Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
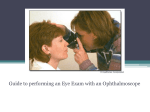
Delhi Journal of Ophthalmology Instrument Scan Understanding your Direct Ophthalmoscope Digvijay Singh, Rohit Saxena, Pradeep Sharma, Vimla Menon Dr. R.P. Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India The direct ophthalmoscope is an extremely important examination tool not only for ophthalmologists but for physicians as well. It is probably the only tool in ophthalmology that can help perform a complete ocular examination. This article highlights the development, functioning and use of direct ophthalmoscopes. A peak in the past Scientists had tried to peer into the then unknown back of the eye in the 18th and 19th century but were unsuccessful in understanding and establishing a coaxial illumination observation system. Then in the mid 19th century, several scientists noticed that if they kept a light source (pointed at the subject) very near their eye, then in some cases (emmetropes) they could view the red reflex and retina. It was in 1849 that Charles Babbage made what was probably the first practical ophthalmoscope.[1] (Figure 1). It was a simple piece of mirror with a silver patch rubbed off from the centre to make it see-through. Shortly afterwards, in 1851, Hermann Von Helmholtz published a monograph describing in detail the optical working of an ophthalmoscope and a designed a practical ophthalmoscope very similar to the ones used today. (Figure 2) Helmholtz is recognized as the inventor of the direct ophthalmoscope. An anecdote in this regard is that when Helmholtz tried to interest the king’s physician in his newly invented ophthalmoscope, he was told that it had no value as every known disease of the eye could already be diagnosed without it. Around the same time, the ophthalmoscope gave Helmholtz an instant global fame in the field of optics. Figure 1: Babbage and his ophthalmoscope DJO 40 Figure 2: Helmholtz and his ophthalmoscope Instrument detailing Currently, the ophthalmoscope comes in various sizes and modifications though all follow the same optical principle. Initially we describe in detail a standard direct ophthalmoscope and later look at the variants available with their specific advantages[2]. (Figure 3) Figure 3: Detailed instrument scheme for the direct ophthalmoscope Vol. 21, No. 3, January-March, 2011 Delhi Journal of Ophthalmology Understanding your Direct Ophthalmoscope The ophthalmoscope consists of a metallic optical tube, usually made of a durable light weight metal such as chromeplated brass for proper alignment of the contents. Inside this tube, glass condensing lens, objective lens, mirror/prism aperture dial assembly, red-free/polarizer assembly and lamp are sealed. The aperture dial is mounted such that it maintains alignment despite a fall/accidental drop from a reasonable height. as a clinical science existed well before the development of the ophthalmoscope as is exemplified by the founding of Moorfields eye hospital in 1804 and many others[3]. Illumination system • Incandescent lamp: This is usually a xenon halogen bright white lamp powered by a 2.5V non-rechargeable or 3.5V [NiMH (Nickel Metal Hydride) or LiION(Lithium ion)] rechargable battery. • Condensing lens: There are two condensing lens, one on either side of the aperture dial which focus the light onto the mirror/prism. • Aperture dial: This has got various apertures such as cobalt blue filter, fixation star, small spot, large spot, pinhole, hemispot and alit. These have a specific function each. • Reflecting mirror/prism: This is a mirror angled at 45 degrees which is partially reflecting or has a central peephole. It makes the light cone projected upon the patients eye appear as if it has originated from the mirror itself. Most modern ophthalmoscopes utilize a prism in place of a mirror for this purpose. Apertures Viewing system • Condensing Lens: These are aspheric lens with ranges varying with every ophthalmoscope model. Eg. +1-10, +15, +20,+40 and -1-10,-15,-20,-25,-35 in the Heine beta 200. • Viewing window: Recessed, antireflective coated to avoid glare. • Polarizing/red free filter: This is mounted on a separate dial and enables green, red free image viewing of the fundus or a polarized view to detect nerve fibre layer. The why, what and how of direct ophthalmoscopy? Why? Why direct? It is a direct ophthalmoscope as the image forms directly on the retina and there is no intermediate image akin to that seen in an indirect ophthalmoscope. Why ophthalmoscope? It is indeed interesting to wonder why this instrument came to be called as an ophthalmoscope since the term ophthalmology was coined a good deal after the invention of the ophthalmoscope by Helmholtz in 1851. It is quite clearly argued in essays written in the nineteenth century that instruments and developing technology such as ophthalmoscope and laryngoscopes actually led to the development of the respective specializations. Of course eye Vol. 21, No. 3, January-March, 2011 What are all the knobs for? Light intensity adjustment dial: This helps provide an illumination of variable intensity for eliminating the corneal reflex and patient comfort. Small spot This provides approximately a five degrees cone and is used for a small pupil. It also helps decrease corneal reflexes and increases patient comfort. Large spot This provides an approximately eight to ten degrees illuminated circle (though highly dependent on the refractive status and papillary diameter). Macular spot/pinhole This provides a small spot to observe only the fovea/macula without any undue light thereby minimizing patient discomfort and enabling viewing through a 1-2mm pupil. Hemi-spot Reduces corneal reflex and provides retinal depth perception. Slit Accurate assessment of retinal elevations and depressions. Assessment of anterior chamber depth. Cobalt blue spot Examination of corneal abrasions and scarring Fixation star (with polar coordinates) Accurate eccentric fixation testing, disc assessment and retinal mapping. Red free filter This may be combined with all filters. Contrasts features by removing red colour and thus betters visualization of blood vessels, hemorrhages and nerve fibre layer. Some ophthalmoscopes may have a polarized filter to better evaluate nerve fibre defects. Condensing/focusing lens They help focus the image onto the observers retina. Need to be selected based on the subjects refractive status and distance at which ophthalmoscopy is done. What are the image properties? The image formed by an ophthalmoscope is virtual, erect and magnified. The area of retina imaged varies between 6.5 to 10 degrees. (Average area subtended by disc is 7 degrees vertical and 5.5 degrees horizontal; thus an average sized disc should just fit the 5 degree cone of ophthalmoscope) DJO 41 Delhi Journal of Ophthalmology How does the ophthalmoscope function? Fundamental Optics The ray diagram of the direct ophthalmoscope is shown below. It also depicts the usage of condensing lenses for eyes with refractive error[2]. (Figure 4) Understanding your Direct Ophthalmoscope When the ophthalmoscopy is being done from very close to the eye, the distance is less than f causing a virtual erect image to be seen. Magnification To understand how the ophthalmoscope magnifies, we take the example of an emmetropic eye. First we examine a small segment of a retinal vessel from 25 cm (the comfortable near vision distance). Let us suppose it subtended an angle of q0. We now view the same vessel segment from very close to the eye. Assuming the eye as a reduced lens of power 60D, we now are seeing from within the focal length of this lens thus we see a virtual erect image. On extrapolating this image to 25cm distance, you can observe that it is much larger and subtends an angle of q10. Thus we observe an angular magnification and no linear magnification. M ang= q10/ q0 = distance(d) × power(D)= 0.25 × 60.This is equal to 15. (Figure 7) Figure 4: Ray diagram depicting optics of ophthalmoscope Image Properties The image properties depend on the working distance used for ophthalmoscopy. When done at a distance of 25 cm for distant direct examination, we observe a real inverted unmagnified image of the fundus as shown in Figure5. 1 A object (upright arrows) at 25 cm subtends angle q at unaided observer’s eye. B Virtual Image (Large grey Arrow) of the same object subtends angle Figure 5: Image properties during distant direct ophthalmoscopy When the fundoscopy is done from a very near distance to the subject’s eye, the image is a virtual erect one.(Figure 6) Figure 6: Image properties while viewing fundus during close range ophthalmoscopy. This image changes from a real to virtual may be understood with a basic knowledge of optics. The focal length of the reduced eye model is 1.67 cm. The retina therefore lies between f and 2f. When we do a distant direct ophthalmoscopy, we are observing the image from distance between 2f and infinity as also, the light source is originating from this point. This thus gives a real inverted image forming on the observer’s eye. DJO 42 q1 when viewed. Figure 7: Image depicting magnification property of ophthalmoscope Field of view The field of view seen in a direct ophthalmoscope varies with the distance at which the examination is carried out and the pupil diameter. For example, if we observe the fundus from a distance of 15 cm in a 2mm pupil, then we can only see an area of about 200-300µ or a short segment of a vessel. In contrast on observing from very close to the eye in a well dilated pupil (8mm), we can see more than 10degrees of field. Theoretically it may be possible to see up to the equator in a fully dilated pupil in a cooperative patient on moving the ophthalmoscope and patients eyes appropriately. How to perform a complete ophthalmoscopic examination? Steps Before proceeding, it is important to understand the instrument well. The first step in the use of an ophthalmoscope is to do Vol. 21, No. 3, January-March, 2011 Delhi Journal of Ophthalmology Understanding your Direct Ophthalmoscope examination at 1m distance. This sheds light on any abnormalities of the eyelids, orbit and periorbita as well as highlights any obvious ocular deviations. This should be followed by a distant direct examination at 22-25cm( a comfortable near vision distance). Some ophthalmologists prefer to do this at a closer distance of 10cm as it gives better details. If the examination is done at 10cm, we should select a +10D condensing lens to view the best glow. At 25 cm, a +4D lens may be used. This examination shows a red reflex and highlights any opacities in the media as black images. The patient may then be asked to look in the four cardinal gazes and the movement of the opacity noted. Movement against the ocular movement means the opacity is behind the nodal point of the eye (i.e. in the lens or vitreous) while a movement with would indicate corneal or anterior segment opacity. The distant direct examination is also used to examine the lens, iris, cornea and adnexa. Any squint in a child may be picked up due to an unequal reflex (Bruckner’s test). The presence of an RAPD can also come forth in this step. The third step involves moving closer to the patient and correspondingly increasing the power in the condensing lens to examine in detail the magnified anterior segment structures. The fourth step entails reducing the condensing lens power such that any part of the retina comes into focus. While reducing the power, the vitreous cavity will come into focus and any pathology in it may be seen. Once the retina is focused, we may localize any blood vessel and follow it backwards against the branching pattern to reach the optic disc. Then move temporally from the disc to reach the macula. We can ask the patient to look into the light and the fovea will come into focus. The blood vessels can be traced into the periphery from the disc to reach second and third order vessels. This completes the posterior pole examination to examine the periphery, we ask the patient to look in the four cardinal gazes while continuing to focus the retina. The ophthalmoscope illuminated cone may be moved to further our view into the peripheral retina. Practical tips • • • • To eliminate the irritating corneal reflex, one can slightly tilt the ophthalmoscope and view obliquely. One can also decrease the illumination intensity and use a smaller aperture. Corneal reflex is also negated if the patient is approached from 15 degrees rather than from straight ahead. Use a small aperture for a smaller pupil as only an illuminated cone equal to the size of the pupil can enter or exit the eye while the rest will reflect off the iris creating unnecessary glare and poor contrast. The fovea lies 3 degrees temporal to the optical axis of the eye, the disc lies 10 degrees nasal and the peripheral Vol. 21, No. 3, January-March, 2011 • • • • • • • retina commences about 16 degrees temporal to it. Thus, if the patient is seeing straight ahead, then we know how much to tit the ophthalmoscope to view these landmarks. The patient should be asked to look straight ahead into the distance or preferably to a target on a far off wall. The patient should be instructed to stay steady and frequently blink during the examination. The examiner should use his right eye to view the patient’s right eye and vice versa. They should keep their opposite hand on the patient’s forehead to support and steady it. The examiner should keep both their eyes open during examination and imagine as if the retina is at 6 meters to prevent accommodation. Normally, the examiner should continue to wear his glasses while the patient has to remove his. The field of view decreases if the examiner wears his glasses therefore for low myopes or hyperopes (± 3Ds) and astigmats (below 2.5Dc) may remove their glasses especially in a small pupil. A trick to decide the appropriate selection of the condensing lens is described as follows. Observe the light reflex on the retinal vessels. If a white line is seen then either the patient is emmtropic or hyperopic. In that case, add plus lens and the highest plus when the line reflex disappears is the appropriate power. This would also be the approximate refractive error of the patient if the examiner had not accommodated. If there is no line of light reflex on the vessels, then the patient is myopic. Add minus power and the smallest minus lens when the reflex appears is the refractive error of the patient. The lenses of the ophthalmoscope can be used to focus variously the apex and base of any intraocular mass and thus helps determine its height in dioptres. How to select an appropriate ophthalmoscope? The ophthalmoscope selection should be guided by a number of factors. Prime among these is the intended clinical role. For a physician who needs to evaluate whether a fundus is normal or abnormal, a basic design should suffice while an ophthalmologist should look for one with highest quality optics and maximum functionality for accurate diagnosis. The ophthalmoscope should have apertures such as the small and large spot, cobalt blue filter, slit and the fixation star. Presence of a green filter is mandatory for diagnostic purposes. The instrument should contain adequate number of focusing lenses with a 1 dioptre minimum count for fine focusing. The battery should preferably be rechargeable Li ion or NiMH which provide extended power. Beyond this minimum specifications, any of the advanced machines may be used. How to Care for the direct ophthalmoscope? The direct ophthalmoscope is a sturdy built instrument for DJO 43 Delhi Journal of Ophthalmology heavy handling but requires proper care for its longevity. The following precautions should be observed: • The battery should be fully discharged and recharged once every few months to maximize battery life. • After fully charging the battery, the bulb should first be switched on at sub-maximal illumination for 1-2 cases before employing full illumination to maximize bulb life. • Use only genuine bulbs and replace in accordance with the owner’s manual instructions. • The condensing lenses are stuck to the dial using glue which is soluble in acetone and related solvents. Therefore never use these to clean your ophthalmoscope. • The ophthalmoscope may be cleaned using mild alcohol or detergent and a soft cloth. • A cotton bud should be used to clean the viewing window and aperture window in a circular sweeping manner. • Ophthalmoscopes come with twist and fit as well as automatic lock heads. Ascertain the head connector in the scope and fix head accordingly. • Always store the ophthalmoscope in ints case when not in use. If it will be unused for a long time, remove the battery and store. • Dispose the NiMH or Li ion battery appropriately. possible but not mutually interfering. This gives a larger view in smaller pupils as well as eliminates corneal reflex artifacts. Apart from this the incorporation of aspheric designs in lenses has led to decreased aberrations and reflex artifacts. Battery life has been greatly enhanced with the modern NiMH or Li ion batteries while their size and weight has more than halved. This has enabled manufacture of Pocket sized or mini ophthalmoscopes which have an added convenience factor. Further advancements are underway to add better and more functionality to this principal tool of every clinician. Conclusion Innovations in direct ophthalmoscopes The direct ophthalmoscope has an immense contribution in furthering the development of ophthalmology as a specialty science. Familiarity with the use of this instrument would go a long way in aiding the diagnosis of diseases by physicians and ophthalmologists alike. Although technology has brought the ophthalmoscope a long way from its humble beginnings, one should realize that like every instrument, it too has its limitations. These include the limited field of view, poor image visibility through hazy media, inability to appreciate the full picture, a high need for patient cooperation and non stereoscopic viewing among others. If we works bearing these in mind, we are unlikely to get mislead by false signs and would gain a lot more from this brilliant instrument. The direct ophthalmoscope has come a long way from the polished mirror made by Babbage or the more practical model of Helmholtz. Illumination technology has shifted from the use of a gas flame as an external source of illumination to the first directly illuminated ophthalmoscope made in 1915 to the current day instruments using halogen and xenon bulbs. The viewing systems have improved drastically over time. The latest innovations include the panoptic ophthalmoscope which uses axial point source optics whereby the light is focused at a point on the cornea before moving onwards into the eye. This enables a wider field of view (up to 5 times wider) in smaller pupils. Another leap forward is the use of advanced coaxial optics where the illumination and viewing is done along the same path of light keeping them as close as References 1. Keeler CR. Babbage the Unfortunate..Br J Ophthalmol 2004;88:730-732. 2. Timberlake GT, Kennedy M.The Direct Ophthalmoscope:How it Works and How to Use It. 2005. University of Kansas Press. 3. Silvester A. The emergence of medical specialties in the nineteenth century: a discussion of the historiography. History of Medicine online 2010 Priory.com publication 4. Instruction user manual of Heine Beta200 ophhalmoscope. 5. Ghosh S, Collier A, Varikarra M, Palmer S. Fundoscopy made easy. 2010. Churchill livingstome Elsevier. 1-21. 6. Fisher WA. Ophthalmoscopy, Retinoscopy and Refracion. 1937:1-34. DJO 44 Understanding your Direct Ophthalmoscope Vol. 21, No. 3, January-March, 2011