Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
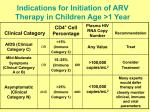
Treatment Adherence HIV Care, Support, and Treatment Office of Overseas Programming & Training Support (OPATS) Antiretroviral Therapy (ART) ART dramatically improves the quality of life of PLHIV and restores hope –Patients gain weight, are less fatigued, feel better, are often able to return to work –Slows or stops progression of illness Joseph Jeune, a farmer in Haiti, before and after treatment for HIV/AIDS and TB co-infection Access to ART While access to HIV treatment has increased by 63 percent from 2009 to 2011, only 54 percent of people eligible for HIV treatment in low and middle-income countries were on ART in 2012 Care and Treatment in the pre-ART Period Critical to identify HIV-infected persons early and enroll in care and support services After diagnosis, but before ART, regular clinic visits and care and support services are vital – For clinic checkups (prophylaxis, screening, treatment for OIs, to monitor progression, etc.) – For education in self-care and living positively to stay healthy and maintain strong immune system – To meet psychosocial needs (support groups, etc.) Eligibility for ART Prompt and timely initiation of ART results improved quality of life and reduced mortality Eligibility for ART is determined at the clinic – When CD4 thresholds are reached (and other criteria) – And before OIs contribute to poor outcomes CD4 Count The major lab indicator of immune function in PLWHIV Key factor in determining: – Urgency of antiretroviral therapy (ART) initiation – Need for prophylaxis for opportunistic infections Strongest predictor of subsequent disease progression and survival Clinical Exams for ART Eligibility Medical history Physical exam: WHO clinical staging and disease classification Laboratory tests: CD4 count, Viral load, OI screening (including TB) Country-specific ART Eligibility Criteria: South Africa Example Adults: CD4 count <350 cells/mm OR clinical staging 3 and 4 (WHO) OR patient with TB Infants and children: All children under 5, irrespective of CD4 cell count Fast tracking ART initiation: Children under 1, CD4 cell count <200 cells/mm, clinical staging 4, women who are pregnant or breastfeeding, patients with TB and CD4 cell count <50 cells/mm ART: How It Works ART uses a combination of at least three ARVs – This combination suppresses the HIV virus and stops the virus from multiplying – With less virus, the immune system becomes stronger, resists infections, and the person gets sick less often NOTE: ART does not completely destroy the virus or cure the disease and ART can reduce, but not eliminate the risk of HIV transmission. People on ART can still transmit the virus to others. ARV Drugs The combination of three drugs reduces the likelihood of the virus developing resistance First, second, and third-line therapies are different combinations of ARV drugs – First-line: Usually standard, but doctor may adjust if patient is pregnant or if person has TB – Second-line: Prescribed if first-line does not work or if there are side effects – Third-line: National guidelines, based on funding, sustainability, and ART access Successful Treatment with ARVs Must be taken daily for remainder of patient’s life to continually suppress the virus – Must be taken at specific times of day, under specific conditions – Must be carefully stored – Must take 95 percent or higher of scheduled doses – Most effective when patients are well-nourished If ARVs are NOT taken correctly, benefits are rapidly reversed, virus may become resistant Predicted and observed risk of viral control according to the longer interval of treatment discontinuation, POSOVIR and REACH cohorts Side Effects of ARVs All medicines can cause side effects, including ARVs. Most common with ARV: – Headaches, nausea, diarrhea, skin rashes, tingling sensations, tiredness, nightmares or anxiety, and changes in body Vary in severity (minor/major), duration, and start; some manageable by patient Can interfere with treatment adherence, lessen quality of life, or cause long-term health conditions ART and TB Treatment PLHIV more susceptible to TB; TB most common cause of death of PLHIV A doctor must decide how to treat both diseases in people with both TB and HIV Some ARVs cannot be used at the same time as some TB drugs; thus, a doctor will prescribe a special first-line ARV drug combination for patients with TB Treatment Adherence The ability to start, manage, and maintain a given medication regimen at the times, frequencies, and under specific conditions as prescribed by a health care provider MORE than just taking drugs – Patient attends all scheduled clinical care visits, follow-up appointments and monitoring, lab tests – Patient practices recommended behaviors (diet, limiting use of alcohol) The Importance of Treatment Adherence Suboptimal adherence – Treatment failure – Limited future treatment options (secondline therapy much more expensive, often unavailable) – Increased risk of HIV transmission to others – Increased mortality Care and Support is Vital for Treatment Adherence ART Initiation and Patient Readiness ART initiation involves a partnership between PLHIV and the health system –Critical to involve patient in decision –Requires adequate preparation and support –Requires commitment from patient Patient Preparation for ART Counseling – To identify barriers and solutions Training – Treatment literacy Patient Assessment – Beliefs, attitudes, mental health Identification of social support – Help with disclosure, socioeconomic situation Development of a treatment plan Barriers to Treatment Adherence Individual Factors System Factors Community Factors Medication Factors Despite Barriers, Treatment Adherence Can Be Achieved Adherence is feasible in low-resource settings – 77 percent of patients in Africa achieved adequate treatment adherence (defined as taking 95 percent of prescribed pills) compared with just 55 percent in North American settings Good adherence has been shown within key populations, including sex workers and People Who Inject Drugs