Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
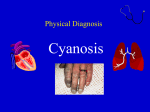
CYANOSIS INTRODUCTION Cyanosis refers to a bluish color of the skin and mucous membranes resulting from an increased amount of reduced hemoglobin, or of hemoglobin derivatives, in the small blood vessels of those areas. It is usually most marked in the lips, nail beds, ears, and malar eminences. The florid skin characteristic of polycythemia vera (Chap. 309) must be distinguished from the true cyanosis discussed here. A cherry-colored flush, rather than cyanosis, is caused by carboxyhemoglobin (Chap. 395). The degree of cyanosis is modified by the quality of cutaneous pigment and the thickness of the skin, as well as by the state of the cutaneous capillaries. The accurate clinical detection of the presence and degree of cyanosis is difficult, as proved by oximetric studies. In some instances, central cyanosis can be detected reliably when the arterial saturation has fallen to 85 percent; in others, particularly in dark-skinned persons, it may not be detected until the saturation has declined to 75 percent. The increase in the quantity of reduced hemoglobin in the cutaneous vessels which produces cyanosis may be brought about either by an increase in the quantity of venous blood in the skin as the result of dilatation of the venules and venous ends of the capillaries or by a reduction in the oxygen saturation in the capillary blood. In general, cyanosis becomes apparent when the mean capillary concentration of reduced hemoglobin exceeds 5 g/dL. It is the absolute rather than the relative quantity of reduced hemoglobin which is important in producing cyanosis. Thus, in a patient with severe anemia, the relative amount of reduced hemoglobin in the venous blood may be very large when considered in relation to the total amount of hemoglobin. However, since the concentration of the latter is markedly reduced, the absolute quantity of reduced hemoglobin may still be small, and therefore patients with severe anemia and even marked arterial desaturation do not display cyanosis. Conversely, the higher the total hemoglobin content, the greater is the tendency toward cyanosis; thus patients with marked polycythemia tend to be cyanotic at higher levels of arterial oxygen saturation than patients with normal hematocrit values. Likewise, local passive congestion, which causes an increase in the total amount of reduced hemoglobin in the vessels in a given area, may cause cyanosis. Cyanosis also is observed when nonfunctional hemoglobin such as methemoglobin or sulfhemoglobin (Chap. 306) is present in blood. Cyanosis may be subdivided into central and peripheral types. In the central type, there is arterial blood unsaturation or an abnormal hemoglobin derivative, and the mucous membranes and skin are both affected. Peripheral cyanosis is due to a slowing of blood flow to an area and abnormally great extraction of oxygen from normally saturated arterial blood. It results from vasoconstriction and diminished peripheral blood flow, such as occurs in cold exposure, shock, congestive failure, and peripheral vascular disease. Often in these conditions the mucous membranes of the oral cavity or those beneath the tongue may be spared. Clinical differentiation between central and peripheral cyanosis may not always be simple, and in conditions such as cardiogenic shock with pulmonary edema there may be a mixture of both types. DIFFERENTIAL DIAGNOSIS (See Table 32-2) Central cyanosis Decreased arterial oxygen saturation results from a marked reduction in the oxygen tension in the arterial blood. This may be brought about by a decline in the tension of oxygen in the inspired air without sufficient compensatory alveolar hyperventilation to maintain alveolar oxygen tension. Cyanosis does not occur to a significant degree in an ascent to an altitude of 2500 m (8000 ft) but is marked in a further ascent to 5000 m (16,000 ft). The reason for this becomes clear on studying the S shape of the oxygen dissociation curve (Fig. 302-4). At 2500 m (8000 ft) the tension of oxygen in the inspired air is about 120 mmHg, the alveolar tension is approximately 80 mmHg, and the hemoglobin is nearly completely saturated. However, at 5000 m (16,000 ft) the oxygen tensions in atmospheric air and alveolar air are about 85 and 50 mmHg, respectively, and the oxygen dissociation curve shows that the arterial blood is only about 75 percent saturated. This leaves 25 percent of the hemoglobin in the reduced form, an amount likely to be associated with cyanosis in 1 the absence of anemia. Similarly, a mutant hemoglobin with a low affinity for oxygen (e.g., Hb Kansas) causes lowered arterial oxygen saturation and resultant central cyanosis (Chap. 306). Seriously impaired pulmonary function, through alveolar hypoventilation or perfusion of unventilated or poorly ventilated areas of the lung, is a common cause of central cyanosis (Chap. 214). This may occur acutely, as in extensive pneumonia or pulmonary edema, or with chronic pulmonary diseases (e.g., emphysema). In the last situation polycythemia is generally present, and clubbing of the fingers may occur. However, in many types of chronic pulmonary disease with fibrosis and obliteration of the capillary vascular bed, cyanosis does not occur because there is relatively little perfusion of underventilated areas. Another cause of decreased arterial oxygen saturation is shunting of systemic venous blood into the arterial circuit. Certain forms of congenital heart disease are associated with cyanosis (Chap. 199). Since blood flows from a higher-pressure to a lower-pressure region, in order for a cardiac defect to result in a right-toleft shunt, it must ordinarily be combined with an obstructive lesion distal to the defect or with elevated pulmonary vascular resistance. The most common congenital cardiac lesion associated with cyanosis in the adult is the combination of ventricular septal defect and pulmonary outflow tract obstruction (tetralogy of Fallot). The more severe the obstruction, the greater the degree of right-to-left shunting and resultant cyanosis. The mechanisms for the elevated pulmonary vascular resistance which may produce cyanosis in the presence of intra- and extracardiac communications without pulmonic stenosis (Eisenmenger syndrome) are discussed elsewhere (Chap. 199). In patients with patent ductus arteriosus, pulmonary hypertension, and right-to-left shunt, differential cyanosis results; i.e., cyanosis occurs in the lower but not in the upper extremities. Pulmonary arteriovenous fistulas may be congenital or acquired, solitary or multiple, microscopic or massive. The degree of cyanosis produced by these fistulas depends on their size and number. They occur with some frequency in hereditary hemorrhagic telangiectasia. Arterial oxygen unsaturation also occurs in some patients with cirrhosis, presumably as a consequence of pulmonary arteriovenous fistulas or portal vein-pulmonary vein anastomoses. In patients with cardiac or pulmonary right-to-left shunts, the presence and severity of cyanosis depend on the size of the shunt relative to the systemic flow as well as on the oxyhemoglobin saturation of the venous blood. In patients with central cyanosis due to arterial oxygen unsaturation, the severity of cyanosis increases with exercise. With increased extraction of oxygen from the blood by the exercising muscles, the venous blood returning to the right side of the heart is more unsaturated than at rest, and shunting of this blood or its passage through lungs incapable of normal oxygenation intensifies the cyanosis. Also, since the systemic vascular resistance normally decreases with exercise, the right-to-left shunt is augmented by exercise in patients with congenital heart disease and communications between the two sides of the heart. Secondary polycythemia occurs frequently in patients with arterial unsaturation and contributes to the cyanosis. Cyanosis can be caused by small amounts of circulating methemoglobin and by even smaller amounts of sulfhemoglobin (Chap. 306). Although they are uncommon causes of cyanosis, these abnormal hemoglobin pigments should be sought by spectroscopy when cyanosis is not readily explained by malfunction of the circulatory or respiratory systems. Generally, clubbing does not occur with them. The diagnosis of methemoglobinemia can be suspected, if, on mixing the patient's blood in a test tube and exposing it to air, it remains brown. Peripheral cyanosis Probably the most common cause of peripheral cyanosis is generalized vasoconstriction resulting from exposure to cold air or water. This is a normal response. When cardiac output is low, as in severe congestive heart failure or shock, cutaneous vasoconstriction occurs as a compensatory mechanism, so blood is diverted from the skin to more vital areas such as the central nervous system and heart (Chap. 195), and intense cyanosis associated with cool extremities may result. Even though the arterial blood is normally 2 saturated, the reduced volume flow through the skin and the reduced oxygen tension at the venous end of the capillary result in cyanosis. Arterial obstruction to an extremity, as with an embolus, or arteriolar constriction, as in cold-induced vasospasm (Raynaud's phenomenon; Chap. 211), generally results in pallor and coldness, but there may be associated cyanosis. If there is venous obstruction and the extremity is congested, as with stagnation of blood flow, cyanosis is also present. Venous hypertension, which may be local (as in thrombophlebitis) or generalized (as in tricuspid valve disease or constrictive pericarditis), dilates the subpapillary venous plexuses and thereby intensifies cyanosis. APPROACH TO THE PATIENT WITH CYANOSIS Certain features are important in arriving at the proper cause of cyanosis: 1 The history, particularly the duration (cyanosis present since birth is usually due to congenital heart disease), and possible exposure to drugs or chemicals which may produce abnormal types of hemoglobin. 2 Clinical differentiation of central as opposed to peripheral cyanosis. Objective evidence by physical or radiographic examination of disorders of the respiratory or cardiovascular systems. Massage or gentle warming of a cyanotic extremity will increase peripheral blood flow and abolish peripheral but not central cyanosis. 3 The presence or absence of clubbing of the fingers (see below). Clubbing without cyanosis is frequent in patients with infective endocarditis and in association with ulcerative colitis; it may occasionally occur in healthy persons, and in some instances it may be occupational, e.g., in jackhammer operators. Slight cyanosis of the lips and cheeks, without clubbing of the fingers, is common in patients with mitral stenosis and is probably due to minimal arterial hypoxia resulting from fibrotic changes in the lungs secondary to long-standing congestion combined with reduction of cardiac output (Chap. 201). The combination of cyanosis and clubbing is frequent in patients with certain types of congenital cardiac disease and is seen occasionally in persons with pulmonary disease such as lung abscess or pulmonary arteriovenous shunts. On the other hand, peripheral cyanosis or acutely developing central cyanosis is not associated with clubbed fingers. 4 Determination of arterial blood oxygen tension or oxygen saturation, spectroscopic and other examinations of the blood for abnormal types of hemoglobin. CLUBBING The selective bullous enlargement of the distal segments of the fingers and toes due to proliferation of connective tissue, particularly on the dorsal surface, is termed clubbing; an increase occurs in the sponginess of the soft tissue at the base of the nail. Clubbing may be hereditary, idiopathic, or acquired and associated with a variety of disorders, including cyanotic congenital heart disease, infective endocarditis, and a variety of pulmonary conditions (among them primary and metastatic lung cancer, bronchiectasis, lung abscess, cystic fibrosis, and mesothelioma), as well as with some gastrointestinal diseases (including regional enteritis, chronic ulcerative colitis, and hepatic cirrhosis). Clubbing in patients with primary and metastatic lung cancer, mesothelioma, bronchiectasis, and hepatic cirrhosis may be associated with hypertrophic osteoarthropathy. In this condition, the subperiosteal formation of new bone in the distal diaphyses of the long bones of the extremities causes pain and symmetric arthritis-like changes in the shoulders, knees, ankles, wrists, and elbows. The diagnosis of hypertrophic osteoarthropathy may be confirmed by bone radiographs and scans. Although the mechanism of clubbing is unclear, it appears to be secondary to a (presumably humoral) substance which causes dilation of the vessels of the fingertip. 3