by diffusion and settling in alveolar spaces. Clearance of Deposited Agents Cough, sneeze Head and larger tracheobronchial airways; very rapid Mucociliary system Mucus blanket propelled toward mouth by ciliated epithelial cells Clears head and all airways in tracheobronchial region Speed decreases with depth in respiratory system; slowest clearance may require 24 hours Alveolar macrophages Surface resident cells in alveoli; ingest deposited particles, carry them to mucociliary blanket; >24 hours. May result in gastrointestinal absorption Respiratory Responses to Exposure Altered secretions - reduction in airway diameter, slowed clearance: chemical irritants Airway constriction - reduction in airway diameter, coughing; chemical irritants, allergens Slowed clearance - reduced ciliary action, impaired macrophage activity: irritants, cytotoxic agents Cell damage - increased membrane permeability to fluids, loss of surface area, decreased lung expansion; corrosive agents Neoplasia - uncontrolled cell growth, invasion of neighboring tissue, airway narrowing, decreased lung expansion: carcinogens Classification of Respiratory Disease 1. Obstructive: narrowing of airways at one or more locations causes reduced air flow or increased work of breathing. Chronic bronchitis, emphysema, asthma, reactive airway disease 2. Restrictive: stiffening of the flexible tissue of the lungs causes reduced lung volume, reduced air flow or increased work of breathing, thickened membranes. Fibrosis, cancer, pneumonia, tuberculosis 3. Vascular: changes in mechanical properties of blood vessels causes increased blood pressure, fluid leakage. Pulmonary edema, heart failure 4. Regulatory: failure of control system, hypoventilation. Respiratory Disease Identification Relationship to environmental and occupational causes Influence of tobacco smoke Spirometry is principal surveillance tool Exposure and occupational histories are critical Effects of Environmental Agents Asthma - pollen, irritant chemicals Chronic Bronchitis - cigarette smoke Retarded Growth of the Respiratory System in Children ozone, oxides of nitrogen Elevated Frequency of Respiratory Infections - ozone, particulate matter Aggravation of Existing Respiratory or Cardiovascular Disease - carbon monoxide, fine/ultrafine particles, sulfate Cancer - cigarette smoke Asphyxiation - gases that displace oxygen: CO2 Occupational Lung Diseases Pneumoconioses - dust in the lungs, fibrosis (scarring, stiffening) generally present Coal workers (CWP) - simple or progressive Silicosis - may be associated with tuberculosis, cancer Shaver’s disease - bauxite Berylliosis - immune system is involved Siderosis - iron; often considered benign Stannosis - tin Asbestosis - may be associated with cancer Occupational Lung Diseases Industrial Bronchitis - chemical irritants Occupational Asthma Allergic response, may be delayed (ca. 12 hours) Wheeze, cough, shortness of breath Agents: animal dander, colophony, isocyanates, grain and wood dusts, anhydrides and phthalates, platinum compounds Byssinosis - cotton processing Endotoxin in bacterial contaminant suspected Hypersensitivity pneumonitis - mold, fungi Occupational Lung Diseases Cancer Bronchogenic cancer: initial site in airway; asbestos, ionizing radiation, coke oven emissions, nickel carbonyl; strong synergism between asbestos and tobacco smoke Mesothelioma: initial site is in visceral pleura (outer lining of lungs); few causes other than asbestos Asphyxiation - interference with oxygen uptake, delivery or utilization Simple - displacement of oxygen by inert gas, eg methane, nitrogen, acetylene Chemical - carbon monoxide, cyanides: interfere with oxygen transport or cellular respiration