Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
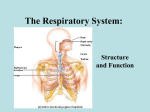
Physiological changes in respiratory function associated with ageing Physiological ageing of the lung is associated with dilatation of alveoli, enlargement of airspaces, decrease in exchange surface area and loss of supporting tissue for peripheral airways (“senile emphysema”), changes resulting in decreased static elastic recoil of the lung and increased residual volume and functional residual capacity. Compliance of the chest wall diminishes, thereby increasing work of breathing when compared with younger subjects. Respiratory muscle strength also decreases with ageing, and is strongly correlated with nutritional status and cardiac index. Expiratory flow rates decrease with a characteristic alteration in the flow–volume curve suggesting small airway disease. The ventilation–perfusion ratio (V ′A/Q ′) heterogeneity increases, with low V ′A/Q ′ zones appearing as a result of premature closing of dependent airways. Carbon monoxide transfer decreases with age, reflecting mainly a loss of surface area. In spite of these changes, the respiratory system remains capable of maintaining adequate gas exchange at rest and during exertion during the entire lifespan, with only a slight decrease in arterial oxygen tension, and no significant change in arterial carbon dioxide tension. Ageing tends to diminish the reserve of the respiratory system in cases of acute disease. Decreased sensitivity of respiratory centres to hypoxia or hypercapnia results in a diminished ventilatory response in cases of heart failure, infection or aggravated airway obstruction. Furthermore, decreased perception bronchoconstriction and diminished physical activity may result in lesser awareness of the disease and delayed diagnosis. GI • • • • • • • • • • alterations in taste and smell, gastric motility, intestinal overgrowth and changes in gastrointestinal hormone release are the basis of the physiological anorexia of aging. Alterations in swallowing lead to silent aspiration. Changes in gastric emptying play a role in postprandial hypotension. Changes in gastrointestinal function can lead to constipation and fecal incontinence. Weakening of the colonic muscular wall produces diverticula. Achlorhydria is associated with malabsorption of some forms of iron and calcium. Vitamin D malabsorption aggravates the hypovitaminosis D that is so common in older persons. Changes in probiotics can lead to diarrhea and altered immune system. In the liver, aging is associated with delayed drug metabolism. Summary: Changes in the physiology of the gut play a role in the anorexia of aging, aspiration pneumonia, postprandial hypotension, constipation and fecal incontinence.