Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
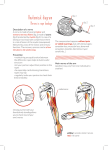
158 Practical Neurology REVIEW Pract Neurol 2008; 8: 158–169 Foot drop: where, why and what to do? John D Stewart Foot drop is a common and distressing problem that can lead to falls and injury. Although the most frequent cause is a (common) peroneal neuropathy at the neck of the fibula, other causes include anterior horn cell disease, lumbar plexopathies, L5 radiculopathy and partial sciatic neuropathy. And even when the nerve lesion is clearly at the fibular neck there are a variety of causes that may not be immediately obvious; habitual leg crossing may well be the most frequent cause and most patients improve when they stop this habit. A meticulous neurological evaluation goes a long way to ascertain the site of the lesion. Nerve conduction and electromyographic studies are useful adjuncts in localising the site of injury, establishing the degree of damage and predicting the degree of recovery. Imaging is important in establishing the cause of foot drop be it at the level of the spine, along the course of the sciatic nerve or in the popliteal fossa; ultrasonography, CT and MR imaging are all useful. For patients with a severe foot drop of any cause, an ankle foot orthosis is a helpful device that enables them to walk better and more safely. he colloquial and medical term ‘‘foot drop’’ admirably describes weakness of the dorsiflexor muscles of the foot. It is to be distinguished from flail foot, in which all the muscles below the knee are affected—the plantar flexors as well as the dorsiflexors. For neurologists, the keen-eyed lot that we are, the most familiar sighting of a foot drop is likely to be that of the late John Thaw who played the part of Inspector Morse in numerous BBC films; we do not know what the cause was.1 Although a lesion of the (common) peroneal nerve is in general the most likely cause of foot drop, the wary neurologist should pose the following questions: T Consultant Neurologist, Lions Gate Hospital, North Vancouver, British Columbia, Canada Correspondence to: Dr J D Stewart 145 East 13th Street, #204, North Vancouver, BC V7L 2L4, Canada; [email protected] 10.1136/jnnp.2008.149393 N N N N is this really a peroneal neuropathy, or could there be a more proximal lesion? if it is a peroneal neuropathy, what is the cause? what investigations will sort this out? what can be done to help the patient? ANATOMY The tibialis anterior, the main dorsiflexor muscle of the foot, is innervated by the peroneal nerve. This is derived from anterior horn cells in the lower spinal cord. Their axons travel in the L4 and L5 spinal nerve roots (‘‘roots’’), they then join to form the lumbosacral trunk that Stewart 159 connects these lumbar plexus structures to the sacral plexus (fig 1). These nerve fibres then enter the lateral trunk of the sciatic nerve which becomes the peroneal nerve when the sciatic divides just above the knee (fig 2). The lateral trunk gives off only one branch in the thigh— that to the short head of the biceps femoris muscle. All of the other hamstring muscles are innervated by the medial trunk of the sciatic nerve; that trunk becomes the tibial nerve. The peroneal nerve passes laterally through the popliteal fossa and winds around the head and neck of the fibula (fig 3). It is closely applied to the periosteum of that bone for about 6 cm and, for most of this distance, it is covered only by skin and subcutaneous tissue. It then pierces the peroneus longus muscle to reach the anterior compartment of the lower leg. At that point, the fibres of the muscle form a tendinous arch over the nerve, and this has been termed the fibular tunnel (fig 3). The nerve supplies the tibialis anterior, the extensors of the toes, and the foot everter (peroneal) muscles. It also supplies the skin over the anterolateral aspect of the lower leg from about midway between the knee and the ankle, and most of the dorsal aspect of the foot and toes. This extensive distribution of sensory loss is seen when the nerve is lacerated at the knee, However, when it is compressed, the sensory loss is much more restricted—usually just to the dorsum of the foot and toes (fig 4). In some patients there may be no sensory signs or symptoms at all, presumably because of sparing of relevant nerve fascicles within the damaged portion of the nerve. Therefore, an anatomy-based differential diagnosis of foot drop includes lesions or disorders affecting anterior horn cells, L4 or L5 roots, lumbosacral plexus, sciatic nerve and peroneal nerve. In practice, in many cases, the cause of the foot drop is clear—that is, a patient who has fallen and struck the lateral knee, or a patient with acute low back pain and classic lumbar radiculopathy symptoms. In many other patients in whom the diagnosis is less obvious, a peroneal neuropathy remains the likely diagnosis, but there are several pitfalls waiting to confound even the experienced clinician. PERONEAL NEUROPATHIES The many causes of this common focal neuropathy are listed in the table. Figure 1 The sacral plexus and the origin of the sciatic nerve. (Reproduced with permission from Stewart JD. Focal peripheral neuropathies. Third edition. Philadelphia: Lippincott Williams & Wilkins, 2000.) Figure 2 Posterior view of the course and branches of the right sciatic nerve. (Reproduced with permission from Stewart JD. Focal peripheral neuropathies. Third edition. Philadelphia: Lippincott Williams & Wilkins, 2000.) www.practical-neurology.com 160 Practical Neurology N Acute trauma is a frequent cause and includes direct blows and lacerations, severe adduction injuries and dislocations of the knee, fractures of the head or neck of the fibula, and bullet wounds. The common peroneal nerve can also be inadvertently injured during knee operations, including total knee replacement and arthroscopic surgery. A specific type of injury results from acute plantar flexion and inversion injuries at the ankle, usually severe sprains or fractures of the distal tibia and fibula;2, 3 the foot drop is usually immediate, but may not appear for several days. It seems that extreme and sudden ankle inversion exerts enough traction on the peroneal nerve in the popliteal fossa to tear the vasa nervorum where they enter the nerve sheath. N External pressure is probably the most frequent cause of peroneal neuropathy and occurs for several reasons. 4 , 5 Symptoms of a peroneal neuropathy are often noticed first on wakening from a normal night’s sleep, probably the result of sleeping in an abnormal position causing nerve compression. During long aeroplane, train and car journeys, the traveller may sleep or sit in such a position that the nerve becomes compressed. Bedridden patients often develop this neuropathy, probably due to a combination of weight loss and pressure on hard hospital mattresses or bed railings. Comatose patients can also lie in such a way as to compress the nerve. Plaster casts unfortunately remain a common cause of peroneal neuropathy. These include below knee casts with a hard upper edge that compresses the nerve as it crosses the fibular neck, and also above knee casts. Leg braces with the upper edge just below the knee, and tight bandages around the knee are other causes of compression at the fibular neck. N Crossing the legs has long been alleged to cause peroneal neuropathy by compressing the nerve between the head of the fibula and the patella or lateral femoral condyle of the opposite leg (fig 5).5–7 Leg crossing is such an ubiquitous habit that its role in causing peroneal palsy is difficult to assess, but I believe it to be the most common cause of otherwise unexplained peroneal neuropathy. This is based on the fact that many of these patients admit to being habitual leg Figure 3 Anterolateral view of the right leg showing the course, clinically relevant anatomical relations, and major branches of the common peroneal nerve. (Reproduced with permission from Stewart JD. Focal peripheral neuropathies. Third edition. Philadelphia: Lippincott Williams & Wilkins, 2000.) Figure 4 Patient with a right foot drop and sensory abnormality in the territory of the distal superficial peroneal nerve (dorsum of the foot) and the deep peroneal nerve (web space between first and second toes and a small area in the adjacent dorsum of the foot). This is the same patient as in figure 5. Informed consent was obtained for publication of this figure. 10.1136/jnnp.2008.149393 Stewart 161 crossers; the nerve involved is in the leg they habitually cross over the top of the other; and they invariably recover when they stop leg crossing. Sometimes the patient recounts an episode of unusual pressure; for example, an episode of sitting (or falling asleep) for a long period with the legs crossed and wedged under a table top, or of another person sitting on the patient’s knee when the legs were crossed. Some people, when sitting crosslegged, may either ignore the resulting paraesthesias or are unaware of them because of alcohol, drugs, illness or sleep. Perhaps some do not have warning paraesthesias, or these are not enough to wake them. Recent weight loss is sometimes very clearly associated with the development of a peroneal neuropathy (‘‘slimmer’s palsy’’). Although a metabolic cause for this condition has been propounded, it is caused by the reduction in the protective padding over the nerve and the satisfaction of once again being able to cross the legs (which obese persons cannot do).8–10 N N Farm labourers and other workers such as carpet layers who squat or kneel for long periods are particularly at risk of developing peroneal palsies (‘‘strawberry pickers’ palsy’’) (figs 6 and 7).5, 7, 11 When the fully flexed knee is bearing the whole weight of the body, the peroneal nerve is probably compressed between the biceps tendon above and the lateral head of the gastrocnemius and the head of the fibula below or, possibly, this position kinks and compresses the nerve within the fibular tunnel (fig 3). Compression at this site has been found on surgical exploration in affected farm workers. In other related postures there may be additional direct pressure against the nerve when the knee is both flexed and pressed against the ground. Perioperative peroneal neuropathy not due to direct surgical injury (see above) has been recognised for decades, but is infrequent compared to ulnar neuropathies and brachial plexopathies.12 The incidence of peroneal neuropathy related to operations remote from the leg can be judged from the report of 421 patients undergoing cardiac bypass surgery: 8 (2%) developed peroneal neuropathies.13 Compression from leg positioning or leg supports may be the cause, but nerve Figure 5 This patient sat like this through most of the history taking and denied that he habitually crossed his legs! His foot drop is shown in figure 4. Informed consent was obtained for publication of this figure. compression pre- and postoperatively can also occur, as with perioperative ulnar neuropathies, because bedridden patients may lie in such a way to compress peripheral nerves. Some perioperative peroneal neuropathies are associated with the lithotomy position. In a prospective study of 991 adults undergoing general anaesthesia and surgery while positioned in lithotomy, 15 (1.5%) developed lower limb neuropathies.14 The peroneal nerve was involved in 3 patients (0.3%). The symptoms were sensory only, and in 2 patients the neuropathy was bilateral; they all recovered well. N Postpartum foot drop is usually due to a common peroneal neuropathy, but other causes include an L5 radiculopathy Crossing the legs has long been alleged to cause peroneal neuropathy www.practical-neurology.com 162 Practical Neurology cause, but also point to pressure from the patient’s hands against the nerves while prolonged hip and knee flexion is maintained by the patient herself during labour.17, 18 TABLE Causes of peroneal neuropathy External compression During anaesthesia, coma, sleep, bed rest Plaster casts, braces Habitual leg crossing Sitting cross-legged Prolonged squatting, kneeling Direct trauma Blunt injuries, lacerations Fractures of the fibula Adduction injuries and dislocations of the knee Surgery and arthroscopy in popliteal fossa and knee Traction injuries Acute ankle injuries Masses Ganglia, Baker’s cysts, callus, fibular tumours, osteomas, haematomas Tumours Nerve sheath tumours Nerve sheath ganglia Lipomas Entrapment In the fibular tunnel Anterior (tibial) compartment syndrome Vascular Vasculitis, local vascular disease Diabetes mellitus: susceptibility to compression, ischaemic damage Leprosy Idiopathic and damage to the lumbosacral trunk (see below). Pressure on the nerve at the neck of the fibula by knee supports is one likely cause.15 In countries where prolonged natural childbirth is common, such neuropathies are often bilateral and may be due to prolonged squatting.16 Other reports confirm squatting as a Figure 6 This young man worked all day tiling a bathroom floor (A), and at the end of the job had a marked left foot drop (B). External compression and kinking of the peroneal nerve was the cause of his peroneal neuropathy. Informed consent was obtained for publication of this figure. 10.1136/jnnp.2008.149393 N Masses: the most common of these is a ganglion arising from the superior tibiofibular joint. Although benign, they are infiltrative and can compress or invade the nerve.19–21 Baker’s cysts may also compress the common peroneal nerve, and sometimes also the tibial nerve.22 Schwannomas and neurofibromas can arise anywhere along the course of the common peroneal nerve, or its two major branches, but are most common in the popliteal fossa.23 Other rare mass lesions are listed in the table. Callus from old fibular fractures, osteomas, and malignant tumours arising from the head or neck of the fibula are all possibilities. N Several cases of true entrapment of the common peroneal nerve in the fibular tunnel have been confirmed surgically.4, 24–26 The characteristic operative findings have been described as a ‘‘tight crescentic band at the origin of the peroneus longus ... constricting the nerve which was swollen proximally’’.25 Division of these bands is effective in relieving the symptoms. Such true peroneal entrapment is rare: Sidey explored 26 common peroneal nerves in 23 patients, and of the 8 with no apparent cause for the neuropathy, he found evidence of entrapment in only one.26 One other report of allegedly surgically proven peroneal nerve entrapments lacks credibility.27 Cadaver dissection studies have shown that few people have a firm fibrous arch as part of Stewart 163 N N the fibular tunnel; this may explain the rarity of nerve entrapment at this site.24 Spontaneous entrapment of the peroneal nerve should be considered when there is absolutely no identifiable cause, when other more proximal lesions have been excluded, and when symptoms and signs worsen progressively, and imaging studies (see below) are normal. Mononeuropathy multiplex syndromes may involve the common peroneal nerve. These disorders include diabetes, vasculitis, and hereditary neuropathy with liability to pressure palsies. In tuberculoid and borderline leprosy, the peroneal nerve is one of the most frequently involved major peripheral nerves. Idiopathic peroneal neuropathy is the frustrating appellation for those patients in whom no specific cause can be found. I believe that with the increasing recognition of leg crossing (including recent weight loss) as a cause, and that with improved imaging techniques, this group is shrinking. Some of these patients may have had an unnoticed episode of external compression, or pressure on the nerve during sleep. Deep peroneal nerve When a patient has neurological deficits restricted to the deep peroneal nerve, the lesion may lie in that major terminal branch of the common peroneal nerve, or there may be a partial lesion of the common peroneal nerve that only damages the fascicles going to form the deep peroneal nerve. The anterior (tibial) compartment syndrome results from raised pressure within the fascial compartment that contains the deep peroneal nerve and the muscles it supplies. Causes include excessive exercise, soft tissue trauma, fractures, haemorrhage, occlusion of the anterior tibial artery or its parent trunk, or restoration of blood flow after acute arterial insufficiency in the leg.28 Severe anterior lower leg pain, swelling and redness are associated with motor and sensory dysfunction of the deep peroneal nerve. The neuropathy is caused by compression by the swollen muscles, and improves rapidly following urgent surgical decompression of the anterior compartment. Chronic deep peroneal neuropathy can result from compression by ganglia, osteochondromas Figure 7 This young woman was in the habit of putting on her make-up sitting like this. She would also often read in the same position. After one particularly long period spent putting on make-up she developed asymmetrical peroneal neuropathies. The mechanism is likely to be kinking of the nerves during prolonged knee flexion. Informed consent was obtained for publication of this figure. and aneurysms. A chronic compartment syndrome has been described, but the involvement of the peroneal nerve is uncertain.29 EXAMINATION OF THE PATIENT WITH FOOT DROP A patient with a complete lesion of the common peroneal nerve has the classical clinical picture of paralysis of dorsiflexion and eversion of the foot, and of extension of the toes, resulting in a foot drop and a characteristic slapping gait. Weakness is present in the foot and toe dorsiflexors, the foot everter muscles, but nowhere else. The important other muscles to test in a patient with foot drop are those supplied by the L4– S1 roots, lumbosacral plexus, and sciatic nerve: the gluteal and hamstring muscles, www.practical-neurology.com 164 Practical Neurology Foot drop following hip arthroplasty is much more likely to be due to sciatic nerve damage than to pressure on the peroneal nerve at the fibular head gastrocnemius, and the tibialis posterior. This last muscle is the foot inverter and is innervated by the same roots as the tibialis anterior (L4, 5), but via the tibial nerve. The sensory loss of a peroneal neuropathy classically extends over the anterolateral surface of the lower leg and the dorsum of the foot and toes. However, except in total nerve lacerations, the sensory loss is often less widespread than the textbook description and is usually restricted to the dorsum of the foot and some toes, as discussed above (fig 4). Sometimes there are no sensory symptoms or signs. The knee and ankle reflexes should be normal in a peroneal neuropathy. If the ankle reflex is abnormal, then an L5 radiculopathy with involvement of the adjacent S1 root, or a plexus or sciatic nerve lesion are to be considered. Case 1 A 69-year-old retired nurse was out for a vigorous walk when she realised that her right foot was slapping the ground. There was also tingling on the dorsum of the foot and ankle. Over the next several days she tripped on the toes of that foot. She had been dieting and exercising and had lost 22 kg. She sat during the consultation with her right leg crossed over the left, and when this was commented on, she said she had been doing this ‘‘all the time’’ since she had lost weight and was able to cross her legs again. Examination showed weakness of the right tibialis anterior (2/5), extensor hallucis longus (3/5), and the peroneal muscles (3/5). The tibialis posterior and all other muscles in both legs were normal. There was no sensory loss. The peroneal nerve was tender to palpation at the fibular neck. Motor nerve conduction studies showed conduction blocking and slowing at the neck of the fibula; the peroneal sensory response was very small compared to that on the left. The patient refused an ankle foot orthosis. She was counselled not to cross her knees. In two months, her strength was somewhat better, and by four months, it was back to normal Take home messages l l l l Peroneal neuropathy can result from habitual leg crossing and, in this patient, illustrates the phenomenon of ‘‘slimmer’s palsy’’. The motor deficits are perfectly in keeping with the distribution of the peroneal nerve, but there was no sensory loss presumably because the sensory fascicles within the nerve were not sufficiently damaged. The tingling was probably due to nerve irritation and abnormal impulse generation. Focal nerve tenderness at the knee is a simple but valuable localising sign. Merely avoiding leg crossing can be curative. The course of the common peroneal nerve should be examined carefully. When present, local tenderness of the nerve and a Tinel’s sign at the fibular head and neck are valuable indicators of a nerve lesion there; however, one sometimes sees patients with L5 radiculopathies and tenderness of the peroneal nerve. The simple straight leg raising test, when abnormal, is always useful in indicating a root or other proximal nerve lesion. Cysts or other masses in the popliteal fossa or lateral to the knee may be found on careful palpation. Thickening of the nerve occurs in leprosy. Patients with foot drop sometimes pose a difficult diagnostic challenge for two reasons: first, partial involvement of the common peroneal nerve may produce highly variable degrees of weakness and sensory loss in the muscles and skin supplied by the nerve, and second the nerve lesion lies more proximally than the common peroneal nerve. Partial peroneal neuropathies Variable involvement of the muscles and skin supplied by the common peroneal nerve is frequent in all but complete lacerations of the nerve.5, 30, 31 Patients often have sensory only or motor only symptoms and signs. The former may involve the superficial or deep sensory branches only. Likewise, the weakness may be confined mainly to the muscles supplied by the deep or the superficial peroneal nerves. This variable motor and sensory involvement is explained by the microscopic anatomy of the nerve. At the knee, the fibres that form the deep and superficial peroneal nerves clearly lie in separate fascicles.32 Damage to the common peroneal nerve from whatever cause can produce differing involvement of individual fascicles in the nerve similar to the partial deficits seen in radial ‘‘Saturday night’’ neuropathies, and ulnar neuropathies at the elbow. DIFFERENTIAL DIAGNOSIS OF FOOT DROP The more proximal focal neuropathies that produce foot drop and masquerade as common peroneal neuropathies are: N N N N 10.1136/jnnp.2008.149393 L5 radiculopathies Lumbar plexopathies Lesions of the lumbosacral trunk of the lumbosacral plexus Sciatic neuropathies Stewart 165 The cause may be clear from the history— for example, a patient with characteristic symptoms of lumbar radiculopathy, a hip fracture, a difficult labour that may have involved the use of forceps or a clear episode of compression or trauma to the sciatic or common peroneal nerve. However, in other situations, it may not be so obvious. Lumbar radiculopathy can occur without low back pain that radiates down the leg. Foot drop following hip arthroplasty is much more likely to be due to sciatic nerve damage than to pressure on the common peroneal nerve at the fibular head. Foot drop following delivery of a child may be due to a disc herniation and L5 radiculopathy, compression of the lumbosacral trunk33 or pressure on the peroneal nerve by knee supports. An L5 radiculopathy, lumbar plexopathy and a lumbosacral trunk lesion will all produce weakness in muscles not supplied by the common peroneal nerve, notably the gluteal, hamstring and, particularly, the tibialis posterior muscle. However, damage to the lateral trunk of the sciatic nerve can exactly mimic a peroneal neuropathy because this trunk becomes the peroneal nerve. Although a trunk lesion involves the innervation to the short head of the biceps femoris, this muscle cannot be clinically examined separately from the other hamstring muscles, so electromyographic examination is required to sort this out. Fortunately, in many cases of lateral trunk lesions, there are often signs of mild involvement of the medial trunk, and these can be revealed by careful clinical and electrophysiological examination. Sometimes a generalised peripheral neuropathy appears superficially like bilateral peroneal neuropathies because foot drop is more obvious than plantar flexor weakness. In Case 2 A 33-year-old, very athletic man competed in a long distance run and cycle ride. Two days later, he realised he had started to limp and when he ran, he tripped over his left foot. He also had a foot drop and numbness over the anterolateral aspect of his lower left leg and dorsum of the foot. He denied any low back or leg pain, and habitual leg crossing. On examination two weeks later, the left tibialis anterior and extensor hallucis muscles were weak (42/5); however, tibialis posterior, gastrocnemius, hamstring, and gluteal muscles were also weak at 4–4+/5. There was sensory loss over the anterolateral aspect of the lower leg and dorsum of the foot. The left ankle reflex was less brisk than the right. Straight leg raising was normal, and the peroneal nerve was not tender at the fibular neck. Nerve conduction studies showed no evidence of a peroneal neuropathy. Needle electromyographic studies showed fibrillation potentials and polyphasic motor unit potentials in the left tibialis anterior, tibialis posterior, and gluteus medius muscles. A CT scan of the lumbosacral spine showed a large L5/S1 disc herniation on the left compressing the L5 and S1 nerve roots. The patient underwent a discectomy and made a complete recovery. Take home messages l l l The patient had symptoms that strongly suggested peroneal neuropathy, but the examination clearly showed deficits best explained by L5 and S1 radiculopathies. In spite of having a large disc herniation, he had no low back pain or ‘‘sciatica’’. Because of the athletic event preceding the symptoms, an anterior compartment syndrome was an important consideration but the absence of shin pain, swelling and hyperaemia argued strongly against that diagnosis. amyotrophic lateral sclerosis, an early feature may be foot drop. And patients with myopathies, particularly the rare distal ones, will often have foot drop. Patients with upper motor neuron weakness of the leg generally have more weakness of foot dorsiflexion than plantar flexion. In all of these, a careful examination will usually show that there are signs beyond the innervation of the common peroneal nerve. Finally, focal dystonia of the foot may present with apparent weakness in dorsiflexion. Figure 8 (A) Longitudinal ultrasonographic view of a normal peroneal nerve (PN) and the adjacent fibula (F). (B) Similar view of a peroneal nerve with an intraneural ganglion. (Reproduced with permission from Visser LH. High-resolution sonography of the common peroneal nerve: detection of intraneural ganglia. Neurology 2006;67:1473–5.) www.practical-neurology.com 166 Practical Neurology Case 3 A 35-year-old primigravida had marked low back pain in the last three months of her pregnancy. She was admitted at 41 weeks gestation and labour was induced under epidural anaesthesia. The fetus was in the right occipital lie. The second stage of labour was prolonged. Forceps were used to rotate the fetus to an occiput anterior position and then to assist in delivery. Throughout labour the mother experienced considerable pain down the left leg. This persisted and developed into burning paraesthesia over the anterolateral lower leg and dorsum of the foot. She had a marked left foot drop. Examination three weeks later showed marked weakness of the tibialis anterior, extensor hallucis longus, the peroneal muscles, and tibialis posterior muscle. There was mild weakness of the left gluteal muscles and hamstrings. There was decreased light touch over the dorsum of the foot. Reflexes were normal. Electrophysiological studies showed no peroneal motor conduction abnormalities at the knee. The peroneal and sural sensory amplitudes were both reduced in size. Needle EMG showed fibrillations and neurogenic motor unit potentials in the clinically weak muscles, but not in lumbar paraspinal muscles. A CT scan of the lumbar spine was normal. A diagnosis of damage to the lumbosacral trunk of the left lumbosacral plexus was made.33 She was fitted with an ankle foot orthosis, and made a slow but nearly complete recovery. Take home messages l l l The differential diagnosis here includes L5 radiculopathy from an L4/5 disc herniation, root damage from misplaced epidural injections, and peroneal neuropathy at the knee due to compression against stirrups, or prolonged knee flexion during delivery. Less frequent than all of these is crush damage to the lumbosacral trunk against the ala of the sacrum (fig 1) from the fetal head and/or forceps. Careful clinical examination and electrodiagnostic studies can usually localise the lesion. Imaging of the lumbar spine is helpful when disc herniation is suspected. INVESTIGATIONS Nerve conduction and electromyographic studies These are a valuable extension of the clinical examination in evaluating patients with foot drop. They should be done whenever there is the slightest concern, following a careful examination, that the foot drop may be due to something other than a peroneal neuropathy. Conduction abnormalities at the level of the fibular neck/head are often found, and electromyographic (EMG) abnormalities are restricted to muscles supplied by that nerve. When more proximal lesions are suspected, then a very useful strategy is to do needle EMG examinations of lumbar paraspinal, gluteal and hamstring muscles. Often the two most important muscles to test are the short head of the biceps femoris and the tibialis posterior, for reasons explained above. 10.1136/jnnp.2008.149393 If searching for evidence of medial trunk of sciatic nerve damage when a sciatic neuropathy with predominant lateral trunk damage is suspected, sural and tibial nerve conduction studies are helpful. The electrophysiological findings are also useful in predicting recovery. Patients with conduction blocking and little or no axonal damage as determined by EMG study of the tibialis anterior muscle often recover in a few weeks if further pressure on the nerve is avoided. Severe axonal damage neuropathies recover slowly and partially over many months. Patients with mixed axonal and conduction block neuropathies will often have a biphasic recovery: improvement within weeks is due to recovery of those fibres that have been affected by demyelination, while the much slower process of axonal regeneration takes many months—up to a year. Imaging Imaging of the knee should be done when a patient with a peroneal neuropathy of no apparent cause is not improving, or is worsening. Plain radiographs sometimes reveal a soft tissue mass or bone lesion. Ultrasonography is effective in outlining Baker’s cysts, aneurysms and ganglia (fig 8).34 CT scanning is excellent for detecting large soft tissue masses in this area. MRI is even more effective for demonstrating the range of intrinsic and extrinsic mass lesions involving the peroneal nerve (fig 9).35, 36 MANAGEMENT OF THE PATIENT WITH FOOT DROP Most patients with a peroneal neuropathy fall into one of three main groups: N N N acute trauma a recognisable compressive episode, or recurrent episodes progressive neuropathy of uncertain cause. If the type of trauma—for example, a laceration, suggests a complete transection, immediate nerve repair is indicated. Incomplete traumatic neuropathies are followed clinically, and spontaneous improvement is expected. If this does not occur within several months, surgical exploration of the nerve may be warranted because scar tissue and neuroma formation can impede axonal Stewart 167 regeneration; careful surgical resection of these, combined with cable nerve grafting can often bring about some degree of recovery. For blunt injuries that appear to be complete, waiting for spontaneous improvement to occur over a period of several months is probably the best approach. Stretch injuries of the peroneal nerve are often associated with long areas of damage. Even when they are repaired with nerve grafts, the results are poor.37 The acute compartment syndromes of the lower leg are surgical emergencies. Prompt fasciotomy is important for good recovery of nerves and muscles. When a definite compressive episode can be identified I re-evaluate the patient in two months. When leg crossing or other postural habits that may repetitively compress the nerve are suspected, I instruct the patient to avoid these and re-evaluate in two months. Extensive investigations are usually not necessary. If a patient does not show signs of improving at this time, or if they worsen, they are categorised in the progressive group. Patients with progressive peroneal neuropathies should have imaging studies. The choice between ultrasonography, CT scanning and MR imaging depends on local availability, expertise, and cost considerations. I usually do ultrasound first, then CT if the diagnosis is still uncertain, and then MRI if necessary. If a mass is discovered, it should be surgically removed unless it is a bony metastasis. If no mass is found, surgical exploration is still warranted. Some soft tissue lesions may not be visible on imaging (with improved imaging this is becoming less likely). If the patient has a true entrapment of the nerve within the Figure 9 Proton density-weighted MR axial image of the leg below the knee. The tibia lies superiorly and to the left, the fibula lower and to the right. Lateral to the neck of the fibula is a large mass (arrow) exactly where the common peroneal nerve lies. The patient had a peroneal neuropathy. The lesion was excised and was a neuroma arising from a branch of the nerve. Reproduced with permission from Loredo R, Hodler J, Pedowitz R, et al. MRI of the common peroneal nerve: normal anatomy and evaluation of masses associated with nerve entrapment. J Comput Assist Tomogr 1998;22:925–31. fibular tunnel, this can only be confirmed surgically. Patients in whom a popliteal mass is palpated when they first present with foot drop should be sent for imaging. For patients with suspected radiculopathy, imaging with CT or MR should be undertaken and further management then decided. If a lumbosacral Figure 10 (A) Foot drop caused by a severe L5 radiculopathy. (B, C) Ankle foot orthosis in place. Informed consent was obtained for publication of this figure. www.practical-neurology.com 168 Practical Neurology Case 4 A 74-year-old man underwent a right total hip replacement for advanced osteoarthritis. When mobilised by the physiotherapist two days later, it was apparent that he had a right foot drop, with paraesthesia and numbness over the anterolateral aspect of the lower leg and dorsum of the foot. He went on to develop allodynia in this area and neuropathic pain in the lower leg. The anaesthetist was blamed for poorly positioning the leg and causing a peroneal neuropathy and the orthopaedic surgeon was contemplating exploring the peroneal nerve at the knee. However, although careful neurological examination confirmed major weakness of the peroneal innervated muscles, and the gluteal, hamstring and tibialis posterior muscles were not weak, the gastrocnemius was mildly weak and the ankle reflex was absent. Also, the sensory abnormality was not only mainly in the peroneal nerve distribution, but there was some impairment in the lateral border and sole of the foot. Nerve conduction studies showed no evidence for a peroneal motor conduction abnormality at the knee. Both the peroneal and sural sensory potentials were abnormally small. Needle EMG studies showed fibrillations and neurogenic abnormalities in the tibialis anterior, the short head of the biceps femoris and, to a lesser degree, in the gastrocnemius. A diagnosis of a lesion of the sciatic nerve in which the predominant damage was to the lateral trunk, was made. The patient was fitted with an ankle foot orthosis, given medications for neuropathic pain, and eventually regained considerable strength. and prevent tripping. The most satisfactory is a lightweight plastic ankle foot orthosis that fits inside the shoe and up the back of the calf (fig 10). In cold climates, a pair of boots often suffices. If the foot drop is permanent, surgical treatment with tendon transfers should be considered. ACKNOWLEDGEMENTS This article was reviewed by David HiltonJones, Oxford, UK. REFERENCES 1. 2. 3. 4. 5. Take home messages l l l l A lesion of the sciatic nerve involving exclusively or predominantly the lateral trunk closely mimics a peroneal neuropathy. Many traumatic lesions of the proximal sciatic nerve preferentially or exclusively damage the lateral trunk. Careful examination of the muscles and skin supplied by the medial trunk of the sciatic nerve often reveals some damage to that trunk as well. Electrodiagnostic studies are a valuable tool in diagnosing the site of the lesion. Needle EMG of the short head of the biceps femoris muscle, innervated by the only branch of the lateral trunk, is particularly useful. Nerve conduction studies of the tibial nerve and EMG of muscles innervated by it are helpful in confirming some damage to the medial trunk of the sciatic nerve. 6. 7. 8. 9. 10. 11. 12. plexus lesion is suspected, then CT or MR imaging of the lower lumbar retroperitoneal area and the pelvis should be done. For sciatic nerve lesions with foot drop, it may not be necessary to perform imaging studies—for example, the post-hip surgery patient. However, if there is no apparent cause, then the main trunk of the sciatic nerve from the sciatic notch to the popliteal fossa should be imaged with MR using gadolinium enhancement searching for tumours of the nerve, or other lesions that may be impinging on it. Regardless of the cause of the peroneal palsy, patients with foot drop benefit greatly from a brace to support the foot, aid walking 10.1136/jnnp.2008.149393 13. 14. 15. 16. 17. 18. 19. Hancock S. The two of us: my life with John Thaw. Bloomsbury, 2004. Nobel W. Peroneal palsy due to hematoma in the common peroneal sheath after distal torsional fractures and inversion ankle sprains. J Bone Joint Surg Am 1966;48:1484–95. Meals RA. Peroneal nerve palsy complicating ankle sprain: a report of two cases and review of the literature. J Bone Joint Surg Am 1977;59:966–8. Berry H, Richardson PM. Common peroneal nerve palsy: a clinical and electrophysiological review. J Neurol Neurosurg Psychiatry 1976;39:1162–71. Garland H, Moorhouse D. Compressive lesions of the external popliteal (common peroneal) nerve. BMJ 1952;2:1373–8. Nagler SH, Rangell L. Peroneal neuropathy caused by crossing the legs. JAMA 1947;133:755–61. Woltman HW. Crossing the legs as a factor in the production of peroneal palsy. JAMA 1929;93:670–2. Sprofkin BE. Peroneal paralysis: a hazard of weight reduction. Arch Intern Med 1958;102:82–7. Sotaniemi K. Slimmer’s paralysis: peroneal neuropathy during weight reduction. J Neurol Neurosurg Psychiatry 1984;47:564–6. Cruz-Martinez A, Arpa J, Palau F. Peroneal neuropathy after weight loss. J Peripher Nerv Syst 2000;5:101–5. Koller RL, Blank NK. Strawberry pickers’ palsy. Arch Neurol 1980;37:320. Kroll DA, Caplan RA, Posner K, et al. Nerve injury associated with anesthesia. Anesthesiology 1994;73:202–7. Lederman RJ, Breuer AC, Hanson MR, et al. Peripheral nervous system complications of coronary bypass graft surgery. Ann Neurol 1982;12:297–301. Warner MA, Warner DO, Hopper CO, et al. Anaesthesiology 2000;93:938–42. Donaldson JO. Neurology and pregnancy. Second edition. London: WB Saunders, 1989. Bademosi O, Osuntokun O, Van de Werd HJ, et al. Obstetric neuropraxia in the Nigerian African. Int JG Gynaecol Obstet 1980;17:611–14. Reif ME. Bilateral common peroneal nerve palsy secondary to prolonged squatting in natural childbirth. Birth 1988;15:100–2. Adornato BT, Carlini WG. ‘‘Pushing palsy’’: a case of self-induced bilateral peroneal palsy during natural childbirth. Neurology 1992;42:936–8. Brooks DM. Nerve compression by simple ganglia: a review of 13 collected cases. J Bone Joint Surg Br 1952;34:391–400. Stewart 169 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. Barber KWJ, Bianco AJJ, Soule EH. Benign extraneural soft tissue tumors of the extremities causing compression of nerves. J Bone Joint Surg Am 1962;44:98–104. Stack RE, Bianco AJ, MacCarty CS. Compression of the common peroneal nerve by ganglion cysts: report of nine cases. J Bone Joint Surg Am 1965;47:773–8. Nakano KK. Entrapment neuropathy from Baker’s cyst. JAMA 1978;239:135. Suh JS, Abenoza P, Galloway HR, et al. Peripheral (extracranial) nerve tumors: correlation of MR imaging and histological findings. Radiology 1992;183:341–6. Sandhu HS, Sandhey BS. Occupational compression of the common peroneal nerve at the neck of the fibula. Aust NZ J Surg 1976;46:160–3. Maudsley RH. Fibular tunnel syndrome. J Bone Joint Surg BR 1967;49:384. Sidey JD. Weak ankles: A study of common peroneal entrapment neuropathy. BMJ 1968;2:623–6. Thoma A, Fawcett S, Ginty M, et al. Decompression of the common peroneal nerve: experience with 20 consecutive cases. Plast Reconstr Surg 2001;107:1183–9. Shields RWJ, Root KE, Wilbourn AJ. Compartment syndromes and compression neuropathies in coma. Neurology 1986;36:1370–4. Styf J. Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165–9. Wilbourn AJ. Common peroneal mononeuropathy at the fibular head. Muscle Nerve 1986;9:825–36. Sourkes M, Stewart JD. Common peroneal neuropathy: a study of selective motor and sensory involvement. Neurology 1991;41:1029–33. Sunderland S. Nerves and nerve injuries. Second edition. Edinburgh, Churchill Livingstone, 1978. Feasby TE, Burton SR, Hahn AF. Obstetrical lumbosacral plexus injury. Muscle Nerve 1992;15:937–40. PRACTICE POINTS l l l l l l l l 34. 35. 36. 37. The most common cause of a unilateral foot drop is peroneal nerve injury. Most of these patients have had a single episode of pressure to the nerve such as during a long aeroplane journey, are habitual leg crossers, or have an occupational cause for the neuropathy. When such causes are identified, the patient should be advised to avoid such risks, and good recovery is to be expected. Proximal nerve lesions mimicking a peroneal neuropathy include L5 radiculopathy, lumbosacral plexopathy and sciatic neuropathy; these produce weakness in muscles outside of the peroneal territory—for example, the hamstring and the foot invertor (tibialis posterior) muscles, and sensory loss in the tibial nerve territory. EMG and nerve conduction studies are helpful in differentiating proximal lesions from peroneal neuropathy. Footdrop due to an L5 radiculopathy sometimes occurs without any low back or radicular pain. Imaging is helpful in diagnosing the cause of foot drop, be it a more proximal nerve lesion or a progressive peroneal neuropathy at the knee. Whatever the cause of the foot drop, it is important to prescribe an ankle foot orthosis to improve gait and help prevent falls. Visser LH. High-resolution sonography of the common peroneal nerve: detection of intraneural ganglia. Neurology 2006;67:1473–5. Loredo R, Hodler J, Pedowitz R, et al. MRI of the common peroneal nerve: normal anatomy and evaluation of masses associated with nerve entrapment. J Comput Assist Tomogr 1998;22:925–31. Iverson, DJ. MRI detection of cysts of the knee causing common peroneal neuropathy. Neurology 2005;65:1829–31. Kim DH, Kline DG. Management and results of peroneal nerve lesions. Neurosurgery 1996;39:312–19. www.practical-neurology.com