Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
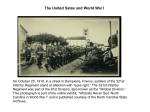
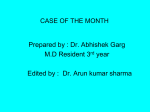
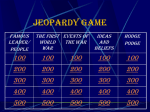
Aliment Pharmacol Ther 2004; 19: 157–165. doi: 10.1046/j.1365-2036.2003.01813.x Review article: diagnosis and current therapy of Wilson’s disease P. FEREN CI Department of Internal Medicine IV, Gastroenterology and Hepatology, University of Vienna, Austria Accepted for publication 14 October 2003 SUMMARY Wilson’s disease is an autosomal recessive inherited disorder of hepatic copper metabolism resulting in liver disease and/or neuropsychiatric disease. The diagnosis of neurological disease is straightforward if the following symptoms are present: Kayser–Fleischer rings, typical neurological symptoms and low serum ceruloplasmin levels. The diagnosis is more complex in patients presenting with liver diseases. None of the commonly used parameters alone allows a diagnosis with certainty. A combination of various laboratory parameters is necessary to firmly establish the diagno- INTRODUCTION Wilson’s disease is an autosomal recessive inherited disorder of hepatic copper metabolism resulting in the accumulation of copper in many organs and tissues. The hallmarks of the disease are the presence of liver disease, neurological symptoms and Kayser–Fleischer corneal rings. Copper is an essential dietary nutrient and is needed for such diverse processes as mitochondrial respiration, melanin biosynthesis, dopamine metabolism, iron homeostasis, antioxidant defence, connective tissue formation and peptide amidation. Specific pathways allow the intracellular trafficking and compartmentalization of copper, ensuring adequate cuproprotein synthesis whilst avoiding cellular toxicity. Biliary excreCorrespondence to: Professor P. Ferenci, Department of Internal Medicine IV, Gastroenterology and Hepatology, University of Vienna, Währinger Gürtel 18–20, A1090 Vienna, Austria. E-mail: [email protected] Ó 2003 Blackwell Publishing Ltd sis. In the future, limited mutation analysis may play an important diagnostic role. Recently, a group of international experts has proposed a score based on a variety of tests and clinical symptoms. The validity of this score needs to be assessed prospectively. Treatment requires life-long administration of copper chelators (d-penicillamine, trientine). A frequently used alternative is zinc. None of these treatments has been tested by prospective randomized controlled studies. Liver transplantation is reserved for severe or treatment-resistant cases with advanced liver disease, whilst experience with refractory neuropsychiatric disease is limited. tion is the only mechanism for copper elimination, and the amount of copper excreted in the bile is directly proportional to the size of the hepatic copper pool. Trafficking of copper in the hepatocytes is complex and involves several transport proteins. The copper transporter 1 transports copper with high affinity in a metalspecific, saturable fashion at the hepatocyte plasma membrane.1, 2 Metallothioneins, a group of cysteinerich intracellular proteins capable of binding metal ions, including copper, cadmium and zinc,3 have a critical role in protecting intracellular proteins from copper toxicity.4 Metallochaperones transfer copper to the site of synthesis of copper-containing proteins.5, 6 The cytoplasmic copper chaperone atox1 is required for copper delivery to the Wilson ATPase (ATP7B) in the hepatocyte secretory pathway7 by direct protein–protein interaction.7–9 In the copper-limiting environment of the cell, the delivery of copper by atox1 is responsible for initiating the catalytic activity and the intracellular trafficking of ATP7B.10 ATP7B is the gene product of 157 158 P. FERENCI the Wilson’s disease gene (see Figure 1) located on chromosome 13 and is a polytopic membrane protein containing several motifs characteristic of P-type ATPases.11 The histidine residue in the SEHPL motif within the cytoplasmic loop is the site of the H1069Q missense mutation, a common disease allele found in northern, central and eastern European populations with Wilson’s disease.12–15 In hepatocytes, this ATPase resides in the trans-Golgi network transporting copper into the secretory pathway for incorporation into apoceruloplasmin and excretion into the bile16 (see Figure 2). Molecular genetic analysis of affected patients reveals over 200 distinct mutations (database maintained at the University of Alberta (http://www.medgen.med.ualberta.ca)). About one-half of these mutations are missense, with most confined to recognized consensus motifs or predicted transmembrane domains. A detailed review of hepatic copper transport has recently been published.17 CLINICAL PRESENTATIONS Wilson’s disease may present with a variety of clinical conditions, the most common being liver disease and neuropsychiatric disturbances. None of the clinical signs is typical or diagnostic. One of the most characteristic features of Wilson’s disease is that no two patients, even within a family, are ever quite alike. With the increased awareness of Wilson’s disease, patients are being diagnosed earlier and ‘late’ consequences of the disease, such as Kayser–Fleischer rings or severe neurological symptoms, can be prevented and, in future, may occur less frequently. Uncommon manifestations of Wilson’s disease include hypercalciuria and nephrocalcinosis, Figure 2. Roles of the Wilson ATPase (ATP7B) in hepatic copper transport. CPL, ceruloplasmin; CTR1, copper transporter 1; MT, metallothionein. chondrocalcinosis and osteoarthritis, sunflower cataracts and cardiac manifestations. The finding of a Kayser–Fleischer ring is a useful indicator of severe copper overload. If the ring is not detected by clinical inspection, the cornea should be examined under a slit lamp by an experienced ophthalmologist. Kayser–Fleischer rings are present in 95% of patients with neurological symptoms, in 50–60% of patients without neurological symptoms and in only 10% of asymptomatic siblings. Most patients with Wilson’s disease, whatever their clinical presentation or pre-symptomatic status, have some degree of liver disease. The most common age of hepatic manifestation is between 8 and 18 years; however, cirrhosis may be present in children below the age of 5 years, or may be diagnosed in patients presenting with advanced chronic liver disease in their fifties or sixties, without neurological symptoms and without Kayser–Fleischer rings. Liver disease may mimic all forms of common liver conditions, including asymptomatic transaminasaemia, acute or chronic hepatitis, fulminant hepatic failure and cirrhosis. Acute Wilsonian hepatitis and fulminant Wilson’s disease Figure 1. Schematic presentation of the Wilson ATPase (ATP7B). Acute Wilsonian hepatitis is indistinguishable from other forms of acute (viral or toxic) liver diseases. Kayser–Fleischer rings and neurological abnormalities may be absent in most patients. The disease may rapidly deteriorate and resemble fulminant hepatic failure. Large amounts of stored copper are released from necrotic hepatocytes and induce a severe haemolytic anaemia complicating acute liver disease. Although Wilson’s disease is rare, it accounts for 6–12% of patients with fulminant hepatic failure referred for emergency liver transplantation. Rapid diagnosis may Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 REVIEW: DIAGNOSIS AND THERAPY OF WILSON’S DISEASE be very difficult. Serum aminotransferase activity is usually less than 10 times normal and thus is much lower than the values commonly recorded in fulminant hepatitis of other aetiologies. The combination of anaemia, marked jaundice and relatively low aminotransferase activities in young patients should always raise the suspicion of acute Wilson’s disease.18, 19 An alkaline phosphatase to total bilirubin ratio below 2.0 has been claimed to provide 100% sensitivity and specificity for the diagnosis of Wilsonian fulminant liver failure, but this was not confirmed in larger series. The best diagnostic test is the quantification of copper in biopsy material or in the explanted liver. One puzzling feature of fulminant Wilson’s disease is the preponderance of females (female to male ratio, 3 : 1). Chronic hepatitis and cirrhosis due to Wilson’s disease Wilson’s disease may present with a clinical syndrome indistinguishable from chronic hepatitis or cirrhosis of other aetiology.20 Liver biopsy shows chronic hepatitis or advanced cirrhosis, but the diagnosis may be missed if the hepatic copper content is not measured. Without treatment, patients progressively deteriorate and may die of liver failure. Neuropsychiatric disease Neurological symptoms usually develop in the midteenage years or twenties.21 However, there are welldocumented cases of late (45–55 years) neurological disease. The initial symptoms may be very subtle, such as mild tremor and speech and writing problems, and are frequently misdiagnosed as behavioural problems associated with puberty. The hallmark of neurological Wilson’s disease is a progressive movement disorder characterized by dysarthria, dysphagia, apraxia and a tremor–rigidity syndrome (‘juvenile Parkinsonism’). About one-third of patients present with psychiatric abnormalities, such as reduced performance in school or at work, depression, labile mood, sexual exhibitionism and frank psychosis. Frequently, adolescents with problems in school or work are referred for psychological counselling and psychotherapy. Patients presenting with neurological symptoms may also suffer from significant liver disease. In a substantial proportion, symptomatic liver disease pre-dates the occurrence of neurological signs. In many patients with neurological disturbances, asymptomatic liver disease Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 159 can only be diagnosed by liver biopsy.22 However, if a liver biopsy is performed in all patients presenting with neurological symptoms at diagnosis, the proportion of patients with cirrhosis is 38.7%23 and about one-half of patients have only minimal liver disease. DIAGNOSIS The diagnosis of neurological Wilson’s disease is usually made on the basis of clinical findings and laboratory abnormalities (see Table 1). No additional tests are required if Kayser–Fleischer rings are present and/or serum ceruloplasmin levels are low.24 However, there are a few well-documented cases of neurological Wilson’s disease without Kayser–Fleischer rings.25 Clinical neurological examination is more sensitive than any other method for the detection of neurological abnormalities. Brain magnetic resonance imaging is useful for documenting the extent of changes in the central nervous system.26 The most common abnormalities are changes in the signal intensity of grey and white matter and atrophy of the caudate nucleus, brainstem and cerebral and cerebellar hemispheres. The diagnosis is more complex in patients presenting with liver diseases (see Figure 3). None of the commonly used parameters alone allows a certain diagnosis of Wilson’s disease. Usually, a combination of various laboratory parameters is necessary to firmly establish the diagnosis. Kayser–Fleischer rings may be absent in up to 50% of patients with Wilsonian liver disease and in an even higher proportion with fulminant Wilson’s disease. Serum ceruloplasmin may be in the low to normal range in up to 45% of patients with hepatic Wilson’s disease.27 On the other hand, even a low ceruloplasmin level is not diagnostic for Wilson’s disease in the absence of Kayser–Fleischer rings. Ceruloplasmin can be decreased in severely malnourished subjects and in heterozygous carriers of the Wilson’s disease gene.28 Very low levels were found in a patient with autoimmune hepatitis, which increased following steroid treatment. Ceruloplasmin is undetectable in familial aceruloplasminaemia. Thus, in patients with liver disease, a normal ceruloplasmin level cannot exclude Wilson’s disease, nor is a low level sufficient to make a diagnosis of Wilson’s disease. Ceruloplasmin is an acute phase reactant and its serum concentration increases as a consequence of inflammation. Most patients with marked liver disease have normal ceruloplasmin levels. An over-estimation of serum ceruloplasmin can be 160 P. FERENCI Table 1. Routine tests for the diagnosis of Wilson’s disease Test Typical finding False ‘negative’ False ‘positive’ Serum ceruloplasmin Decreased 24-h urinary copper > 100 lg/day Low levels in: malabsorption aceruloplasminaemia liver insufficiency heterozygotes Increased: hepatocellular necrosis contamination Serum ‘free’ copper > 10 lg/dL Hepatic copper > 250 lg/g dry weight Kayser–Fleischer rings by slit lamp Present Normal levels in patients with marked hepatic inflammation Over-estimation by immunological assay Normal: incorrect collection children without liver disease Normal if ceruloplasmin over-estimated by immunological assay Due to regional variation: in patients with active liver disease in patients with regenerative nodules In up to 40% of patients with hepatic Wilson’s disease In most asymptomatic siblings Cholestatic syndromes Primary biliary cirrhosis Figure 3. An algorithm for the diagnosis of Wilson’s disease. CPL, ceruloplasmin; KFR, Kayser–Fleischer rings. *Depends on availability. In Europe: H1069Q, exons 8 and 15. àEither at baseline or after d-penicillamine challenge. suspected if the serum copper concentration is lower than expected from the measured ceruloplasmin level (which contains 0.3% of copper). The ‘free’ copper concentration can be calculated by subtracting from the total copper concentration the ceruloplasmin-bound copper (ceruloplasmin times 3.3). An increased ‘free’ copper is not useful diagnostically, but can be employed as an adjunct to diagnosis, and is more important for monitoring the response to treatment. Urinary copper excretion is increased in patients with Wilson’s disease; however, its usefulness in clinical practice is limited. The estimation of urinary copper excretion may be misleading due to the incorrect collection of the 24-h urinary volume or to copper contamination. In pre-symptomatic patients, urinary copper excretion may be normal, but increases after d-penicillamine challenge.29 However, urinary copper excretion is also increased in any disease with extensive hepatocellular necrosis. The hepatic copper content is increased in 82% of patients with Wilson’s disease and usually exceeds 250 lg/g dry weight (normal, up to 50 lg/g dry weight). In the absence of other tests suggestive of abnormal copper metabolism, a diagnosis of Wilson’s disease cannot be made on the basis of an increased hepatic copper content alone. Patients with chronic Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 REVIEW: DIAGNOSIS AND THERAPY OF WILSON’S DISEASE cholestatic diseases, neonates and young children and possibly also subjects with exogenous copper overload have increased hepatic copper concentration of > 250 lg/g dry weight. In a recent study, we measured the hepatic copper content in 103 liver biopsies obtained at the diagnosis of Wilson’s disease, in 212 patients with a variety of non-cholestatic liver diseases (including 144 with chronic hepatitis C and 44 with non-alcoholic fatty liver disease), in 27 patients with chronic cholestasis and in 26 patients without evidence of liver disease.23 The liver copper content was > 250 lg/g dry weight in 85 (81%) Wilson’s disease patients, between 50 and 250 lg/g dry weight in 15 and in the normal range in four. The liver copper content did not correlate with age, grade of fibrosis or presence of stainable copper. The liver copper content was > 250 lg/g dry weight or between 50 and 250 lg/g dry weight in three (1.4%) and 20 (9.1%) of the 219 patients with non-cholestatic liver diseases, respectively. By lowering the cut-off from > 250 to 75 lg/g dry weight, the sensitivity of liver copper content for the diagnosis of Wilson’s disease increased from 81.2% to 96%, the negative predictive value increased from 88.2% to 97.1%, but the specificity (98.6% to 90.1%) and the positive predictive value (97.6% to 87.4%) decreased. It was concluded that, although liver copper content is a useful parameter, it neither proves or excludes Wilson’s disease with certainty. The diagnosis requires a combination of a variety of clinical and biochemical tests. Recently, a group of international experts has discussed this issue and has proposed a score based on a variety of tests and clinical symptoms.30 The validity of this score needs to be assessed prospectively. Liver biopsy findings are generally non-specific and are not helpful for the diagnosis of Wilson’s disease; however, the exclusion of other aetiologies may be equally important and may require a liver biopsy. The pathology includes early changes, such as fatty intracellular accumulations, which often proceed to marked steatosis. At later stages, portal and periportal lymphocytic infiltrates and the presence of necrosis and fibrosis may be indistinguishable from other forms of hepatitis. Some patients have cirrhosis without any inflammation. The detection of focal copper stores by the rhodanine stain is a pathognomonic feature of Wilson’s disease, but is only present in a minority (about 10%) of patients.31 The ultrastructural abnormalities include changes in mitochondria and peroxisomes and are stage specific. Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 161 Molecular genetic testing Mutation analysis for diagnosis is cumbersome because of the occurrence of many mutations, each of which is rare. Furthermore, most patients are compound heterozygotes (i.e. carry two different mutations). Direct mutation analysis for diagnosis is only helpful if a mutation occurs with a reasonable frequency in the population. In northern, central and eastern Europe,12, 14, 15 the most common mutations are: H1069Q mutation (allele frequency, 43.5%), mutations of exon 8 (6.8%), 3400delC (3%) and P969Q (1.6%).32 In other parts of the world, the pattern of mutations is different (Turkey, A1003T and P969Q;33 Sardinia, UTR -441/427del, 2463delC;34 Far East, R778L35, 36). Eventually, a multiplex polymerase chain reaction for the most frequent Wilson’s disease mutations in the region should make direct mutation analysis for diagnosis feasible and obtainable within a week. Family screening Once a diagnosis of Wilson’s disease is made in an index patient, an evaluation of his or her family is mandatory. The likelihood of finding a homozygote amongst the siblings is 25% and amongst the children 0.5%. Testing of second-degree relatives is only useful if the gene is found in one of the immediate members of the relative’s family. No single test is able to identify affected siblings or heterozygote carriers of the Wilson’s disease gene with sufficient certainty.37 Today, mutation analysis is the only reliable tool for screening the family of an index case with known mutations; otherwise haplotype analysis can be used. A number of highly polymorphic microsatellite markers that closely flank the gene allow the Wilson’s disease gene to be traced in a family.38 For such an analysis, at least one first-degree relative and the index patient are required. TREATMENT Treatments for Wilson’s disease have progressed from the intramuscular administration of dimercaprol (BAL) to the more easily administered oral penicillamine. Alternative agents to penicillamine, such as trientine, have been developed and introduced specifically for patients with adverse reactions to penicillamine. Zinc was developed separately, as was tetrathiomolybdate, which was used for copper poisoning in animals. 162 P. FERENCI Today, the mainstay of treatment for Wilson’s disease remains life-long pharmacological therapy, but the choice of drug mostly depends on the opinion of the treating physician and is not based on comparative data. According to the recent AASLD practice guidelines on Wilson’s disease, initial treatment for symptomatic patients should include a chelating agent (penicillamine or trientine).39 Treatment of pre-symptomatic patients and maintenance therapy of successfully treated symptomatic patients can be accomplished with the chelating agents penicillamine or trientine, or with zinc.39 Liver transplantation, which corrects the underlying hepatic defect in Wilson’s disease, is reserved for severe or resistant cases. Penicillamine Penicillamine is still the ‘gold standard’ for therapy.40 Penicillamine reduces copper bound to protein and thereby decreases the affinity of the protein for copper. Reduction of copper facilitates its binding to the drug. The copper mobilized by penicillamine is then excreted in the urine. Most symptomatic patients, whether hepatic, neurological or psychiatric, respond within months of starting treatment. Amongst neurological patients, a significant number may experience an initial worsening of symptoms before they get better. The usual dose of penicillamine is 1–1.5 g/day. Once the clinical benefit has been established, it is possible to reduce the dosage to 0.5–1 g/day. Initially, this dose will cause a large cupriuresis, but copper excretion later decreases to 0.5 mg/day. To prevent deficiency induced by penicillamine, pyridoxine (vitamin B6) should be supplemented (50 mg/week). A major problem of penicillamine is its high level of toxicity. In our series, 20% of patients had major side-effects and were switched to other treatments. Others report even higher frequencies of side-effects. There are two broad classes of penicillamine toxicity: direct, dose-dependent side-effects and immunologically induced lesions. Direct side-effects include pyridoxine deficiency and interference with collagen and elastin formation. The latter results in skin lesions such as cutis laxa and elastosis perforans serpingiosa. Immunologically mediated side-effects include leucopenia and thrombocytopenia, systemic lupus erythematodes, immune complex nephritis, pemphigus, buccal ulcerations, myasthenia gravis, optic neuritis and Goodpasture syndrome. Immunologically mediated side-effects require the immediate cessation of penicillamine. Trientine Trientine is a copper chelator, acting primarily by enhancing urinary copper excretion. Trientine is licensed for the treatment of Wilson’s disease and is as effective as penicillamine with far fewer sideeffects.41 However, the efficacy of trientine has not been compared with penicillamine as an initial treatment of Wilson’s disease. Anecdotal reports and our own experience indicate that trientine is a satisfactory first-line treatment for Wilson’s disease. Trientine appears to be more potent than penicillamine in the mobilization of copper, but cupriuresis diminishes more rapidly than with penicillamine. The cupriuretic power of trientine, however, is sufficient to keep the patient clinically well. Ammonium tetrathiomolybdate This drug has two mechanisms of action. First, it complexes with copper in the intestinal tract and thereby prevents the absorption of copper. Second, the absorbed drug forms a complex with copper and albumin in the blood and renders the copper unavailable for cellular uptake. The experience with this drug is very limited, but it appears to be useful for the initial treatment of patients with neurological symptoms.42 Zinc Zinc interferes with the intestinal absorption of copper by two mechanisms. Both metals share the same carrier in enterocytes and pre-treatment with zinc blocks this carrier for copper transport (with a half-life of about 11 days).43 The impact of the zinc-induced blockade of copper transport by other carriers into the enterocytes has not been studied. Second, zinc induces metallothionein in enterocytes, which acts as an intracellular ligand binding metals,44 which are then excreted in the faeces with desquamated epithelial cells. Indeed, the faecal excretion of copper is increased in patients with Wilson’s disease on treatment with zinc. Furthermore, zinc also induces metallothionein in the liver, protecting hepatocytes against copper toxicity.45 Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 REVIEW: DIAGNOSIS AND THERAPY OF WILSON’S DISEASE Data on zinc in the treatment of Wilson’s disease have been derived from uncontrolled studies using different zinc preparations (zinc sulphate, zinc acetate) at different doses (75–250 mg/day).46 The efficacy of zinc has been assessed by four different approaches. First, patients successfully decoppered by d-penicillamine were switched to zinc and the maintenance of their asymptomatic condition was monitored. Most patients maintained a negative copper balance and no symptomatic recurrences occurred. Some patients, however, died of liver failure after treatment was switched to zinc. Brewer et al. observed the occurrence of severe neurological symptoms in a 25-year-old asymptomatic sibling 4 months after switching from d-penicillamine to zinc.47 A second group includes symptomatic patients switched to zinc as an alternative treatment due to intolerance to d-penicillamine. 16 case histories have been published so far. Liver function and neurological symptoms improved in three and five patients, respectively. One patient further deteriorated neurologically and improved on re-treatment with d-penicillamine. The remaining patients remained in a stable condition. Follow-up studies in 141 patients have demonstrated that zinc is effective as sole therapy in the long-term maintenance treatment of Wilson’s disease.47 In a third group, zinc was used as first-line therapy.48 About one-third of patients were asymptomatic siblings of patients with Wilson’s disease and two-thirds presented with neurological or hepatic symptoms. Most patients remained free of symptoms or improved. In 15%, neurological symptoms worsened and improved on d-penicillamine. Three patients died of progressive liver disease. Finally, in a prospective study, in 67 newly diagnosed cases of Wilson’s disease, the efficacies of d-penicillamine and zinc were similar.49 Zinc was better tolerated than d-penicillamine. However, two zinc-treated patients died of progressive liver disease. Antioxidants Antioxidants, mainly vitamin E, may have a role as adjunctive treatment. Serum and hepatic vitamin E levels have been found to be low in Wilson’s disease.50 Symptomatic improvement when vitamin E is added to the treatment regimen has been reported occasionally, but no rigorous studies have been conducted. Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 163 Monitoring therapy If a decoppering agent is used for treatment, compliance can be tested by repeated measurement of the 24-h urinary copper excretion. This approach is not useful if patients are treated with zinc. If, in a compliant patient, urinary copper excretion decreases over time and stabilizes at < 500 lg/day, the dose of d-penicillamine can be lowered. The efficacy of treatment can be monitored by the determination of ‘free’ copper in serum and, depending on the presenting symptoms, liver disease can be assessed by routine liver function tests; repeated liver biopsies with measurement of hepatic copper content are not helpful. Improvement of neurological symptoms can be documented by clinical examination. In addition, some of the magnetic resonance imaging abnormalities are fully reversible on treatment. Auditory evoked brainstem potentials are also helpful to document improvement by decoppering treatment.51, 52 Liver transplantation Liver transplantation is the treatment of choice in patients with fulminant Wilson’s disease and in those with decompensated cirrhosis. In addition to improving survival, liver transplantation also corrects the biochemical defect underlying Wilson’s disease. However, the role of this procedure in the management of patients with neurological Wilson’s disease, in the absence of hepatic insufficiency, is still uncertain. Schilsky et al. analysed 55 transplants performed in 33 Wilson’s disease patients with decompensated cirrhosis and in 21 patients with Wilsonian fulminant hepatitis in the USA and Europe.53 The median survival after orthotopic liver transplantation was 2.5 years; the longest survival time after transplantation was 20 years. Survival at 1 year was 79%. Nonfatal complications occurred in five patients. Fifty-one orthotopic liver transplants were performed on 39 patients (16 paediatric, 23 adults) with Wilson’s disease at the University of Pittsburgh.54 The rate of primary graft survival was 73% and patient survival was 79.4%. Survival was better in those with chronic advanced liver disease (90%) than in those with fulminant hepatic failure (73%). In the Mayo Clinic series, the 1-year survival ranged from 79% to 87%, with an excellent chance for survival long term.55 The outcome of neurological disease following orthotopic 164 P. FERENCI liver transplantation is uncertain. In a retrospective survey, four of seven patients with neurological or psychiatric symptoms due to Wilson’s disease improved after orthotopic liver transplantation. Anecdotal reports document a dramatic improvement in neurological function within 3–4 months after orthotopic liver transplantation. In contrast, central pontine and extrapontine myelinolysis and new extrapyramidal symptoms developed in a patient 19 months after orthotopic liver transplantation.56 Some patients with psychiatric or neurological symptoms transplanted for decompensated cirrhosis have shown improvement of these symptoms following orthotopic liver transplantation.57 REFERENCES 1 Lee J, Pena MM, Nose Y, Thiele DJ. Biochemical characterization of the human copper transporter Ctr1. J Biol Chem 2001; 277: 4380–7. 2 Klomp AE, Tops BB, Van Denberg IE, Berger R, Klomp LW. Biochemical characterization and subcellular localization of human copper transporter 1 (hCTR1). Biochem J 2002; 364: 497–505. 3 Palmiter RD. The elusive function of metallothioneins. Proc Natl Acad Sci USA 1998; 95: 8428–30. 4 Kelley EJ, Palmiter RJ. A murine model of Menkes disease reveals a physiological function of metallothionein. Nat Genet 1996; 13: 219–22. 5 Rae T, Schmidt P, Pufahl R, Culotta VC, O’Halloran TV. Undetectable intracellular free copper: the requirement of a copper chaperone for superoxide dismutase. Science 1999; 284: 805–8. 6 Huffman DL, O’Halloran TV. Function, structure, and mechanism of intracellular copper trafficking proteins. Annu Rev Biochem 2002; 70: 677–701. 7 Hamza I, Schaefer M, Klomp LW, Gitlin JD. Interaction of the copper chaperone HAH1 with the Wilson disease protein is essential for copper homeostasis. Proc Natl Acad Sci USA 1999; 96: 13 363–8. 8 Larin D, Mekios C, Das K, Ross B, Yang AS, Gilliam TC. Characterization of the interaction between the Wilson and Menkes disease proteins and the cytoplasmic copper chaperone, HAH1p. J Biol Chem 1999; 274: 28 497–504. 9 Wernimont AK, Huffman DL, Lamb AL, O’Halloran TV, Rosenzweig AC. Structural basis for copper transfer by the metallochaperone for Menkes/Wilson disease proteins. Nat Struct Biol 2000; 7: 766–71. 10 Walker JM, Tsivkovskii R, Lutsenko S. Metallochaperone Atox1 transfers copper to the NH2-terminal domain of the Wilson’s disease protein and regulates its catalytic activity. J Biol Chem 2002; 277: 27 953–9. 11 Lutsenko S, Petris MJ. Function and regulation of the mammalian copper-transporting ATPases: insights from bio- 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 chemical and cell biological approaches. J Membr Biol 2003; 191: 1–12. Thomas GR, Forbes JR, Roberts EA, Walshe JM, Cox DW. The Wilson disease gene: spectrum of mutations and their consequences. Nat Genet 1995; 9: 210–7. Maier-Dobersberger T, Ferenci P, Polli C, et al. Detection of the His1069Gln mutation in Wilson disease by rapid polymerase chain reaction. Ann Intern Med 1997; 127: 21–6. Caca K, Ferenci P, Kuhn HJ, et al. High prevalence of the H1069Q mutation in East German patients with Wilson disease: rapid detection of mutations by limited sequencing and phenotype–genotype analysis. J Hepatol 2001; 35: 575–81. Firneisz G, Lakatos PL, Szalay F, Polli C, Glant TT, Ferenci P. Common mutations of ATP7B in Wilson disease patients from Hungary. Am J Med Genet 2002; 108: 23–8. Schaefer M, Hopkins R, Failla M, Gitlin JD. Hepatocyte-specific localization and copper-dependent trafficking of the Wilson’s disease protein in the liver. Am J Physiol 1999; 276: G639– 46. Tao YT, Gitlin JD. Hepatic copper metabolism: insights from genetic disease. Hepatology 2003; 37: 1241–7. McCullough AJ, Fleming CR, Thistle JL, et al. Diagnosis of Wilson’s disease presenting as fulminant hepatic failure. Gastroenterology 1983; 84: 161–7. Berman DH, Leventhal RI, Gavaler JS, Cadoff EM, Van Thiel DH. Clinical differentiation of fulminant wilsonian hepatitis from other causes of hepatic failure. Gastroenterology 1991; 100: 1129–34. Scott J, Gollan JL, Samourian S, Sherlock S. Wilson’s disease, presenting as chronic active hepatitis. Gastroenterology 1978; 74: 645–51. Oder W, Grimm G, Kollegger H, Ferenci P, Schneider B, Deecke L. Neurological and neuropsychiatric spectrum of Wilson’s disease. A prospective study in 45 cases. J Neurol 1991; 238: 281–7. Scheinberg IH, Sternlieb I. Wilson’s Disease. Vol. 23. Major Problems in Internal Medicine. Philadelphia: Saunders, 1984. Ferenci P, Steindl-Munda P, Vogel W, et al. Diagnostic value of quantitative hepatic copper determination in patients with Wilson disease. Lancet 2004 (in press). Sternlieb I. Perspectives on Wilson’s disease. Hepatology 1990; 12: 1234–9. Demirkiran M, Jankovic J, Lewis RA, Cox DW. Neurologic presentation of Wilson disease without Kayser–Fleischer rings. Neurology 1996; 46: 1040–3. van Wassenaer-van Hall HN, van den Heuvel AG, Algra A, Hoogenraad TU, Mali WP. Wilson disease: findings at MR imaging and CT of the brain with clinical correlation. Radiology 1996; 198: 531–6. Steindl P, Ferenci P, Dienes HP, et al. Wilson’s disease in patients presenting with liver disease: a diagnostic challenge. Gastroenterology 1997; 113: 212–8. Cauza E, Maier-Dobersberger Th, Ferenci P. Plasma ceruloplasmin as screening test for Wilson’s disease. J Hepatol 1997; 27: 358–62. Da Costa CM, Baldwin D, Portmann B, Lolin Y, Mowat AP, Mieli-Vergani G. Value of urinary copper excretion after Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 REVIEW: DIAGNOSIS AND THERAPY OF WILSON’S DISEASE 30 31 32 33 34 35 36 37 38 39 40 41 42 43 penicillamine challenge in the diagnosis of Wilson’s disease. Hepatology 1992; 15: 609–15. Ferenci P, Caca K, Loudianos G, et al. Diagnosis and phenotypic classification of Wilson disease. Final report of the Proceedings of the Working Party at the 8th International Meeting on Wilson Disease and Menkes Disease, Leipzig/Germany, 2001. Liver Int 2003; 23: 139–42. Ludwig J, Moyer TP, Rakela J. The liver biopsy diagnosis of Wilson’s disease. Am J Clin Pathol 1994; 102: 443–6. Ferenci P. Genotype–phenotype correlations in Wilson disease. J Hepatol 2002; 36(Suppl. 1): 158. Yurdaydin C, Demir K, Bozkaya H, et al. Mutation analysis in Turkish patients with Wilson disease. Hepatology 2003 (in press). Loudianos G, Dessi V, Lovicu M, et al. Molecular characterization of Wilson disease in the Sardinian population — evidence of a founder effect. Hum Mutat 1999; 14: 294–303. Kim EK, Yoo OJ, Song KY, et al. Identification of three novel mutations and a high frequency of the Arg778Leu mutation in Korean patients with Wilson disease. Hum Mutat 1998; 11: 275–8. Nanji MS, Nguyen VT, Kawasoe JH, et al. Haplotype and mutation analysis in Japanese patients with Wilson disease. Am J Hum Genet 1997; 60: 1423–6. Maier-Dobersberger Th, Rack S, Granditsch G, et al. Diagnosis of Wilson’s disease in an asymptomatic sibling by DNA linkage analysis. Gastroenterology 1995; 109: 2015–8. Cox DW. Molecular advances in Wilson disease. Prog Liver Dis 1996; 14: 246–64. Roberts EA, Schilsky ML. AASLD practice guidelines. A practice guideline on Wilson disease. Hepatology 2003; 37: 1475–92. Walshe JM, Yealland M. Chelation treatment of neurological Wilson’s disease. Q J Med 1993; 86: 197–204. Scheinberg IH, Jaffe ME, Sternlieb I. The use of trientine in preventing the effects of interrupting penicillamine therapy in Wilson’s disease. N Engl J Med 1987; 317: 209–13. Brewer GJ, Johnson V, Dick RD, Kluin KJ, Fink JK, Brunberg JA. Treatment of Wilson disease with ammonium tetrathiomolybdate. II. Initial therapy in 33 neurologically affected patients and follow-up with zinc therapy. Arch Neurol 1996; 53: 1017–25. Condomina J, Zornoza-Sabina T, Granero L, Polache A. Kinetics of zinc transport in vitro in rat small intestine and colon: interaction with copper. Eur J Pharm Sci 2002; 16: 289–95. Ó 2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 19, 157–165 165 44 Yuzbasiyan-Gurkan V, Grider A, Nostrant T, Cousins RJ, Brewer GJ. Treatment of Wilson’s disease with zinc. X. Intestinal metallothionein induction. J Lab Clin Med 1992; 120: 380–6. 45 Lee DY, Brewer GJ, Wang Y. Treatment of Wilson’s disease with zinc. VII. Protection of the liver from copper toxicity by zinc-induced metallothionein in a rat model. J Lab Clin Med 1989; 114: 639–45. 46 Ferenci P. Zinc treatment of Wilson’s disease. In: Kruse-Jarres JD, Schölmerich J, eds. Zinc and Diseases of the Digestive Tract. Lancaster: Kluwer Academic Publishers, 1997: 117– 24. 47 Brewer GJ, Dick RD, Johnson VD, Brunberg JA, Kluin KJ, Fink JK. The treatment of Wilson’s disease with zinc. J Lab Clin Med 1999; 134: 322–4. 48 Brewer GJ, Yuzbasiyan Gurkan V, Lee DY, Appelman H. Treatment of Wilson’s disease with zinc. VI. Initial treatment studies. J Lab Clin Med 1989; 114: 633–8. 49 Czlonkowska A, Gajda J, Rodo M. Effects of long-term treatment in Wilson’s disease with d-penicillamine and zinc sulphate. J Neurol 1996; 243: 269–73. 50 Sokol RJ, Twedt D, McKim JM Jr, et al. Oxidant injury to hepatic mitochondria in patients with Wilson’s disease and Bedlington terriers with copper toxicosis. Gastroenterology 1994; 107: 1788–98. 51 Grimm G, Madl Ch, Katzenschlager R, Oder W, Ferenci P, Gangl A. Detailed evaluation of brain dysfunction in patients with Wilson’s disease. EEG Clin Neurophysiol 1992; 82: 119–24. 52 Grimm G, Oder W, Prayer L, Ferenci P, Madl Ch. Prospective follow-up study in Wilson’s disease. Lancet 1990; 336: 963– 4. 53 Schilsky ML, Scheinberg IH, Sternlieb I. Liver transplantation for Wilson’s disease: indications and outcome. Hepatology 1994; 19: 583–7. 54 Bellary S, Hassanein T, Van Thiel DH. Liver transplantation for Wilson’s disease. J Hepatol 1995; 23: 373–81. 55 Eghtesad B, Nezakatgoo N, Geraci LC, et al. Liver transplantation for Wilson’s disease: a single-center experience. Liver Transpl Surg 1999; 5: 467–74. 56 Guarino M, Stracciari A, D’Alessandro R, Pazzaglia P. No neurological improvement after liver transplantation for Wilson’s disease. Acta Neurol Scand 1995; 92: 405–8. 57 Bax RT, Hassler A, Luck W, et al. Cerebral manifestation of Wilson’s disease successfully treated with liver transplantation. Neurology 1998; 51: 863–5.