Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
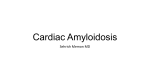
A CHANGE OF HEART: PROGRESSIVE EDEMA IN AN ELDERLY MAN Meghan Gilroy, MD and Jeffrey Southard, MD University of California, Davis Medical Center, Sacramento, CA A A • The systemic amyloidoses are a rare group of diseases caused by diffuse extracellular deposition of proteinacious material • Amyloid light-chain amyloidosis is characterized by multiorgan involvement • Cardiac involvement carries a poor prognosis B A 77 year-old man with a significant cardiac history presented to his cardiologist with new-onset lower extremity edema. Despite oral diuresis, edema progressed to anasarca and the patient was admitted for IV diuresis. ROS: edema, orthopnea, fatigue, jaw claudication, neck pain, difficulty elevating his head B Figure 1. Echocardiographic images from our patient demonstrating hypergranularity of myocardium. (A) Parasternal long axis view showing left atrial enlargement. (B) Apical four-chamber view showing biatrial enlargement. Figure 2. Echocardiographic m-mode data from our patient demonstrating (A) reduced E/A indicating diastolic dysfunction and (B) septal tissue doppler with low amplitude E’ wave suggesting restriction. A PMH: CAD s/p CABG, paroxysmal atrial dysrhythmia, diastolic heart failure, hypertension, hypothyroidism, CKD, anemia PE: JVP 9cm, irregularly irregular heart rhythm, decreased breath sounds at bilateral lung bases, severe pitting edema of the lower extremities and scrotum Laboratory: Cr 2.03 mg/dL Hgb 10.1 g/dL BNP 2122 pg/mL Troponin <0.01 Imaging: CXR: pulmonary edema, R pleural effusion Echo: elevated PA pressure, biatrial enlargement, LVH, E/A 1.2 (Figures 1 & 2) Cardiac cath: elevated RA pressure, elevated RV EDP (Figure 3) Tissue: Endomyocardial biopsy: Congo Red- postive, birefringent Mass spectrometry: kappa-type amyloid Bone marrow biopsy: plasma cell dyscrasia B Figure 3. Right sided cardiac catheterization from our patient showing (A) elevated right atrial pressure and (B) elevated right ventricular end-diastolic pressure with “square root sign” suggesting restrictive physiology. A B Cardiac catheterization was performed which suggested restrictive cardiomyopathy. Endomyocardial biopsy stained positive for amyloid. Bone marrow biopsy suggested light-chain amyloidosis. Despite diuresis, the patient remained fluid overloaded and renal failure progressed. As light-chain subtype was not confirmed until later in clinical course, the patient was not treated for amyloidosis. While in the hospital he developed wide complex tachycardia, which led to cardiac arrest. Autopsy revealed marked cardiomegaly (720gm) with biventricular hypertrophy. Histology showed amyloid deposition in the heart, kidneys, thyroid, temporal artery, and strap muscles of the neck. AL amyloidosis is a rare plasma cell dyscrasia in which monoclonal immunoglobulin light chains form amyloid precursors; incidence is 8.9 cases per million person-years1. Cardiac involvement is present in approximately 60% of patients and can cause ventricular hypertrophy, pericardial and pleural effusions, granular-appearing myocardium on echocardiography, and low-voltage EKG1,2,4. Once heart failure develops, median survival is less than six months3. Early diagnosis and treatment is paramount for reversal of organ damage1. Treatment options include melphalan, dexamethasone, stem cell transplant, and heart transplant2,3. Endomyocardial biopsy proved amyloidosis as the etiology for heart failure in our patient. Autopsy suggested extensive systemic involvement (Figure 4). Amyloidosis is an important component of the differential for heart failure when the etiology is uncertain, particularly in the setting of multiorgan dysfunction. C D Figure 4. Photomicrographs from our patient’s autopsy including (A) cardiac tissue stained with Congo Red; (B) cardiac tissue under polarized light; (C) kidney tissue stained with Congo Red; (D) kidney tissue under polarized light. 1. Merlini G, Seldin DC, Gertz MA. Amyloidosis: pathogenesis and new therapeutic options. J Clin Onc 2011;29(14):1924-33. 2. Kapoor P, Thenappan T, Singh E, Kumar S, Geipp PR. Cardiac amyloidosis: a practical approach to diagnosis and management. Am J Med 2011;124:1006-15. 3. Cohen AD and Comenzo RL. Systemic light-chain amyloidosis: advances in diagnosis, prognosis, and therapy. Hematology Am Soc Hematol Educ Program 2010;2010:287-94. 4. Apridonidze T, Steingart RM, Comenzo RL, Hoffman J, Goldsmith Y, Bella JN, Landau H, Liu JE. Clinical and echocardiographic correlates of elevated troponin in amyloid light-chain cardiac amyloidosis. Am J Cardiol 2012 Jul 5 [Epub ahead of print]. ACKNOWLEDGEMENT: We would like to thank Christina DiLoreto of the UCDMC pathology department for her asistance with tissue photomicrographs.