Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
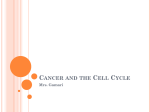
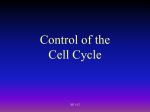
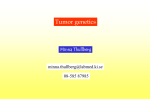
UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells The effect of hyperbaric oxygen on human oral cancer cells. T.B. SUN1, R.L. CHEN2, Y.H. HSU3 1 Division of Plastic Surgery and Center for Hyperbaric Oxygen Therapy; 2Center for Bone Marrow Transplantation; Department of Pathology, Tzu Chi Medical Center and Institute of Medical Sciences, Tzu Chi University, Hualien, Taiwan. 3 Sun T.B., Chen R.L., Hsu, Y.H., The effect of hyperbaric oxygen on human oral cancer cells. Undersea Hyperb Med 2004, 31(2):255-264. Discoveries of the beneficial cellular and biochemical effects have strengthened the rationale for the administration of hyperbaric oxygen therapy (HBO2) as an adjunctive therapy for the treatment of osteoradionecrosis (ORN). Malignancies, however, are considered a contraindication for HBO2 because of the possible tumor-promoting effects. The aim of this study was to examine the effects of HBO2 therapy on tumor weight, and to measure the progression of apoptosis and tumor cell proliferating activity in a cultured human oral cancer cell line. Twenty 5-week-old male NODscid mice underwent daily HBO2 of 2.5 atm abs, 90 minutes for 20 treatments. The control group, n = 20, did not undergo HBO2 and tumor weight, apoptosis index, and proliferating activity parameters were compared between the two groups. The results showed no significant differences (p < 0.05) in the whole-body weights, tumor weights, apoptotic index or proliferating activity index between the two groups. By using the apoptosis and proliferating activity assays which were better indicators of tumor cell growth than tumor weight alone, our results suggest that the clinical application of HBO2 does not promote the growth or proliferation of human oral cancer cells. INTRODUCTION Hyperbaric oxygen therapy (HBO2) is presently one of the most effective adjunctive treatments for osteoradionecrosis (ORN) (1-4). By increasing tissue oxygenation and neovascularization, HBO2 promotes wound healing in irradiated tissues. Recent discoveries of beneficial cellular biochemical effects have further strengthened the rationale for the clinical application of HBO2 (5-10). However, concomitant malignancy has been recognized as a contraindication to HBO2 because of possible growth enhancing effects to the tumor cells (11, 12). For patients with mandibular radionecrosis the most common scenario is that they undergo surgery and radiotherapy to eliminate the cancer cells. After radiotherapy, soft tissue breakdown and mandible erosion may develop. It is well known that HBO2 is helpful for patients with wounds in radiated tissue but concern for residual and recurrent disease has made the timing of HBO2 uncertain. The question of whether to use HBO2 in patients with ORN when there are concerns about oral cancer is important. The purpose of this study was to determine whether the cancer promoting effects of HBO2 occur in human oral cancer cells. It has been suggested that possible cancer growth enhancing effects of HBO2 could be categorized by tumor nourishment, immune suppression, and free radical-mediated toxicity (11). The traditional ways of evaluating tumor growth include measuring the weights and/or the volumes of the tumors (13-15). Recently, two more sensitive approaches, apoptosis and proliferating cell nuclear antigen (PCNA) assays, have been applied in oncology studies (16-20). We used both approaches along with the traditional tumor weight measurements to follow tumor progression and aspects of tumor nourishment and toxicity during the application of HBO2. Copyright © 2004 Undersea and Hyperbaric Medical Society, Inc. 251 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells METHODS Animals Forty male non-obese diabetic/severe combined immune-deficient (NODscid) mice at 5 weeks old were used in this study. The immune competence of NODscid mice is decreased due to poor T cell, B cell, and natural killer cell activity that allows human xenografts to be transplanted successfully (21). Since NODscid mice are more immune-deficient than nude athymic mice, a new trend in live culture media has developed for research (22). The mice were housed at the Laboratory Animal Center of the Tzu Chi University, Taiwan. The Ethics Committee for Animal Experimentation of the Tzu Chi University and Hospital approved the experimental protocols. Cell Cultures An oral cancer cell line, CRL-1623, derived from human squamous cell carcinoma of the tongue was provided by the American Type Culture Collection (ATCC). The tumorigenecity of CRL-1623 is very high, it is not too demanding to maintain and subculture this cell line (23, 24), and the 40kD keratin filament by-product may be used as an indicator to verify its squamous cell origin (25). The cell line was propagated in a mixture of 45% Dulbecco's modified Eagle's medium, 45% Ham's F12 medium, 10% fetal bovine serum, and 400 ng/ml hydrocortisone in a 75 cm cell culture flask and incubated in saturated humidity at 37 °C and 5% CO2 in air. The complete culture medium was changed every 3 to 4 days. The cells were subcultured with 0.25% trypsin, 0.03% ethylenediamine tetraacetic acid (EDTA) solution after an adherent monolayer was formed in the flask (Figure 1). Fig. 1. Representative view of the adherent monolayer of the CRL-1623 human tongue squamous cell carcinoma cell line in a 75 cm2 culture flask. (400X magnification). The cells were harvested after eight culture passages. Unit doses of 0.15 ml containing 106 single cell suspensions were prepared for subsequent inoculations of immunocompromized experimental animals. In vivo Tumor Xenografts The NODscid mice were divided into to two groups randomly and raised in sterilized cages with a density of five mice per cage. Each animal had access to sterile water and food ad libitum. A 12-hour light and 12-hour dark cycle was performed automatically. The cultured cancer cells, 106 cells in 0.15 ml phosphate buffered saline, were inoculated into the back of each 252 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells mouse subcutaneously. treatment. All 40 mice were allowed to recover for 72 hours before HBO2 Hyperbaric Oxygen Treatment A SIGMA-34 monoplace hyperbaric chamber (Perry Baromedical Corporation, Fla., USA) was used for this study. The study group, n = 20, received daily HBO2 from 10:20 a.m. to 12:20 p.m. Monday through Friday. The compression was started after 10 minutes of rest and 2.5 atm abs was reached within 10 minutes. During the treatment, the animals breathed the chamber atmosphere, which was 100% O2. The pressure was kept at 2.5 atm abs for 90 minutes. For decompression, the pressure was decreased 0.1 atm abs min-1 until 1 atm abs was reached. Each animal underwent 20 treatments and all were completed smoothly without adverse effects. The control group, n = 20, experienced the same transportation procedure simultaneously and were treated with air at 1.0 atm abs. Tumor Evaluations After completion of the HBO2 treatments, the animals were euthanized with CO2. Surgical dissections of the tumors were performed immediately after death (Fig. 2). An electronic scale was used to measure the weight in milligrams of each tumor in the fresh state. The tumors were subsequently fixed with buffered 10% formaldehyde for more than 72 hours. Blocks of tumors in size of 0.5 × 0.5 × 0.5 cm3 were dehydrated using a graded ethyl alcohol series and then infiltrated with liquefied paraffin. The paraffin blocks were sliced to sections of 5 to 10 microns in thickness with a sharp steel knife in the microtome. The sections of tissue slices were placed on slides for Hematoxylin and Eosin (H&E) stain, apoptotic assay, and proliferation assay. Fig. 2a. A subcutaneous tumor derived from CRL-1623 cells inoculated onto the back of a NOD-SCID mouse. Figure 2b (right). Dissection of CRL-1623 cell line-derived xenografted tumor from subcutaneous layer in a NODscid mouse. The firm yellowish tumors were well-defined, highly-vascular, and adherent to the underlining muscular layer. The H&E stain was used to confirm the morphologic characters of the tumor cells (26). DNA fragmentation detection kits (TdT-FragEL) from Oncogene Research Products (Mass., USA) were used to detect the apoptosis of tumor cells by fragment end labeling of the DNA. In this assay, terminal deoxynucleotidyl transferase (TdT) binds to exposed 3’-OH ends of DNA fragments and catalyzes the addition of biotin-labeled and unlabeled deoxynucleotides during incubation at 37°C for 1.5 hours. Biotinylated nucleotides were detected using a streptavidin-horseradish peroxidase conjugate. The labeled sample was incubated with diaminobenzidine at room temperature for 10 to 15 minutes to generate an insoluble colored substrate at the site of DNA fragmentation. The specimen was counterstained with methyl green as a contrast agent for morphological evaluation and characterization of normal and apoptotic cells (27, 28). A positive control was generated by TdT-FragEL staining of human acute myeloid 253 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells leukemia HL60 cells induced to undergo apoptosis with 0.5 µg/ml actinomycin D (slide supplied by Oncogene, Mass., USA). The proliferating activity of the tumor cells was evaluated using an immunohistochemical stain. After endogenous peroxidase activity was quenched by incubating the specimen with 3% hydrogen peroxide at room temperature, it was incubated with the primary mouse monoclonal antibody (generated by immunizing BALB/c mice with recombinant PCNA fused with myeloma SP2/0-Ag14; DAKO Inc, Calif., USA) overnight in a humidified chamber at 4o C. Then the specimen was incubated with a biotinylated secondary anti-mouse antibody and peroxidase-labeled streptavidin (DAKO Inc, Calif., USA). Staining was complete after 10 minutes of incubation with diaminobenzidine, which resulted in a brown precipitate at the antigen sites. The background was counterstained with hematoxylin (29, 30). Analysis and Statistics Representative slides of H&E, TdT-FragEL, and PCNA assays for each tumor were analyzed using a light microscope (Olympus, CH30, Tokyo, Japan) at magnifications of 400X (H&E, TdT-FragEL) and 1000X (PCNA). Indexes of the apoptosis (TdT-FragEL stained cells) and tumor cell proliferating activity (PCNA stained cells) were calculated using the formula: total number of positive stained cells in 10 microscopic fields 10 All of the measurement values were expressed as mean ± SEM. Two-tail Student’s t-test was performed for comparison between the experimental group and the control group. The statistical significance was defined as P < 0.05. RESULTS Human oral cancer cells derived from the CRL-1623 cell line were inoculated into the back of 40 NODscid mice successfully. By the end of the experiment, each animal had a noticeable bulge in the inoculation region (see Figure 2, previous page). No seizures or other hyperoxia-related complications developed during the experiment. The mean body weight of the experimental group (32.2 ± 0.58 g) showed no significant difference between that of control group (31.4 ± 0.67 g) at the end of the experiment. The mean fresh tumor weight of the HBO2 treated mice was 4.01 ± 0.40 g, which compared to the mean fresh tumor weights of the control animals (4.42 ± 0.44 g), was not statistically different (Table 1). Microscopic examination of the control and experimental H&E stained paraffin-embedded tumor sections revealed well differentiated squamous cell carcinomas that were not morphologically distinct. Furthermore, the grades of differentiation of the tumors from both the control and experimental animals were similar (Figure 3). In addition to the static parameters of tumor growth, the apoptotic index and proliferating activity of each tumor were examined. The functional apoptotic status of the tumor cells was evaluated using the TdT-FragEL stain. There was very little apoptotic activity for the tumor derived from the CRL-1623 cell line (Figure 4). 254 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells Table 1: The effect of HBO2 on the CRL1623 cell line-derived xenograft tumors. HBO2 group (n = 20) Control group (n = 20) P value Body Weight (g) 32.2 ± 0.58 31.4 ± 0.67 0.3844 Fresh Tumor Weight (g) 4.01 ± 0.40 4.42 ± 0.44 0.4954 Apoptotic Index 1.18 ± 0.26 1.23 ± 0.30 0.9030 Proliferating Activity Index 81.5 ± 2.77 84.8 ± 5.04 0.5485 Table 1. Values are expressed as mean ± SEM. Two tailed Student’s t-test was used for comparison of the data. The apoptotic index is calculated from the mean positive TdT-FragEL stained cells of 400X light microscopy. The proliferating activity index is calculated from the mean positive PCNA stained cells under light microscope with 1000X magnification. The body weight, fresh tumour weight, apoptotic index, and proliferating activity index of CRL-1623 cell line-derived xenografted tumours in NODscid mice after 20 treatments with hyperbaric oxygen at 2.5 ATA for 90 minutes were all not significantly different from those in the control animals. Fig. 3. Representative views of a CRL-1623 cell line-derived xenografted tumor in NODscid mice. The xenografted tumor cells were very similar to those found in well-differentiated squamous cell carcinomas in human oral cavities. There is no difference in morphology and grade-differentiation between HBO2-treated (left) and control (right) tumors (400X magnification). Fig. 4. Representative view of the apoptosis assay (TdT-FragEL) in cells from CRL-1623 cell line-derived xenografted tumors in NODscid mice. The arrow indicates a dark brown stained apoptotic cell (400X magnification). The calculated apoptotic index expressed as the mean positive TDT-FragEL stained cells under 400X light microscopy for the HBO2 treated group was 1.18 ± 0.26 and that for the control group was 1.23 ± 0.30. There were no statistical differences in apoptotic activity between the two groups. The high number of PCNA immunohistochemically-stained cells shown in Figure 5 indicates the high 255 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells level of proliferating activity in the CRL-1623 cell line. The proliferating activity index for the HBO2 group (81.5 ± 2.77) was not significantly different from that of control group (84.8 ± 5.04). Fig. 5. Representative view of proliferating cell nuclear antigen (PCNA)-stained cells from CRL-1623 cell line-derived xenografted tumors in NODscid mice. The arrows indicate the positive dark brown stained proliferating cells. (400X magnification). DISCUSSION A growing body of strong evidence supports the use of HBO2 as an effective adjunctive therapy for treating delayed radiation injury in various diseases (1-3, 31-37). Unfortunately, a growth-promoting effect makes HBO2 a contraindication for patients with concerns of malignancies (12). For example, many patients develop mandibular ORN after wide excision and radiotherapy for oral cancers, and some who undergo painful surgical and radiation procedures are found to have soft tissue break down and bony erosions months after their initial treatments. Although it is clear that HBO2 is an effective adjunct for managing ORN, we considered the risks of nourishment and proliferation of residual or recurrent tumor cells in a high oxygen environment and/or the promotion of new malignancies due to ROS formation during HBO2 treatment of mandibular ORN to be worthy of further examination. Feldmeier et al. reviewed 24 scientific articles published between 1960 and 1993. The results of three clinical studies and two animal model studies supported the statement that HBO2 had a growth promoting effect on malignancies (11). However, most of the studies did not focus on the oral cancers. One study on oral cancer used an animal model in which the buccal cancer was induced by repeated application of the carcinogen dimethylbenzanthracene (DMBA) to the buccal pouch of golden Syrian hamster (13). However, the experimental model in hamsters is far removed from the human condition and the behavior of induced cancer in this model would not be the same as for humans. Thus, the responses achieved during their study should not be used as the final word (4, 11). For example, human papillomavirus type 16 and 18 demonstrate oncogenicity by transforming normal human oral keratinocytes in vitro. However, repeated viral inoculation of hamster oral mucosa failed to produce tumors or histopathological evidence of malignancy (38). Marx and Johnson designed an investigation using the hamster cheek pouch model (39). In contrast to the results of McMillan et al. (13) which suggested HBO2 had a stimulatory effect during the proliferate phase of DMBA-induced carcinoma, their results indicated that HBO2 had no effect on the development of early dysplastic changes and had a suppressive effect on the transformation from dysplasia to malignancy. To elucidate the effects of HBO2 on oral cancer, further studies using different models are necessary. Myers et al. used an experimental animal xenograft to evaluate the effects of target molecular therapy for oral cancer (40). However, HBO2 studies using xenograft animal models usually relied on static weight and volume of tumors as parameters for evaluating tumor growth (13-15). The dynamic status of 256 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells tumor cells including the number of cells programmed to die and the number of cells undergoing proliferation remains unknown. Apoptosis, or programmed cell death, has been a prevalent topic of research in recent years (41-44). There are three different mechanisms by which a cell commits suicide via apoptosis (45-48). First, apoptosis is triggered by death signals, either extrinsic or intrinsic. Second, apoptosis is triggered by deprivation of survival signals. Third, apoptosis is induced by specific radiation or anti-cancer drugs. Serial enzymatic reactions are induced and lead to chromatin condensation and fragmentation of DNA (49). In this study, we used the terminal deoxynucleotidyl transferase DNA fragmentation end-labeling technique to determine the status of apoptosis for each tumor (50). PCNA is a cyclin protein of 37 kD molecular weight also called polymerase-δ accessory protein. It is recognized that there are very high correlations between PCNA expression and the proliferation activity of cells (51). Recently, PCNA has been used to evaluate tumor growth in various malignancies, including lung cancer, (52) hepatocellular carcinoma, (19, 20) squamous cell carcinoma, (53) and tumors originating in the central nervous system (18). In the present study, immunohistochemical staining for PCNA was used to indicate the proliferating activity of tumors derived from a human oral cancer cell line. To our knowledge, there has been no previous HBO2 study that used the apoptosis and PCNA assays to evaluate the HBO2 associated cancer-promoting effects. Most tumor evaluation methods have used tumor numbers, weights, and volumes. It has been recognized that the PCNA labeling index correlated with the clinical outcome and grading of malignant central nervous and hepatic tumors (18, 19). Greene et al. used apoptosis and PCNA assays to evaluate the effects of basic fibroblast growth factor (bFGF) and the angiogenesis inhibitor TNP-470 on hepatic regeneration after partial hepatectomy. Their results suggested that the cessation of the regenerative process correlated with a decrease in endothelial proliferation and an increase in endothelial apoptosis (54). Kohno et al. also demonstrated that the apoptosis and PCNA labeling index reflected the pathological alterations of human oral carcinogenesis (55). It is clear that the application of the apoptosis and PCNA assays provided evidence about the dynamic nature of HBO2 on human oral cancer cells. The in vivo xenograft model used in our study presented a very hypercellular picture. Roughly, an average of 1076 tumor cells was seen in a microscopic field of 400X magnification. Comparing with the data of Kohno et al., in which the experimental oral tumors presented a 35% positive stain for PCNA and 22% for apoptosis assay (55), our data demonstrated a very active proliferation activity (about 80% positive stain for PCNA) and extremely low apoptosis (about 1%). The results of these two novel assays in our study showed that the malignant tumors derived from the CRL-1623 cell line of both the HBO2 group and the control group had low apoptotic and high proliferation potentials. HBO2 did not show significant effects on toxicity or nourishment of these squamous carcinoma cells. Most of the previous studies involved assessment of cancer recurrence over a short period of time. It was not realistic for HBO2-mediated cancers to recur on a long time scale following treatment. An advantage of this study using apoptotic and proliferating activity indices was that these assays may potentially indicate growth recurrence of squamous cell carcinoma over a longer time scale. For the low apoptosis index shown in our results, a positive control was established by using TdT-FragEL staining of human leukemia HL-60 cells induced to undergo apoptosis with 0.5 µg/ml actinomycin D to verify the apoptosis assay functioned properly. We did not use a second cell line to examine for differences in apoptotic activity index in our animal 257 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells model. However, new evidence on the benign effects of HBO2 was demonstrated on oral cancer cells. In summary, we used NODscid mice with profound immunodeficiency, CRL-1623 cell line of high and constant tumorigenecity, and the dynamic evaluation of tumor growth using TdT-FragEL and PCNA assay. The results showed that there were no significant differences in body weight, tumor weight, apoptotic index or proliferating activity between the HBO2 group and the control group. CONCLUSION The results of our study showed that 20 HBO2 treatments at a dose of 2.5 atm abs for 90 minutes did not promote the growth or proliferation of human oral cancer cells. ACKNOWLEDGMENTS This work was supported by Buddhist Tzu Chi Medical Center grant TCRD91-21. The authors gratefully acknowledge the assistance of Miss Tsuey-Hwa Tsai, Prof. Terry B.J. Kuo, Prof. Cheryl C.H. Yang, and Department of Medical Research. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Marx RE. A new concept in the treatment of osteoradionecrosis. J Oral Maxillofac Surg 1983; 41: 351-357. Marx RE, Johnson RP. Studies in the radiobiology of osteoradionecrosis and their clinical significance. Oral Surg Oral Med Oral Pathol 1987; 64: 379-390. Feldmeier JJ, Heimbach RD, Davolt DA, McDonough MJ, Stegmann BJ, Sheffield PJ. Hyperbaric oxygen in the treatment of delayed radiation injuries of the extremities. Undersea Hyperb Med 2000; 27: 15-19. Feldmeier JJ, Hampson NB. A systematic review of the literature reporting the application of hyperbaric oxygen prevention and treatment of delayed radiation injuries: an evidence based approach. Undersea Hyperb Med 2002; 29: 4-30. Zamboni WA, Roth AC, Russell RC, Graham B, Suchy H, Kucan JO. Morphologic analysis of the microcirculation during reperfusion of ischemic skeletal muscle and the effect of hyperbaric oxygen. Plast Reconstr Surg 1993; 91: 1110-1123. Mink RB, Dutka AJ. Hyperbaric oxygen after global cerebral ischemia in rabbits does not promote brain lipid peroxidation. Crit Care Med 1995; 23: 1398-1404. Tibbles PM, Edelsberg JS. Hyperbaric-oxygen therapy. N Eng J Med 1996; 334: 1642-1648. Thom SR, Mendiguren I, Hardy K, Bolotin T, Fisher D, Nebolon M, Kilpatrick L. Inhibition of human neutrophil beta2-integrin-dependent adherence by hyperbaric O2. Am J Physiol 1997; 272: C770-C777. Zamboni WA, Stephenson LL, Roth AC, Suchy H, Russell RC. Ischemia-reperfusion injury in skeletal muscle: CD 18-dependent neutrophil-endothelial adhesion and arteriolar vasoconstriction. Plast Reconstr Surg 1997; 99: 2002-2007. Buras JA, Stahl GL, Svoboda KK, Reenstra WR. Hyperbaric oxygen downregulates ICAM-1 expression induced by hypoxia and hypoglycemia: the role of NOS. Am J Physiol - Cell Physiol 2000; 278: C292-C302. Feldmeier JJ, Heimbach RD, Davolt DA, Brakora MJ, Sheffield PJ, Porter AT. Does hyperbaric oxygen have a cancer-causing or -promoting effect? A review of the pertinent literature. Undersea Hyperb Med 1994; 21: 467-475. Jain KK. Textbook of hyperbaric medicine. 3rd rev. ed. Gottingen: Hogrefe and Huber publisher, 1999. McMillan T, Calhoun KH, Mader JT, Stiernberg CM, Rajaraman S. The effect of hyperbaric oxygen therapy of oral mucosal carcinoma. Laryngoscope 1989; 99: 241-244. 258 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Headley DB, Gapany M, Dawson DE, Kruse GD, Robinson RA, McCabe BF. The effect of hyperbaric oxygen on growth of human squamous cell carcinoma xenografts. Arch Otolaryngol -- Head Neck Surg 1991; 117: 1269-1272. Sklizovic D, Sanger JR, Kindwall EP, Fink JG, Grunert BK, Campbell BH. Hyperbaric oxygen therapy and squamous cell carcinoma cell line growth. Head Neck 1993; 15: 236-240. Moriki T, Takahashi T, Kataoka H, Hiroi M, Yamane T, Hara H. Proliferation marker MIB-1 correlates well with proliferative activity evaluated by BrdU in breast cancer: an immunohistochemical study including correlation with PCNA, p53, c-erbB-2 and estrogen receptor status. Pathology International 1996; 46: 953-961. Zhang Y, Fujita N, Tsuruo T. Caspase-mediated cleavage of p21Waf1/Cip1 converts cancer cells from growth arrest to undergoing apoptosis. Oncogene 1999; 18: 1131-1138. Kayaselcuk F, Zorludemir S, Gumurduhu D, Zeren H, Erman T. PCNA and Ki-67 in central nervous system tumors: correlation with the histological type and grade. J Neuro-Oncol 2002; 57: 115-121. Paiva C, Oshima CT, Lanzoni VP, Forones NM. Apoptosis, PCNA and p53 in hepatocellular carcinoma. Hepato-Gastroenterol 2002; 49: 1058-1061. Zeng WJ, Liu GY, Xu J, Zhou XD, Zhang YE, Zhang N. Pathological characteristics, PCNA labeling index and DNA index in prognostic evaluation of patients with moderately differentiated hepatocellular carcinoma. World J Gastroenterol 2002; 8: 1040-1044. Prochazka M, Gaskins HR, Shultz LD, Leiter EH. The nonobese diabetic scid mouse: model for spontaneous thymomagenesis associated with immunodeficiency. Proc Natl Acad Sci USA 1992; 89: 3290-3294. Williams SS, Alosco TR, Croy BA, Bankert RB. The study of human neoplastic disease in severe combined immunodeficient mice. Lab Anim Sci 1993; 43: 139-146. Rheinwald JG, Beckett MA. Defective terminal differentiation in culture as a consistent and selectable character of malignant human keratinocytes. Cell 1980; 22: 629-632. Rheinwald JG, Beckett MA. Tumorigenic keratinocyte lines requiring anchorage and fibroblast support cultures from human squamous cell carcinomas. Cancer Res 1981; 41: 1657-1663. Wu YJ, Rheinwald JG. A new small (40 kd) keratin filament protein made by some cultured human squamous cell carcinomas. Cell 1981; 25: 627-635. Bancroft JD, Cook HC, Stirling RW. Principles of tissue demonstration and routine morphological staining. In: Bancroft JD, Cook HC, Stirling RW, eds. Manual of histological techniques and their diagnostic applications. New York: Churchill Livingstone, 1994: 17-34. Silvestrini G, Mocetti P, Ballanti P, Di Grezia R, Bonucci E. In vivo incidence of apoptosis evaluated with the TdT FragEL DNA fragmentation detection kit in cartilage and bone cells of the rat tibia. Tissue Cell 1998; 30: 627-633. Sciandrello G, Barbaro R, Caradonna F, Barbata G. Early induction of genetic instability and apoptosis by arsenic in cultured Chinese hamster cells. Mutagenesis 2002; 17: 99-103. Fujiwaki R, Hata K, Iida K, Maede Y, Koike M, Miyazaki K. Thymidine phosphorylase expression in progression of cervical cancer: correlation with microvessel count, proliferating cell nuclear antigen, and apoptosis. J Clin Pathol 1999; 52: 598-603. Martins AC, Faria SM, Cologna AJ, Suaid HJ, Tucci S, Jr. Immunoexpression of p53 protein and proliferating cell nuclear antigen in penile carcinoma. J Urol 2002; 167: 89-92. Kindwall EP, Whelan HT. Hyperbaric medicine practice. 2nd ed. Flagstaff: Best publishing company, 1999. Mansfield MJ, Sanders DW, Heimbach RD, Marx RE. Hyperbaric oxygen as an adjunct in the treatment of osteoradionecrosis of the mandible. J Oral Surg 1981; 39: 585-589. Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Maxillofac Surg 1983; 41: 283-288. Marx RE, Ames JR. The use of hyperbaric oxygen therapy in bony reconstruction of the irradiated and tissue-deficient patient. J Oral Maxillofac Surg 1982; 40: 412-420. Marx RE, Johnson RP, Kline SN. Prevention of osteoradionecrosis: a randomized prospective clinical trial of hyperbaric oxygen versus penicillin. J Am Dent Assoc 1985; 111: 49-54. Moon RE, Feldmeier JJ. Hyperbaric oxygen: an evidence based approach to its application. Undersea Hyperb Med 2002; 29: 1-3. Neovius EB, Lind MG, Lind FG. Hyperbaric oxygen therapy for wound complications after surgery in the irradiated head and neck: a review of the literature and a report of 15 consecutive patients. Head Neck 1997; 19: 315-322. Park NH, Li SL, Xie JF, Cherrick HM. In vitro and animal studies of the role of viruses in oral carcinogenesis. 259 UHM 2004, Vol. 31, No. 2 – HBO2 on human oral cancer cells 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. Eur J Cancer 1992; Part B: 145-152. Marx RE, Johnson RP. Relationship of hyperbaric oxygen to oral cancer. In: Davis JC, Hunt TK, eds. Problem wounds: the role of oxygen. New York: Elsevier, 1988: 107-110. Myers JN, Holsinger FC, Bekele BN, Li E, Jasser SA, Killion JJ, Fidler IJ. Targeted molecular therapy for oral cancer with epidermal growth factor receptor blockade: a preliminary report. Arch Otolaryngol -- Head Neck Surg 2002; 128: 875-879. Kerr JF, Wyllie AH, Currie AR. Apoptosis: a basic biological phenomenon with wide-ranging implications in tissue kinetics. Br J Cancer 1972; 26: 239-257. Martin SJ, Lennon SV, Bonham AM, Cotter TG. Induction of apoptosis (programmed cell death) in human leukemic HL-60 cells by inhibition of RNA or protein synthesis. J Immunol 1990; 145: 1859-1867. Fawthrop DJ, Boobis AR, Davies DS. Mechanisms of cell death. Arch Toxicol 1991; 65: 437-444. Gu Y, Jow GM, Moulton BC, et al. Apoptosis in decidual tissue regression and reorganization. Endocrinol 1994; 135: 1272-1279. Nagata S, Golstein P. The Fas death factor. Science 1995; 267: 1449-1456. Nagata S. Apoptosis by death factor. Cell 1997; 88: 355-365. Raff M. Cell suicide for beginners. Nature 1998; 396: 119-122. Vaux DL, Korsmeyer SJ. Cell death in development. Cell 1999; 96: 245-254. Wyllie AH. Glucocorticoid-induced thymocyte apoptosis is associated with endogenous endonuclease activation. Nature 1980; 284: 555-556. Gavrieli Y, Sherman Y, Ben-Sasson SA. Identification of programmed cell death in situ via specific labeling of nuclear DNA fragmentation. J Cell Biol 1992; 119: 493-501. Haracska L, Unk I, Johnson RE, Phillips BB, Hurwitz J, Prakash L, Prakash S. Stimulation of DNA synthesis activity of human DNA polymerase kappa by PCNA. Mol Cell Biol 2002; 22: 784-791. Griffey SM, Kraegel SA, Madewell BR. Proliferation indices in spontaneous canine lung cancer: proliferating cell nuclear antigen (PCNA), Ki-67 (MIB1) and mitotic counts. J Comp Pathol 1999; 120: 321-332. Niu Y, Liu F, Zhou Z, Wang H. Expression of CD44V6 and PCNA in squamous cell carcinomas. China Med J 2002; 115: 1564-1568. Greene AK, Wiener S, Puder M, et al. Endothelial-directed hepatic regeneration after partial hepatectomy. Ann Surg 2003; 237: 530-535. Kohno Y, Patel V, Kim Y, et al. Apoptosis, proliferation and p12(doc-1) profiles in normal, dysplastic and malignant squamous epithelium of the Syrian hamster cheek pouch model. Oral Oncol 2002; 38: 274-280. 260