Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
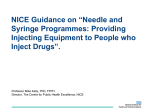
Recent policy developments and research about effective interventions for injecting drug users. Vilnius, November 2009 Zhannat Kosmukhamedova, HIV Unit HIV and injecting drug use: restatement of the priority area Estimated Number of People who Inject Drugs: 1,044,000 15,861,500 3,476,500 247,000 2,270,500 3,957,500 2,018,000 1,778,500 (Source : UN Reference group for IDUs,2008) 173,500 Slide 2 HIV and injecting drug use: restatement of the priority area Estimated Number of People who Inject Drugs: 15,861,500 2,997,500 Estimated Number of HIV Positive Among them: 940,000 29,000 347,000 114,000 661,000 580,500 221,000 (Source : UN Reference group for IDUs, 2008) 2,500 Slide 3 Why the area is important? Injecting Drug Use were reported in 148 countries HIV infections among People who Inject Drugs - in 120 countries 92 countries support harm reduction in policy or practice 71 countries have an explicit supportive reference to harm reduction in national policy documents HIV prevention service coverage - below 10 % 92% of people who inject drugs in low- and middle income countries have no access to HIV prevention services of any kind (Source : UN Reference group for IDUs, 2008) Slide 4 Evidence informed HIV services 1961 Single Convention on Narcotic Drugs; 1971 Convention on Psychotropic Substances and 1988 UN Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances, and the commitment to achieving universal access to HIV prevention, treatment, care and support by 2010, including for people who inject drugs Slide 5 Injecting drug use - in 148 countries; HIV/IDUs – 120 countries Global Availability of Pharmacological Treatment 63 countries have Pharmacotherapy Slide 6 Injecting drug use - in 148 countries; HIV/IDUs – 120 countries WHO European Region: Availability of PT buprenorphine diamorphine codeine injectable methadone methadone slow-release morphine Slide 7 Injecting drug use - in 148 countries; HIV/IDUs – 120 countries EU: Availability of PTM Slide 8 Injecting drug use - in 148 countries; HIV/IDUs – 120 countries EU: Availability of PT in prison 37 countries have PT in prison Slide 9 Injecting drug use - in 148 countries; HIV/IDUs – 120 countries Global: Availability of NSP 77 countries have needle and syringe programmes 10 countries have needle and syringe in prisons Slide 10 Injecting Drug Use were reported in 148 countries Only 61 low and middle income countries – HIV testing and counseling Only 14 % of PLWH in EE and CA (current or former drug users) – ART (Source : UN Reference group, 2008) Slide 11 Obstacles: why it is not working • • • • • • • • • • • • Poor availability of harm reduction measures (abstinence-only mentality) Poor accessibility and quality of services Restrictive inclusion criteria Lack of gender responsive Lack of confidentiality and protection of personal information Punitive policies and legislation Harassment by law enforcement personnel Drug user as “a criminal” keeps people away from services Increased prison populations - higher risk of HIV infection Ineffective spending – focus on criminalizing, not treating Absence of political and societal support, Stigma, discrimination and violation of human rights… Slide 12 What is working well and should be expanded Commission on Narcotic Drugs (CND, 52 states), UNAIDS Programme Coordinating Board (PCB, 22 states) and the United Nations Economic and Social Council (ECOSOC,54 members) in 2009: a common understanding in the UN on what is a comprehensive package of HIV services for injecting drug users (harm reduction). UNAIDS, WHO and UNODC recommend: - Needle and syringe programmes - Pharmacological treatment - Anti-retroviral therapy - Voluntary HIV counselling and testing - Prevention and treatment of STIs - Condom programing; - Targeted information, education and communication - Hepatitis diagnosis, treatment and vaccination - TB prevention, diagnosis and treatment. Source: WHO,UNODC,UNAIDS Technical Guide for countries to set targets for universal access to HIV prevention, treatment and care for IDUs, 2008 Slide 13 WHO study on OST and HIV/AIDS, 2008 Aim: to examine effectiveness of OST in China, Ukraine, Indonesia, Thailand, Lithuania, Poland, Iran, Australia. Findings: 70% treatment retention rate after 6 months with significant reductions in reported heroin and other illicit opioid use. WHO/UNAIDS/UNODC position paper on Substitution treatment (2004) ‘…IDUs who do not enter treatment are up to six times more likely to become infected with HIV than injectors who enter and remain in treatment.’ Slide 14 Universality of OST effectiveness BBV-TRAQ injecting risk score The WHO Collaborative Study on Substitution Therapy of Opioid Dependence and HIV/AIDS - injecting risk behaviour 25 China 20 Indonesia 15 Thailand Iran 10 Australia 5 Lithuania Poland 0 Ukraine Baseline 3-month 6-month Slide 15 Substitution treatment: Societal outcomes Substitution treatment: Societal outcomes - Associated with improved social functioning and employment. - Substantial reductions in criminal activity. - 4 to 7 fold savings in reduced drug-related crime, criminal justice costs and theft alone. - No evidence for increased drug use in community. Sources : 1WHO/UNODC/UNAIDS position paper: Substitution maintenance therapy in the management of opioid dependence and HIV/AIDS prevention (WHO, 2004) 2WHO/UNOC/UNAIDS: Effectiveness of Drug Dependence Treatment in Preventing HIV among Injecting Drug Users, Geneva 2005 Slide 16 New research on effectiveness of NSP Over 30 million needles and syringes have been distributed every year in Australia since 2000. A recent study estimates that this intervention has directly prevented more than 32,000 cases of HIV infection and almost 100,000 cases of hepatitis C. For every Australian dollar spent on NSPs, four were returned. Source: UNSW’s National Centre in HIV Epidemiology and Clinical Research, Return on Investment 2: Evaluating Slide 17 the cost-effectiveness of needle and syringe programs in Australia), 2009 ‘…we have evidence that effective programmes for harm reduction and substitution therapy can save billions of dollars. During this crisis, UNAIDS will champion these and other evidence informed prevention programmes as smart investments for saving money, saving lives and restoring health and dignity to people.’ Michele Sidibe, UNAIDS Executive Director, PCB June 2009 speech Slide 18 Thank you www.unodc.org www.who.int www.unaids.org Slide 19