Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
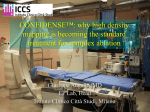
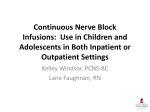
Review Article Rates of infection for single-lumen versus multilumen central venous catheters: A meta-analysis Cameron Dezfulian, MD; James Lavelle, MD; Brahmajee K. Nallamothu, MD, MPH; Samuel R. Kaufman, MA; Sanjay Saint, MD, MPH Objective: Since the introduction of multilumen central venous catheters two decades ago, there has been controversy whether the additional lumens place patients with these catheters at higher risk for infection. Our objective was to determine the risk of catheter-related bloodstream infection (CRBSI) and catheter colonization in multilumen catheters compared with single-lumen catheters. Data Source: Studies were identified by a computerized search of MEDLINE, EMBASE, CINAHL, Current Contents, and PREMEDLINE databases and by review of bibliographies and expert consultation. Studies comparing the prevalence of CRBSI or catheter colonization among single-, double-, and triple-lumen central venous catheters were included. We excluded studies if they included central venous catheters that were long-term, cuffed, tunneled, or coated with antibiotic or antiseptic agents. Data Abstraction: Two independent reviewers abstracted data on: 1) risk factors for CRBSI and colonization, 2) outcome definitions used, 3) the absolute prevalence of CRBSI and catheter colonization, and 4) study design and quality. Data Synthesis: A total of 15 studies met inclusion criteria. C atheter-related bloodstream infection (CRBSI) occurs commonly (1) in the United States, with a prevalence ranging from 3% to 7% (2–5). The attributable mortality of CRBSI is approximately 15%, and each episode is estimated to cost approximately $9,000 (2). Catheter colonization— or bacterial growth from the catheter tip without bac- From the Departments of Internal Medicine (CD, JL, BKN, SS) and Pediatrics (CD), University of Michigan, Ann Arbor, MI; Ann Arbor VA Health Services Research and Development Field Program, Ann Arbor, MI (SS); and the Patient Safety Enhancement Program, University of Michigan Health System, Ann Arbor, MI (SRK, SS). Dr. S. Saint is supported, in part, by a Career Development Award from the Health Services Research and Development Program of the Department of Veterans Affairs and a Patient Safety Developmental Center Grant from the Agency for Healthcare Research and Quality (P20-HS11540). Copyright © 2003 by Lippincott Williams & Wilkins DOI: 10.1097/01.CCM.0000084843.31852.01 Crit Care Med 2003 Vol. 31, No. 9 Summary odds ratios were calculated using a random-effects model. Although CRBSI was more common in multilumen catheters (summary odds ratios, 2.15; 95% confidence interval, 1.00 – 4.66), catheter colonization was not (summary odds ratios, 1.78; 95% confidence interval, 0.92–3.47). Tests for heterogeneity, however, suggested substantial variation by study. When only studies of higher quality were included, multilumen catheters were found not to be associated with a significant increase in CRBSI prevalence (summary odds ratios, 1.30; 95% confidence interval, 0.50 –3.41). Conclusions: Multilumen central venous catheters may be associated with a slightly higher risk of infection when compared with single-lumen catheters; however, this relationship diminishes when only high-quality studies that control for patient differences are considered. The slight increase in infectious risk when using multilumen catheters is likely offset by their improved convenience, thereby justifying the continued use of multilumen vascular catheters. (Crit Care Med 2003; 31:2385–2390) KEY WORDS: bactermia; central venous catheterization; indwelling catheters; cross infection; infection control; septicemia teremia— occurs in 20% of central venous catheters (2, 6, 7), with an estimated cost of almost $400 per episode (2). Despite these infectious complications, central venous catheters remain essential in the treatment of many hospitalized patients, especially the critically ill. Identifying modifiable risk factors for catheter-related infection is therefore crucial. The use of multilumen central venous catheters provides obvious advantages in patients who may require numerous intravenous medications, laboratory tests, blood product transfusions, and parenteral nutrition. Since their introduction two decades ago, triple-lumen catheters have become the preferred central venous catheters for patients requiring central venous access (6). Unfortunately, multilumen central venous catheters may lead to a higher rate of catheter colonization and CRBSI because of a higher frequency of catheter manipulations, with subsequent bacterial introduction; however, clinical trials directly comparing rates of CRBSI and catheter colonization between single- and multilumen catheters have yielded mixed results (8 –28). Accordingly, we performed a systematic and quantitative meta-analysis to compare the rates of CRBSI and catheter colonization in single-lumen vs. multilumen catheters. MATERIALS AND METHODS Study Design and Data Abstraction. We conducted a computerized search of the MEDLINE, CINAHL, Currents Contents, EMBASE, and PREMEDLINE databases. The exploded and focused “Medical Subject Headings” (MeSH) headings (or related text keywords) “catheterization” or “catheter” were combined with “infection” and, in MEDLINE, the floating subheading “adverse events.” The text words “single,” “double,” or “triple,” when found adjacent to the text word “lumen,” were then combined with the above results. A research librarian was consulted to ensure a thorough search. Titles and abstracts of all articles were scanned independently by two 2385 authors (C. Dezfulian, B. K. Nallamothu) and relevant articles identified. We also scanned bibliographies of retrieved articles and related review articles, and we contacted corresponding authors and experts to identify additional published or unpublished reports. Finally, the authors of all excluded articles containing potentially useful data were contacted in an effort to obtain these data. Criteria for Inclusion and Exclusion. Articles were included in the meta-analysis if they met the following criteria: 1) trials compared the rates of infection of at least two of the three different types of temporary central venous catheters (single-lumen catheters, double-lumen catheters, and triple-lumen catheters); and 2) the prevalence of catheter colonization or CRBSI was reported per catheter with sufficient data to calculate the odds ratio. We excluded studies that focused on hemodialysis catheters, peripherally inserted central venous catheters, pulmonary artery catheters or their introducer sheaths, and tunneled, cuffed, or antiseptic/ antibiotic– coated central venous catheters. Also excluded were studies in which the definition of CRBSI was unclear or overlapped with the definition of catheter colonization. In this event, attempts were made to contact corresponding authors to clarify these data and include them in the analysis. Definitions and Outcomes. Our primary outcome of interest was the prevalence of CRBSI by catheter type. To meet the definition of CRBSI in our analysis, studies were required to show isolation of the same organism from cultures of the catheter tip and blood. Catheter colonization, on the other hand, was defined as 1) the presence of bacterial growth from culture of the catheter tip in the absence of concomitant positive blood cultures for the same organism or 2) the presence of local purulence or cellulitis at the catheter insertion site, along with culture results from this site. The method of culturing catheter tips could be quantitative, semiquantitative, or qualitative. The qualitative culture method accepted any growth as positive. The semiquantitative method, based on the protocol of Maki et al. (29), required the growth of ⬎15 colonies per plate to be considered positive. The only use of purely quantitative cultures occurred in one study whose definition of CRBSI differed significantly from all others (16). In this study, catheters were identified as the source of bacteremia if cultures drawn through the lumen grew more than five times as many colonies as peripheral blood cultures in the absence of other anatomic sources for infection. Data Extraction. Data abstraction was performed independently by two authors (C. Dezfulian, J. Lavelle) using standardized forms. Data were abstracted on study design, study setting and population, the types of catheters used, the anatomic location and method of catheter insertion, duration of catheterization, type and frequency of site care performed, the use of total parenteral nutrition or systemic antimicrobial therapy, and the prevalence of catheter colonization and CRBSI. Disagree- 2386 ments among abstracters were resolved by discussion and ultimately arbitrated by a third author (S. Saint). Assessment of Study Design and Quality. Studies were assigned quality scores (A, B, or C) based on their methodology for the purposes of a sensitivity analysis. The quality score “A” was given to randomized, controlled trials because confounding by co-morbid conditions or severity of illness were thought to least likely affect this type of study design. The quality score “B” was given to prospective studies that demonstrated no statistically significant differences between the characteristics of their populations of patients. Although not randomized, these studies analyzed a number of known confounders and found no significant differences between groups that would bias the comparison of outcomes. All remaining studies received the quality score “C.” This group included prospective studies in which comparison of the patient groups revealed significant differences in one or more known CRBSI risk factors (i.e., femoral location of catheterization, duration of catheterization, use of total parenteral nutrition, patient severity of illness, emergent placement of catheters). Also included in group “C” were retrospective studies in which reliance on medical record review may have led to incomplete ascertainment of all catheterized patients during the study period. Statistical Analysis. Data on CRBSI and catheter colonization were analyzed separately. Separate pooled analyses were also performed for studies given different quality scores. In each of the included studies, the absolute risk of CRBSI and catheter colonization was calculated for all catheter types, along with corresponding standard deviations and 95% confidence intervals (CI). Summary odds ratios (OR) were calculated using the DerSimonian and Laird (30) method under a random-effects model. A random-effects model was chosen, given significant heterogeneity between the studies. All statistical analyses were performed using STATA 7.0 (College Station, TX) (31). RESULTS Study Characteristics. Our initial computerized search revealed 141 studies, 16 of which seemed to compare CRBSI or catheter colonization between two or more types of catheters. Four studies were excluded because they contained data from patients with excluded catheter types (pulmonary artery catheters, percutaneously inserted central catheters [peripherally inserted central venous catheters]) (23–25, 32). (The authors of these studies were contacted in an effort to obtain additional information on catheter types within the studies that met inclusion criteria. Unfortunately, this information was not available.) An additional two studies and one abstract were included after scanning bibliographies of the retrieved studies. Thus, a total of 15 studies were available for analysis (8 –22) and are summarized in Table 1. Most studies compared single- and triple-lumen catheters (12 of 15), placed catheters in the subclavian position (10 of 15), and gave total parenteral nutrition through one of the lumens (total parenteral nutrition was given in all studies; 8 of 15 gave total parenteral nutrition to all patients). Full barrier protection during catheter insertion was generally used, except in two studies (10, 22) in which only sterile gloves and drapes were used; data on barrier protection were unavailable in two other studies (8, 12). Of the 15 studies included in our analysis, six were randomized, controlled trials (quality score A), three were prospective studies with similar groups (quality score B), and the remaining six were either retrospective studies or prospective studies in which there were significant differences between groups (quality score C). Within the group B studies, patients were shown to be similar based on several of the characteristics in Table 1 and on either a review of patient diagnoses or comparison of formal clinical scores to assess the degree of illness of the patient populations. Thus, this subset of observational studies was assigned a higher quality score than the other observational studies (i.e., group C studies). Prevalence of CRBSI and Colonization. Table 2 summarizes the prevalence of CRBSI and catheter colonization, the method of catheter tip culture, and the definitions used for CRBSI. The intravascular catheter tip was usually cultured to establish infection at the site of insertion; in some studies (11, 13), however, local wound culture was also accepted. Studies usually required the presence of fever and occasionally other signs and symptoms of infection (such as elevated white blood cell count, chills, or pus at the catheter insertion site) as part of their definition. Some studies also required resolution of these signs and symptoms after removal of the catheter or the absence of other possible sites of infection. Occasionally, studies were more flexible in their definition of CRBSI, allowing for culture of the blood to be different from that of the catheter site or negative altogether. In these situations, the symptoms of infection had to resolve after removal of the catheter, and in some studies, no other Crit Care Med 2003 Vol. 31, No. 9 Table 1. Summary of studies included in analysis First Author’s Last Name (Ref. No.) Quality score Types of catheters being compared Pomp (8) Farkas (9) Yeung (10) Miller (11) Powell (12) Goetz (13) Ma (14) Kemp (15) Clark (16) Johnson (17) Gil (18) Pemberton (19) McCarthy (20) Lee (21) Rose (22) C SLC TLC A SLC TLC C SLC TLC B SLC TLC A SLC DLC C SLC TLC A DLC TLC C SLC DLC TLC A SLC TLC A SLC DLC B SLC TLC C SLC TLC A SLC TLC B SLC TLC C SLC TLC Y Y Y Y NR N Y Y Y N N NR Y NR Y Y NR Y Y N Y Y NR Y Y NR Y Y NR Y Y NR Y Y Y Y N N Y Y NR N 39 61 100 100 100 46 24 30 80 20 68 26 6 7.46 100 NR 39 54 7 NR 100 Mostly Rarely 100 Catheters placed de novo Initially Y Subsequently N Full barrier technique NR used Anatomic location of catheter placement, % Subclavian NR Internal jugular Femoral Mean duration of catheterization, days SLC DLC TLC 3 to 4 TPN given (proportion), % Y (NR) SLC DLC TLC 11.6 4.6 3.0 9.1 Y 98 14.7 Y 10 3.0 Y 100 98 35 100 NR 8.2 16.0 14.5 Y 10.0 Y 20 Y 100 100 Y 100 100 100 100 100 39 13.66–14.36 24.1 NR NR NR 9.5 11.4 20.5 Y 100 100 100 Y 100 100 100 Y (52) Y 100 8.5 Y 100 11.2 Y 100 100 100 100 Y (42) A, B, C, quality scores were assigned to each study as described in the METHODS section; SLC, DLC, TLC, single, double, triple lumen catheters, respectively; NR, data not reported. Key characteristics abstracted from the 15 studies included in the analysis are summarized above. Table 2. Prevalence of catheter-related bloodstream infections (CRBSI) and catheter colonization First Author’s Last Name (Ref. No.) Quality score Method of culture Definition of CRBSI Signs of infection Resolution of symptom Positive catheter culture Positive blood culture No other source of infection Prevalence of CRBSI (%) SLC Pomp Farkas Yeung Miller Powell (8) (9) (10) (11) (12) C NR A L ⫹ ⫹ ⫹ ⫹ Prevalence of colonization (%) SLC Kemp (15) C SQ A SQ C SQ A Q A SQ B SQ C NR ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⌬ ⫹ ⌬ ⫹ ⫹ 2/78 (2.6) B L A L ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ 8/617 (1.3) 5/68 (7.4) 3/1936 1/10 (0.15) (10.0) 2/22 (9.1) 0/22 (0) 4/165 (2.4) 7/595 (1.2) 5/61 (8.2) 18/495 (3.6) 2/27 (7.4) 18/68 5/1936 3/10 (26.5) (0.26) (30.0) DLC TLC Ma (14) C SQ DLC TLC Goetz (13) 14/61 16/495 14/27 (23.0) (3.2) (51.8) 4/130 (3.1) 1/22 (4.5) 0/22 (0) 21/165 (12.7) 15/130 (11.5) 0/6 (0) 1/49 0/18 (2.0) (0) 1/52 37/373 (1.9) (9.9) Clark-Cristoff Johnson (16) (17) Lee (21) Rose (22) A SQ B SQ C NR ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⌬ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ 0/48 (0) 0/51 (0) 5/63 (7.9) 2/68 (3) 0/36 (0) 0/68 (0) 4/248 (1.6) 6/157 (3.8) 11/59 (18.6) 4/39 (10.3) 4/307 (1.3) 12/232 (4.9) 10/63 (15.8) 2/68 (2.9) 0/36 (0) 3/68 (4.4) 32/157 (20.3) 3/59 (5.1) 1/39 (2.6) 32/307 (10.4) 13/99 (13.1) 1/48 (2.1) 1/51 (2.0) Gil (18) Pemberton McCarthy (19) (20) ⫹ A, B, C, quality scores were assigned to each study as described in the METHODS section of the text; NR, data were not reported; methods of culture were qualitative (L), semiquantitative (SQ), or quantitative (Q); ⌬, studies that were more flexible in their definition of CRBSI; SLC, DLC, TLC, single, double, triple lumen catheters, respectively. For each study, the method of culture, the definition of CRBSI, and the number of infected catheters/total number of catheters (with percentage) are given. Crit Care Med 2003 Vol. 31, No. 9 2387 source of infection could be present (14, 15, 17). It was impossible in these cases to discern which of the CRBSI diagnoses were made with this alternative definition, and therefore, the numbers provided by the authors had to be accepted. Summary OR of CRBSI and Catheter Colonization. For both end points, double-lumen catheters made up only 2% of the total catheters analyzed and were therefore grouped together with triplelumen catheters as multilumen catheters when calculating summary ORs. Alternative groupings were also analyzed and revealed no difference between several possible permutations because of the small number of double-lumen catheters. Likewise, calculation of ORs comparing only triple-lumen catheters with singlelumen catheters yielded no qualitative differences in the results and required exclusion of two A-quality studies that were thought to be valuable in the overall meta-analysis (analyses not shown). Figures 1 and 2 summarize the OR for CRBSI and catheter colonization when comparing multilumen catheters with single-lumen catheters. The OR for CRBSI could not be calculated for one study that did not have a single-lumen catheter group (14) and for another study in which the absolute rate of CRBSI was zero for both single- and double-lumen catheters (17). When the remaining studies were included in the analysis, the summary OR for CRBSI was 2.15 (95% CI, 1.00 – 4.66) and, for colonization, 1.78 (95% CI, 0.92–3.47), in both cases reflecting a higher risk of infection for multilumen catheters. When the analysis was limited to higher-quality studies (quality scores A and B), the OR for CRBSI was 1.30 (95% CI, 0.50 –3.41) and, for colonization, 1.30 (95% CI, 0.82–2.07). The test for heterogeneity was significant (p ⫽ .001 for CRBSI, p ⫽ .004 for colonization) when all studies were included in the analysis but not when only higherquality studies were analyzed (p ⫽ .11 for CRBSI, p ⫽ .67 for colonization). Sensitivity Analysis. Summary ORs for both outcomes were calculated excluding each study individually. The exclusion of the study by Yeung et al. (10) (quality score C) had the most significant effect on the summary OR for both outcomes (summary OR for CRBSI, 1.64 [95% CI, 0.89 –3.00]; for colonization, 1.21 [95% CI, 0.82–1.76]). Review of this study revealed the reported absolute prevalence of both CRBSI (0.15%) and colonization (0.26%) were far lower than 2388 Figure 1. Analysis of catheter-related bloodstream infections in (A) all studies and (B) only higher-quality studies. The diamond indicates the summary odds ratio (OR) and 95% confidence interval (CI). Studies are listed sequentially by study reference number. The size of the squares is proportional to the weight of the studies (inverse variance). similar outcomes reported in the other studies (Table 2) or in the literature (1, 5, 6, 33). Exclusion of this study alone made the test for heterogeneity for both outcomes insignificant (p ⫽ .41 and p ⫽ .63 for CRBSI and colonization, respectively). The next most influential study when excluded was that by Pemberton et al. (19) (quality score C), which had a similar, albeit lesser, effect on the tests for heterogeneity and the summary OR for both outcomes. The study by Miller et al. (11) involved a relatively small number of patients (n ⫽ 37), and we therefore questioned whether this study had sufficient statistical power to detect meaningful baseline clinical differences between patients in the single-lumen and multilumen catheter groups. Although this study was assigned a quality score of B in the base case analysis, we repeated our analyses using a quality score of C for this study. The quality score assignment had little effect on the summary ORs or the CIs (data not shown). DISCUSSION We performed a systematic, evidencebased review that used meta-analysis to quantify the risk of CRBSI and catheter colonization in temporary multilumen Figure 2. Analysis of catheter colonization in (A) all studies and (B) only higher-quality studies. The diamond indicates the summary odds ratio (OR) and 95% confidence interval (CI). Studies are listed sequentially by study reference number. The size of the squares is proportional to the weight of the studies (inverse variance). central venous catheters when compared with single-lumen central venous catheters. We summarized data from 15 studies using a random-effects model. Our results suggested an apparent increase in CRBSI and a trend toward more catheter colonization in multilumen catheters. Tests for heterogeneity, however, demonstrated significant variation across the results of these studies. Importantly, exclusion of lower-quality studies diminished the relationship between infection rate and multilumen catheters. An earlier review by Farkas et al. (9) suggested similar results, noting a bias toward “sicker” patients receiving triplelumen catheters. Gil et al. (18) also considered this potential bias in observational studies and attempted to compensate for it by using the Acute Physiology Scoring System to show similarity between their patient groups. Neither study, however, provided quantitative results to verify this bias nor did they systematically review the literature to find all relevant studies. Our comprehensive analysis expands on the work of these authors and others and clarifies much of the variability found in previous individual studies. It has been suggested that increased manipulations of central venous catheters contributes to higher rates of CRBSI Crit Care Med 2003 Vol. 31, No. 9 (34). Clark-Cristoff et al. (16), in a randomized trial, found a higher risk of CRBSI in triple-lumen compared with single-lumen catheters. In their study, the investigators reported “additional lumens of the triple-lumen catheters were accessed from 15 to 20 times a day for administration of drugs and for blood sampling.” They concluded this was likely to be responsible for the increased risk of infection. Although their study was randomized and prospective, the catheters used remained in place on average twice as long as in other studies, and their method of catheter tip culture was unique. Furthermore, their measured prevalence of CRBSI in multilumen catheters (13.1%) was significantly higher than that reported in other randomized, controlled trials (35). Another possible reason for the observed increase in CRBSI and colonization prevalence found in observational studies of multilumen catheters would be their use for a longer period of time compared with single-lumen catheters. The relationship between infection and duration of catheterization is clear (3). Our present study is unable to evaluate this hypothesis because most of the studies reported the prevalence of infections as episodes per catheter rather than episodes per catheter-day. In the studies in which the duration of catheterization was reported (Table 1), the duration between the two groups is roughly comparable. A recent meta-analysis of randomized trials comparing antibiotic-coated and uncoated triple-lumen catheters revealed rates of CRBSI in the uncoated triple lumen group to range from 2.1% to 11.7% (35), which is very similar to the rate of CRBSI in triple-lumen catheters found in our study. This range also includes the range of single lumen CRBSI found in this study, and it is not surprising that the difference between the two types of catheters is not statistically significant. The studies in which the OR for CRBSI in multilumen catheters tended to be the greatest have either excessively high (⬎10%) rates of CRBSI in multilumen catheters (16, 19, 20) or a low rate of CRBSI in the single-lumen catheters (10) when compared with published values of CRBSI in the literature (35). Two high-quality studies cited in this analysis compared double- and singlelumen catheters. In both, the prevalence of CRBSI and colonization in doublelumen catheters was either less than (12) or the same as (17) in single-lumen cathCrit Care Med 2003 Vol. 31, No. 9 eters. The latter study could not be included in our summary OR because of the absence of infection in both groups. Within these studies, increased manipulation of a double-lumen catheter’s extra lumen—in contrast to triple-lumen catheters— did not significantly increase the risk for CRBSI. This is inconsistent with the hypothesis that additional lumens yield increased infection because of increased manipulations. In addition, one high-quality study comparing doubleand triple-lumen catheters, which also could not be included in our metaanalysis for lack of a control (singlelumen catheter) group, demonstrated no significant difference in CRBSI between these two groups (14). Most studies recruited any medical or surgical inpatients needing a central venous catheter or total parenteral nutrition. Thus, a significant proportion of non–intensive care unit patients were included. Only the studies of Farkas et al. (9) and Gil et al. (18) explicitly stated they recruited only intensive care unit patients, and the prevalence of catheter infections were similar in both groups compared in both studies (Table 2). Only the studies of Ma et al. (14), Pemberton et al. (19), and McCarthy et al. (20) reported the proportion of patients in the intensive care unit. The studies of Ma et al. (14) and McCarthy et al. (20) were both randomized, controlled trials (quality A), and similar proportions of patients were in the intensive care unit in both catheter groups (Ma et al., 23 [62%] patients with double-lumen catheters and 28 [67%] with triple-lumen catheters; McCarthy et al., 21 [58%] patients with single-lumen catheters and 22 [56%] with triple-lumen catheters). Ma et al. (14) found no difference in infection rates between double and triple-lumen catheters, whereas McCarthy et al. (20) found a higher rate of CRBSI and colonization in triple vs. single-lumen catheters. The study by Pemberton et al. (19) was prospective but not randomized (quality C), and significantly more patients in the triple-lumen– catheter group were in the intensive care unit (32 patients, 78%) vs. those with single-lumen catheters (22 patients, 39%). In addition, these triple-lumen– catheter patients had higher rates of mortality, malnutrition, and major surgery. This study found a higher rate of CRBSI in triple-lumen catheters vs. singlelumen catheters. We found that the risk of CRBSI and catheter colonization for multilumen T he slight increase in infectious risk when using multi- lumen catheters is likely offset by their improved convenience, thereby justifying the continued use of multilumen vascular catheters. catheters was greater than for singlelumen catheters, but this difference was not statistically significant after accounting for differences in the quality of the individual studies. Even if the upper limit of the 95% CI was taken as the actual effect size (a conservative estimate), then the 3.4-fold increased risk of CRBSI and 2-fold increased risk of catheter colonization in multilumen catheters must be weighed against the risks of increased mechanical complications associated with the placement of multiple singlelumen catheters. When Powell et al. (12) randomized patients to receive one double-lumen catheter vs. two single-lumen catheters, they found a 3-fold increase in the rate of mechanical complications (13.6% vs. 4.5%) in the single-lumen group. Misny et al. (28), in a retrospective study published only in abstract form, likewise found a higher rate of pneumothorax (3.0% vs. 0.5%) and thrombosis (1.1% vs. 0.5%) and a higher rate of “primary sepsis” (1.5% vs. 0.5%) in singlelumen catheters when compared with triple-lumen catheters. Unfortunately, the authors of this study could not be located to clarify their definitions of catheter-related sepsis, and therefore, the study could not be included in our analysis. The effects of the higher rate of mechanical complications involved in the placement of one or more single-lumen catheter instead of a single multilumen catheter would likely counterbalance any savings in CRBSI. CONCLUSIONS Meta-analyses have a number of limitations compared with large controlled trials (36, 37); however, the cost of a randomized, controlled trial adequately powered to definitely answer the question 2389 of whether multilumen catheters cause more infectious complications than single-lumen catheters would be high. Our data demonstrate it is unlikely that there is a substantial increase in the risk of CRBSI or catheter colonization when multilumen catheters are used instead of single-lumen catheters. The controversy regarding this issue likely stems from poorly controlled prospective or retrospective observational studies that have implicated multilumen catheters as a risk factor for infection. Our analysis reveals that the bulk of standardized, wellcontrolled studies comparing similar patient groups indicate multilumen catheters are not a significant risk factor for increased bloodstream infections or local catheter colonization when compared with single-lumen catheters. ACKNOWLEDGMENTS We thank Gurpreet K. Rana, MLIS, research librarian at the University of Michigan Taubman Medical Library, for her assistance with devising the search strategy; Kathleen Welch, MA, MPH, and Myra Kim, ScD, of the University of Michigan Center for Statistical Consultation and Research for statistical support; Carlos H. Ramirez-Ronda, MD, MACP, Horace F. Henriques III, MD, FACS, Louis Flancbaum, and Debra S. Kovacevich, RN, MPH, for providing additional information about their publications; Carol E. Chenoweth, MD, Benjamin A. Lipsky, MD, FACP, FIDSA, and Michele L Pearson, MD, for acting as experts in evaluating the completeness of the literature search strategy; and Catherine Gage Michalak, MS, RN, for providing us information on catheter purchases within the University of Michigan Health System. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. REFERENCES 16. 1. Mermel LA: Prevention of intravascular catheter-related infections. Ann Intern Med 2000; 132:391– 402 2. Saint S, Veenstra DL, Lipsky BA: The clinical and economic consequences of nosocomial central venous catheter-related infection: Are antimicrobial catheters useful? Infect Control Hosp Epidemiol 2000; 21:375–380 3. Maki DG: Infections caused by intravascular devices used for infusion therapy. In: Infections Associated with Indwelling Medical Devices. Bisno AL, Waldvogel FA (Eds). Washington, DC, ASM Press, 1994, pp 155–205 4. Veenstra DL, Saint S, Sullivan SD: Costeffectiveness of antiseptic-impregnated cen- 2390 17. 18. 19. 20. tral venous catheters for the prevention of catheter-related bloodstream infection. JAMA 1999; 282:554 –560 Kaufman JL, Rodriguez JL, McFadden JA, et al: Clinical experience with the multiple lumen central venous catheter. JPEN J Parenter Enteral Nutr 1986; 10:487– 489 Apelgren KN: Triple lumen catheters: Technological advance or setback? Am Surg 1987; 53:113–116 Richet H, Hubert B, Nitemberg G, et al: Prospective multicenter study of vascularcatheter–related complications and risk factors for positive central-catheter cultures in intensive care unit patients. J Clin Microbiol 1990; 28:2520 –2525 Pomp A, Varella L, Caldwell MD, et al: Catheterrelated sepsis: Single lumen catheters (SLC) vs. triple lumen catheters (TLC). JPEN J Parenter Enteral Nutr 1988; 12:23S, Abstract 122 Farkas JC, Liu N, Bleriot JP, et al: Single- versus triple-lumen central catheter–related sepsis: A prospective randomized study in a critically ill population. Am J Med 1992; 93:277–282 Yeung C, May J, Hughes R: Infection rate for single lumen v triple lumen subclavian catheters. Infect Control Hosp Epidemiol 1988; 9:154 –158 Miller JJ, Venus B, Mathru M: Comparison of the sterility of long-term central venous catheterization using single lumen, triple lumen, and pulmonary artery catheters. Crit Care Med 1984; 12(8):634 – 637 Powell C, Fabri PJ, Kudsk KA: Risk of infection accompanying the use of single-lumen vs. double-lumen subclavian catheters: A prospective randomized study. JPEN J Parenter Enteral Nutr 1988; 12:127–129 Goetz AM, Wagener MM, Miller JM, et al: Risk of infection due to central venous catheters: Effect of site of placement and catheter type. Infect Control Hosp Epidemiol 1998; 19:842–845 Ma TY, Yoshinaka R, Banaag A, et al: Total parenteral nutrition via multilumen catheters does not increase the risk of catheterrelated sepsis: A randomized, prospective study. Clin Infect Dis 1998; 27:500 –503 Kemp L, Burge J, Choban P, et al: The effect of catheter type and site on infection rates in total parenteral nutrition patients. JPEN J Parenter Enteral Nutr 1994; 18:71–74 Clark-Cristoff N, Watters VA, Sparks W, et al: Use of triple-lumen subclavian catheters for administration of total parenteral nutrition. JPEN J Parenter Enteral Nutr 1992; 16:403–407 Johnson BH, Rypins EB: Single-lumen vs double-lumen catheters for total parenteral nutrition. Arch Surg 1990; 125:990 –992 Gil RT, Kruse JA, Thill-Baharozian MC, et al: Triple- vs single-lumen central venous catheters. Arch Intern Med 1989; 149:1139 –1143 Pemberton LB, Lyman B, Lander V, et al: Sepsis from triple- vs. single-lumen catheters during total parenteral nutrition in surgical or critically ill patients. Arch Surg 1986; 121:591–594 McCarthy MC, Shives JK, Robison RJ, et al: Pro- 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. spective evaluation of single and triple lumen catheters in total parenteral nutrition. JPEN J Parenter Enteral Nutr 1987; 11:259–262 Lee RB, Buckner M, Sharp KW: Do multilumen catheters increase central venous catheter sepsis compared to single-lumen catheters? J Trauma 1988; 28:1472–1475 Rose SG, Pitsch RJ, Karrer FW, et al: Subclavian catheter infections. JPEN J Parenter Enteral Nutr 1988; 12:511–512 Henriques HF III, Karmy-Jones R, Knoll SM, et al: Avoiding complications of long-term venous access. Am Surg 1993; 59:555–558 Lugo LJ, Zapata NJ, Ramirez-Ronda CH: Catheter related infections in Damas hospital. Bol Asoc Med P R 86(4 – 6):37– 41, 1994 Hilton E, Haslett TM, Borenstein MT, et al: Central catheter infections: Single- versus triplelumen catheters. Am J Med 1988; 84:667–672 Eyer S, Brummitt C, Crossley K, et al: Catheterrelated sepsis: Prospective, randomized study of three methods of long-term catheter maintenance. Crit Care Med 1990; 18:1073–1079 Kovacevich DS, Faubion WC, Braunschweig CL, et al: Prevalence of catheter sepsis in parenteral nutrition patients with triple lumen vs. single lumen catheters. Abstr. JPEN J Parenter Enteral Nutr 1988; 12:23S, Abstract 123 Misny P, Srp F, Marein C, et al: Complications of single lumen (SLC) versus multilumen (MLC) temporary central venous catheters (TCVC) for total parenteral nutrition (TPN). JPEN J Parenter Enteral Nutr 1986; 17S, Abstract 86 Maki DG, Weise CE, Sarafin HW: A semiquantitative culture method for identifying intravenous catheter-related infection. N Engl Med 1977; 296:1305–1309 DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials 1986; 7:177–188 Bradburn MJ, Deeks JJ, Altman DG: metan: An alternative meta-analysis command. Stata Tech Bull 1998; 44(sbe24):4 –15 Savage AP, Picard M, Hopkins CC, et al: Complications and survival of multilumen central venous catheters used for total parenteral nutrition. Br J Surg 1993; 80:1287–1290 Mantese VA, German DS, Kaminski DL, et al: Colonization and sepsis from triple-lumen catheters in critically ill patients. Am J Surg 1987; 154:597– 601 Viale P, Politi E, Sisti M, et al: Impact of central venous catheters (CVC) management on infectious risk. Abstr. J Hosp Infect 1998; 40(Suppl A):8.1.8 Veenstra DL, Saint S, Saha S, et al: Efficacy of antiseptic-impregnated central venous catheters in preventing catheter-related bloodstream infection. JAMA 1999; 281:261–267 Lelorier J, Gregoire G, Benhaddad A, et al: Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N Engl J Med 1997; 8:536 –542 Ioannidis JPA, Cappelleri JC, Lau J: Issues in comparisons between meta-analyses and large trials. JAMA 1998; 279:1089 –1093 Crit Care Med 2003 Vol. 31, No. 9