Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of catecholamine research wikipedia , lookup
Menstrual cycle wikipedia , lookup
Mammary gland wikipedia , lookup
Breast development wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Triclocarban wikipedia , lookup
Endocrine disruptor wikipedia , lookup
Adrenal gland wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Growth hormone therapy wikipedia , lookup
Hypothalamus wikipedia , lookup
Hypothyroidism wikipedia , lookup
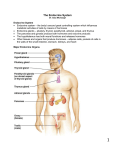
CHEMISTRY OF HORMONES Definition • Hormones are organic substances, produced in small amounts by specific tissues (endocrine glands), secreted into the blood stream to control the metabolic and biological activities in the target cells. • Hormones may be regarded as the chemical messengers involved in the transmission of information from one tissue to another and cell to cell. Chemical messengers • Endocrine hormones: – – – – produced by ductless endocrine glands mix to blood have target organs e.g. TH, LH, FSH • Autocrine hormones: – act on the same cells where they are synthesized. e.g. interleukin-2 • Paracrine hormones: – act on the cells adjacent/close to the cells from where they are synthesized e.g. prostaglandins • Neurotransmitters: – released by nerve cells and usually act on the adjacent cells. e.g. Catecholamines • Pheromones: – transmitted between the cells in the organisms of opposite sex – stimulates reproductive behavior and serve as sex attractants. CLASSIFICATION OF HORMONES 1. BASED ON CHEMICAL NATURE: Peptide hormones : Insulin Glucagon ADH Oxytocin Steroid hormones: Sex hormones Glucocorticoids Mineralocorticoids Amino acid derivatives: Epinephrine Norepinephrine Thyroid hormones 2. BASED ON MECHANISM OF ACTION GROUP I: intracellular receptor (Lipophilic) • Hormones bind to intracellular receptors (HRE in DNA) to form receptor hormone complexes to carry out the biochemical functions. They are derivatives of cholesterol, lipophilic in nature and possess long half lives. GROUP II: surface receptor (Hydrophilic) • These hormones bind to cell surface receptors and stimulate the release of second messengers which in turn perform the biochemical function. They are hydrophilic in nature and possess short half lives. Group-I hormones Hormones bind with HRE in DNA – Estrogens – Progestins – Androgens – Glucocorticoids – Mineralocorticoids – Calcitriol – Thyroid Hormones Group –II hormones (a) The second messenger is cAMP – – – – – – – – – – – – Adrenocorticotropic hormone (ACTH) Follicle stimulating hormone (FSH) Leuteinzing Hormone (LH) Thyroid stimulating hormone (TSH) Chorionic gonadotropins (hCG) Endorphins & Enkephalins Anti diuretic hormone (ADH) Glucagon Parathyroid hormone (PTH) Calcitonin Epinephrine Nor-epinephrine (b) The second messenger is cGMP – Atrial natriuretic factor (ANF) – Nitric oxide (NO) (c) The second messenger is phosphotidyl inositol/calcium (or both) – – – – Thyrotropin releasing hormone (TRH) Gonadotropin releasing hormone (GnRH) Gastrin Cholecystokinin (CCK) (d) The second messenger is unknown/ unsettled (Kinase/Phosphatase cascade) – – – – – Insulin Growth hormone (GH) Prolactin (PRL) Oxytocin Somatomedins (Insulin like growth factor) (IGF-I, IGF-II) MECHANISM OF HORMONE ACTION Group I Hormones – Lipophilic in nature cross plasma membrane by diffusion – Act through intracellular receptors located either in cytosol or nucleus – Duration of action is hours to days – Hormone first binds with receptor forms HR-complex binds with the specific region on the DNA called hormone responsive element (HRE) causes increased expression of specific genes transcription translation production of specific proteins carries biochemical action of hormone HRE HORMONE RESPONSE ELEMENT (HRE):– Specific sequence present in DNA which binds HR complex during lipophilic hormone action – HRE hormone specific RESULT:– Binding of HR complex to HRE transcription mRNA Translation (specific protein) Biochemical response Hormone receptor interaction: STRUCTURE OF RECEPTOR MOLECULES – Large, integral membrane proteins with specificity & high affinity for hormones. – Hormone & receptor binding is reversible. – Initiate response without entering the cell. – Rapid response/ shorter duration of action (seconds to hours). – Mediate effect through second messengers. MECHANISM OF HORMONE ACTION GROUP II HORMONES – These hormones are considered as first messenger – Hormone binds to surface receptors – Carry the action through mediatory molecules (second messengers) – Hormones First messenger Second messenger Activation of protein kinase phosphorylation of enzyme biochemical action. cAMP • Cyclic adenosine 3’,5’-monophosphate (cAMP) consists of adenine, ribose & a phosphate. • Adenylate cyclase converts ATP to cAMP • cAMP is a second messenger for majority of polypeptide hormones • cAMP binds with protein kinase and activates it to carry out the phosphorylation for the biochemical action of hormone • cAMP degrades to 5’ AMP by phosphodiasterase Thyroid hormones • Thyroid gland produces two principal hormones T4 (3,5,3’,5’-tetraiodothyronine) & T3 (3,5,3’-triiodothyronine) • Calcitonin, a hormone of calcium homeostasis is also produced by thyroid gland. Biosynthesis of T3 & T4 • • T3 & T4 are synthesized from tyrosine amino acid by the help of thyroglobulin Biosynthesis covers the following steps 1. Uptake of iodine 2. Formation of active iodine 3. synthesis of T3 & T4 Biosynthesis (contd…) • Uptake of iodine: – Iodide uptake is done by thyroid gland – Energy requiring process of Na+-K+ ATPase against concentration gradient (≈ 20:1) – Uptake is controlled by TSH • Formation of active iodine: – I- is converted to I+ by thyroid gland – Reaction requires H2O2 & catalyzed by thyroperoxidase Biosynthesis (contd…) • Synthesis of T3 & T4 : – Thyroglobulin is required to synthesize T3 & T4 – Thyroglobulin contains many tyrosine residues which serve as substrates for iodine to form thyroid hormones – Tyrosine becomes iodinated to form monoiodotyrosine (MIT) & diiodotyrosine (DIT) – MIT & DIT couple to form T3 and DIT & DIT to form T4 Storage & release of T3 & T4 • Thyroglobulin containing T3 & T4 can be stored in thyroid gland for several months • Can meet the body requirements for 1-3 months • T3 & T4 are released after proteolysis of thyroglobulin by lysosomes • MIT & DIT undergo deiodination by deiodinase and iodine may be reutilized Transport of T3 & T4 • Thyroxine binding globulin (TBG) & thyroxine binding prealbumin (TBPA) are responsible for transport • T3 is biologically more active than T4 Regulation of T3 & T4 synthesis • Synthesis is regulated by feedback regulation • Production of TSH by pituitary causes TRH production by hypothalamus which are inhibited by T3 • If T3 & T4 are less then TSH & TRH will be produced more and vice-versa • Normal thyroid secretion rate is – T4 = 100 g/day – T3 = 7 g/day – (Ratio of T4:T3 = 14:1 ) Biochemical functions of T3 & T4 1. Influence on the metabolic rate: – Stimulate metabolic activities & increases oxygen consumption 2. Effect on protein synthesis: – Promotes protein synthesis by acting at the transcriptional level. – Cause positive nitrogen balance & promotes growth and development 3. Influence on carbohydrate metabolism: – Promote intestinal absorption of glucose and its utilization – Promote hyperglycemia (↑gluconeogenesis & glycogenolysis) 4. Effect on lipid metabolism: – Stimulates lipid turnover and utilization Metabolic fate of T3 & T4 • They undergo deiodination in peripheral tissues • May get conjugated with glucuronic acid or sulphate in liver and excreted through bile • They may also form tetraiodothyroacetic acid ( from T4) and triiodothyroacetic acid (from T3) which then undergo conjugation and excretion. Abnormalities of thyroid function • Three abnormalities are known associated with thyroid hormones 1. Goiter 2. Hyperthyroidism 3. Hypothyroidism Goiter • Any abnormal increase in size of thyroid gland is goiter • Enlargement is mostly to compensate ↓ thyroid hormones & ↑ TSH • This is primarily due to a failure in the autoregulation of T3 & T4 synthesis • May be caused by deficiency or excess of iodine • Goitrogenic substances: thiocyanates, nitrates & percholates and drugs like thiourea, thiouracil, thiocarbamide etc. • Simple endemic goiter: due to iodine deficiency in diet. Mostly found in those geographical regions where iodine is less in soil & water Hyperthyroidism • Also known as thyrotoxicosis which is due to the overproduction of thyroid hormones and ↓TSH • Characterized by increased metabolic rate (↑ BMR), nervousness, irritability, anxiety, rapid heart rate, loss of weight, weakness, diarrhea, sweating, sensitivity to heat etc. • Caused by either Grave’s disease (↑ thyroid stimulating IgG) or increased intake of thyroid hormones • Diagnosed by scanning or thyroid hormones estimation Hypothyroidism • May be due to an impairment in the function of thyroid gland or disorders of pituitary or hypothalamus as a result there will be ↓ T3 & T4 level and ↑ TSH • Characterized by reduced BMR, slow heart rate, weight gain, sluggish behavior, constipation, sensitivity to cold, dry skin etc. • Cretinism (physical & mental retardation) in children and myxodema (bagginess under the eyes, puffiness of face, slowness in physical & mental activities) in adults. Thyroid function test • OBJECTIVES: – To assess the functional status of the gland. – To know anatomical features of thyroid gland. – To evaluate possible cause. – To confirm the biochemical response. – To assess treatment (complications). Serum TSH level • Normal serum TSH = 0.4 – 5.0 U/ml (<10 U/ml) • TSH in case of: – Primary hypothyroidism – Recovery from severe illness – Iodine deficiency (nontoxic goiter) – Pituitary tumor, etc • TSH in case of: – Hyperthyroidism – Exogenous thyroid hormone excess – Thyroiditis – First trimester of pregnancy Thyroxine (T4) • Serum T4 levels: – Serum total T4 (TT4) = 5-12μg/dL(65-156nmol/L) – Serum free T4 (FT4) = 0.8-2.4ng/dl(10-30pmol/L) • Interpretation: – Serum T4 ( > 12 g/dL) – Hyperthyroidism – Serum T4 ( < 2.5 g/dL) – Hypothyroidism Triiodothyronine (T3) • Serum T3 level: – Normal serum T3: 80–220ng/dL(1.2-3.3mmol/L) – Normal serum rT3: 30-80ng/dL(0.45-1.2nmol/L) • Interpretation: – Serum T3 ( > 300 ng/dL) Hyperthyroidism – Serum T3 ( < 70 ng/dL) Hypothyroidism