Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
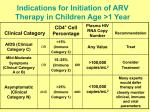
Challenges in monitoring ARV therapy A clinical and public health view of the issues involved Charlie Gilks SRM team, HIV department The M&E Pipeline MONITORING EVALUATION Process Evaluation Effectiveness Evaluation INPUTS PROCESS OUTPUTS OUTCOMES IMPACT Core problem for ART Programmes ART does not easily fit into M&E pipeline • • • • The only easy parts to define are the inputs Process is complex and open-ended Outputs differ according to the processes Outcome and Impact (the goals of therapy) are varied and have not been agreed upon Quality not just quantity - numbers on ART Processes and Outputs • ART turns HIV into a chronic disease process - open-ended, continuous therapy with lifelong care - in life, healthy people/healthier patients move around - long-term adherence matters • ART and the simplified Public Health approach - different treatments: first line and second line - toxicity means some drugs have to change - many patients will end up failing treatments Outcomes and Impact Several different measures of “effectiveness” – – – – improved survival / mortality rates quality of life reduction in HIV transmission drug resistance contained Which should programmes be evaluated on? How will this be decided? This critically impacts the M&E process Developing process indicators Key is to simplify clinical decision making process Then standardise indicators around this Charlie’s four S’s - the core of ARV management: – – – – Start according to guidelines on first-line ART Substitute single drug for toxicity Switch for failure to second-line ART Stop and move to palliative care sadly, this only works in english …. but the principle are the same Addressing the Process Issues The key is matching up different system flows patients on treatment drug supplies money (fee for service) All intersect at the point of dispensing ARVs Different components with this linkage What are the components - 1 Patient identifier: mobility and life-long care – unique – non-transferable – robust Drug supply: link ordering to use – tracking stock to and in pharmacy – dispensing/prescribing log – avoid stock-outs, expiry on shelf and pilfering What are the components - 2 • Patient records and forms: progress and Px – facility-based: clinical notes, patient registers – patient-held: treatment card • Data collection system: new or integrated – data to central monitoring points – data transfer in timely fashion (warehouse, MoH, M&E unit, budget centres) Current approaches Most projects use paper records (as does TB) Complex, non-standardised data collection Grave disadvantages with paper: – – – – slow inaccurate insecure labour-intensive Paper may work in single facility but not robust enough to go to scale, or for national reporting What can technology offer ? • • • • Unique patient identifier - fingerprints bar-coding of drug cartons smart cards (clinic data and prescriptions) simple smart card readers – treatment centres – dispensing centres • mobile telephone-based linkages The “Luddite” view Sceptics abound when technology is discussed • • • • too fragile for developing countries too complex for public sector to organise too costly staff not competent or skilled enough to use There is no other way to monitor ART to scale This is a unique opportunity to fast-tract change Some conclusions M&E of ART is complex and challenging Need for consensus on goals of treatment Processes can be simplified (around the 4S’s) Standardised indicators can be developed Facility-based paper records inadequate for task “Technology” can and will have to be utilised