Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
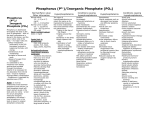
Management of Hypophosphataemia Summary Table (See below for further guidance) Mild Phosphate level (mmol/L) Oral Therapy Parental Therapy 0.6-0.79 3 to 6 tablets per day of Phosphate Sandoz Not Applicable E.g ONE or TWO tablets TWO or THREE times a day Moderate 0.32-0.59 6 tablets per day of Phosphate Sandoz E.g TWO tablets THREE times a day Severe <0.32 See IV for urgent correction Readily diluted phosphate Polyfusor Usually 7.5ml per hour for 12 hours (equivalent to 9 mmol over 12 hours) (Discard any remaining liquid) Readily diluted phosphate Polyfusor 2-5ml/kg over 6-12 hours. 24 hour maximum = 30mmol (300ml) 24 hour maximum in a critical care setting =50mmol (500ml) General Guidance Hypophophataemia is often asymptomatic until levels become severe (below 0.32mmol/litre). Symptoms include neuromuscular dysfunction such as muscle weakness and paraesthesia, convulsions, cardiomyopathy, respiratory failure, and haematological abnormalities. Prolonged hypophosphataemia can result in rickets or osteomalacia.1-2 Both serum level and patient condition should guide choice of treatment1-3. APPROVED BY: To be approved by North East Essex Medicines Management Committee REVIEW BY: October 2017 VERSION: 2 AUTHOR: Steven De-Giovanni 1 Oral Treatment The tablet of choice within the Trust is Phosphate Sandoz. Each tablet contains 16.1 mmol of phosphate.4 Caution in patients with sodium restriction (e.g CCF). Each tablet also contains 20.1mmol of sodium and 3.1mmol of potassium4. Tablets should be dissolved in ½ glass of water before taking4. The main side effect of oral phosphate is diarrhoea. Consider a dose reduction if this occurs.4 Avoid giving calcium at the same time as phosphate tablets (reduced bioavailability and efficacy). 2,3 Intravenous Treatment The treatment of choice for intravenous phosphate within the Trust is Phosphate Polyfusor.5 This is readily diluted and should not be infused with any other medications or IV fluids.5,6 500ml of Phosphate Polyfusor contains approximately 50mmol of phosphate5. Doses should be reduced in significant renal impairment. Seek specialist advice. Monitoring 6 Electrolytes (particularly phosphate, calcium as well as potassium). This should be at least daily (possibly 12 hourly with IV replacement therapy) Renal function Blood pressure (when giving intravenously) References 1. Sweetman S (ed.). Martindale. The Complete Drug Reference, online edition. The Pharmaceutical Press, London (accessed via www.medicinescomplete.com 28th October 2015) 2. McEvoy GK (ed.). AHFS Drug Information 2009, online edition. American Society of Health-System Pharmacists, Bethesda, USA. accessed via www.medicinescomplete.com October 28th 2015 3. British National Formulary 65 (April 2013) accessed online via www.medicinescomplete.com October 2015 4. Handbook of Injectable drugs (accessed via. www.medicinescomplete.com October 28th 2015) 4. Summary of product characteristics for Phosphate Sandoz. Date of revision of the text October 2002. Electronic Medicines Compendium. 5. Summary of product characteristics for Phosphates as Polyfusor®. Date of revision of the text August 2006. Received from Fresenius Kabi. 6. University College London Hospitals: Injectable medicines administration guide (3rd edition) Wiley-Blackwell publications APPROVED BY: To be approved by North East Essex Medicines Management Committee REVIEW BY: October 2017 VERSION: 2 AUTHOR: Steven De-Giovanni 2