Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
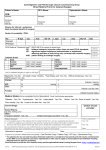
Ophthalmology Referral Form Referral should be made by FAX to the Patient Care Advisors Central Lancashire Patient Care Advisors Clinical Speciality: Assessment for Cataract Surgery FAX: 01772 769634 DOB Female Title: First Name: Patient Surname: Previous Surname: Patient Address: Male NHS No (if known): Post Code: Tel.(Daytime): Tel.(Evening): Mobile e-mail address (if known) Temporary Resident: Yes No Overseas Visitor: Yes No Yes No Language Spoken: Interpreter Required: Special Requirements: Referring Optometrist (PLEASE USE BLOCK CAPITALS) Council Registration Number: Name: Address: Registered GP Practice (if different) Name: Address: Post Code: TEL: Post Code: TEL: FAX: FAX: Please confirm the patient: Has A visually significant cataract Has Any Known Diabetic retinopathy Significant age-related Macular Degeneration Other significant ocular pathology Other retinal vascular disorders Corneal Pathology Glaucoma Amblyopia ANY ADDITIONAL INFORMATION Cataract (please circle) : Right / Left / Both eyes Patient’s visual status Current BEST corrected VA Current Refraction Previous VA if known Previous refraction if known Intra Ocular Pressure Right eye 6/ Left Eye 6/ 6/ 6/ …………mmHg ……….mmHg What symptoms is the patient having: Gradual reduction in vision Difficulty in activities of daily living Glare Monocular diplopia Date Where Appropriate Method of recording IOP NCT/Goldman/Perkins/OBF Has the patient been advised of the following? 1.Cataract surgery is only necessary if your quality of life is affected. 2.Cataract surgery is usually very successful but, as with any operation, complications may occur. There is a less than 1% chance of the vision being worse after surgery. Yes / No Has patient been given the “Choice” leaflet? Yes / No Has patient agreed to surgery and given verbal consent to providers having access to their patient information and clinical records. Yes/No Optometrist Signature: Administration section Date referral received: Date patient contacted PCA: Provider chosen: 582780293 Examination Date: PCT: PCA: Appointment date booked: